SYMPTOMS AND PHYSICAL SIGNS SURGICAL DISEASES OF THE











































: Protrusion of the membranes that cover the spine and part of the")
 is called")
 protruding through the spinal")

































- Slides: 84
SYMPTOMS AND PHYSICAL SIGNS SURGICAL DISEASES OF THE HEAD LIDIA IONESCU The IIIrd. Surgical Unit
SURGICAL DISEASES DIAGNOSIS HYSTORY CLINICAL EXAMINATION LAB. TESTS IMAGISTIC INVESTIGATIONS
Symptom- what the patient feels Physical sign- what the doctor finds at clinical examination of the patient’s segments. Symptom is subjective Physical sign is objective Clinical diagnosis = symptoms + signs Final diagnosis= symptoms + signs + lab. tests + investigations.
SURFACE LANDMARKS OF THE HEAD Nasion External occipital protuberance Vertex Superior nuchal line Mastoid process of the temporal bone Zygomatic arch Superficial temporal artery Facial artery Parotid duct
Surface landmarks
Sebaceous cysts Swelling - cystic mass - cystic tumor - lump Hairy parts of the body- scalp The mouth of the seb. gland opens into the hair follicle If blocked mouth, seb. gland becomes distended
Seb. Cyst History- slow growing Symptoms-a lump that gets scratched when the patient is combing the hair Such scratches may get infected If the cyst becomes infected it enlarges rapidly and becomes acutely painful
Seb. Cyst- examination-physical signs Position-hairy parts of the body Color- the skin overlying the cyst normal unless it is infected Tenderness- not tender unless infected Temperature-normal except when infected Shape- spherical Size- variable: mm-4 -5 cm. Surface- smooth Edge-well defined Composition- hard depending on the pressure in the cust “cheesy material”
Seb. cyst of the scalp Parietal region
Seb. cyst- lateral view
Seb. cyst of the scalp
Seb. cyst of the scalp
Surgical treatment- excision
Intact sebaceous cyst-specimen
Cut section- seb. cyst- “cheesy material”-sebum
Lipoma-case report A 59 -year-old woman was admitted with a 10 years' history of a painless swelling at the right thigh. The lesion became ulcerative over the past few months with mild pain. She had no significant medical and surgical history. Examination revealed normal vital signs, chest, heart, abdominal and rectal examinations.
Lipoma On local examination, a large mass occupying the posterior aspect of the lower two thirds of the right thigh was confirmed. There was an ulcerative lesion at the posteromedial aspect of the mass. The right popliteal artery was difficult to palpate, but the posterior tibial and dorsalis pedis were normal. There was no neuronal abnormality.
Lipoma- case report Blood tests showed normal blood count, liver function, urea and electrolytes as well as ESR. She had a normal chest and abdominal X-ray. The X-ray of the right thigh showed a soft tissue shadow and normal bone. Surgical excision was performed and the findings were consistent with a giant lipoma. The wound was closed easily as there was redundant skin because of the size of the mass. The weight of the specimen was 3. 2 kg.
Lipoma- case report The patient had an uneventful recovery and was discharged home with a very good condition. Histology of the specimen reported benign lipoma.
Huge lipoma of the thigh
Ulcerated lipoma on the postmedial thigh
Specimen- 3. 2 Kg.
Lipoma - a benign tumor of adipocyte origin. • The bright yellow color is typical of fat. • Note the lobulated appearance - typical of this lesion. • This particular tumor arose in the subcutaneous fat (note the small strip of skin ).
Case Report-lipoma A 60 year old male presented in out patient clinic with history of progressively increasing swelling in right thigh, which he noticed 3½ years back. Swelling was otherwise asymptomatic except that he had to wear loose fitting trousers. On examination, right thigh girth was grossly increased as compared to the left thigh.
Lipoma There were erythema ab agni over the medial aspect of both thighs (as is usual in Kashmiri people because of Kangri – “the fire pot”). The swelling was firm, non-tender and free from underlying structures.
Lipoma
CT scan of the right thigh was done which revealed a hypodense mass in the posterior compartment of the thigh beneath the hamstring muscles
Lipoma- case report FNAC of the swelling revealed mature fat cells, suggestive of lipoma. The patient was operated on under general anaesthesia, in prone position and the tumour was found beneath the hamstring muscles and was dissected out easily because of the capsule. Wound was closed in layers, leaving a suction drain inside the cavity. Healing progressed uneventfully. Histopathological examination revealed features consistent with lipoma. The tumour removed measured 21 x 17 x 14 cm in size and weighed 2, 95 Kg.
Specimen. Six months after surgery, the patient is symptom free and has no signs of recurrence
Lipoma is one of the commonest benign mesenchymal tumour in the body composed of mature adipose cells. It is found in almost all the organs of the body where normally fat exists. Most of the lipomas present as small subcutaneous swellings without any specific symptom.
Lipoma Giant lipomas, though rare, can present in thigh, shoulder or trunk. Clinical features of these giant lipomas are mainly because of their size which includes pain because of stretching of adjacent nerves, (restriction in movements of the part involved or social embarrassment because of mere size of the swelling). Definitive diagnosis of giant lipoma can be made only by histopathological examination.
Lipoma Surgery is the treatment of choice The dissection of these lipomas is usually easy because of a well defined capsule. Dead space created because of dissection of the giant lipomas is usually drained with the help of a suction drain to avoid collection.
LIPOMA
Surgical specimen
Hemangioma Benign skin lesion consisting of dense, usually elevated masses of dilated blood vessel. Benign neoplasm characterized by blood vascular channels. A cavernous hemangioma consists of large vascular spaces. A capillary hemangioma consists of many small blood vessels. A collection of dilated small vessels, 3 types: strawberry nevus, port-wine stains, spider nevus
Cavernous hemangioma
Hemangioma Congenital benign tumour made of blood vessels in the skin. Capillary hemangioma , an abnormal mass of capillaries on the head, neck, or face, is pink to dark bluish-red and even with the skin. Size and shape vary. It becomes less noticeable or disappears with age. Hemangioma simplex/strawberry mark, a reddish nub of dilated small blood vessels, enlarges in the first six months and may become ulcerated but usually recedes after the first year. Cavernous hemangioma, a rare, red-blue, raised mass of larger blood vessels, can occur in skin or in mucous membranes, the brain, or the viscera. Hemangiomas can often be removed by cosmetic surgery.
Strawberry hemangioma Intradermal, subdermal collection of dilated blood vessels Congenital lesion- present at birth Looks like a strawberry Often regress spontaneously in months/years after birth Rubbed or knocked they may ulcerate and bleed
Strawberry hemangioma
Physical examination Position- any part of the body- head/neck> Color- bright or dark red Shape- protrude from the skin surface Size- usually- 1 -2 cm. Surface-irregular Consistence- soft, compressible not pulsatile Relations- confined to the skin, freely mobile over the deep tissues
Port-wine stain-extensive intradermal hemangioma, mostly venous
PORT-WINE STAIN
Cavernous hemangioma on the tongue
Meningocele (MM): Protrusion of the membranes that cover the spine and part of the spinal cord through a bone defect in the vertebral column. MM is due to failure of closure during embryonic life of bottom end of the neural tube. The term spina bifida refers specifically to the bony defect in the vertebral column through which the meningeal membrane and cord may protrude (spina bifida cystica) or may not protrude so that the defect remains hidden, covered by skin (spina bifida occulta). The risk of MM (and all neural tube defects) can be decreased by the mother eating ample folic acid during pregnancy.
A birth defect involving an abnormal opening in the spinal bones (vertebrae) is called spina bifida. The spinal vertebrae have not formed and joined normally, leaving an opening
A defect which also includes a small, moist sac (cyst) protruding through the spinal defect, containing a portion of the spinal cord membrane (meninges), spinal fluid, and a portion of spinal cord and nerves is called a meningocele, myelomeningocele, or meningomyelocele
Surgical treatment is needed to repair the defect and is usually done within 12 to 24 hours after birth to prevent infection, swelling, and further damage. Under general anesthesia, an incision is made in the sac and some of the excess fluid is drained off. The spinal cord is covered with the membranes (meninges) and the skin is closed over the protruding meninges, spinal cord, and nerves.
The long-term result depends on the condition of the spinal cord and nerves. Outcomes range from normal development to paralysis (paraplegia). Infants may require about 2 weeks in the hospital after surgery.
Physical signs in head injury Examination of a case of recent head injury The patient is unconscious Examine the scalp for a wound or local bruising or hematoma Examine the nostrils and ears for evidence of blood diluted with CSF Compare the size of the pupils and test their reaction to light Make a general survey of the body for other injuries Search for paralysis Palpate and percuss the hypogastrium for evidence of an overfull bladder Temperature, pulse rate, RR-charted every half-hour
Head injury Radiographs of the skull should be taken at the first opportunity compatible with safety Brain injury is more likely in the presence of a skull fracture BUT skull fracture of itself does not indicate brain injury
COMA Coma is a state of absolute unconsciousness in which the patient does not respond to any stimulus Reflexes are absent, including the corneal and swallowing reflexes. Semi-coma- the patient responds only to painful stimuli and reflexes are present
Head injury The patient is conscious or semi-conscious Patient with skull fracture – hospital admission Close observation: PR, BP, RR, pupil size and reaction/ every ½ h. Signs of neurological deterioration: Falling pulse rate Reduced respiratory rate Falling GCS Dilatation of pupils Loss of light reaction or developing asymmetry of pupils
Complications of traumatic brain injury Cranial bleeding Cerebral hypoxia Infection Posttraumatic intracranial bleeding may be: - extradural - subdural - intracerebral CT of the brain documents the lesions Local brain compression- focal neurological effects - raised intracranial pressure
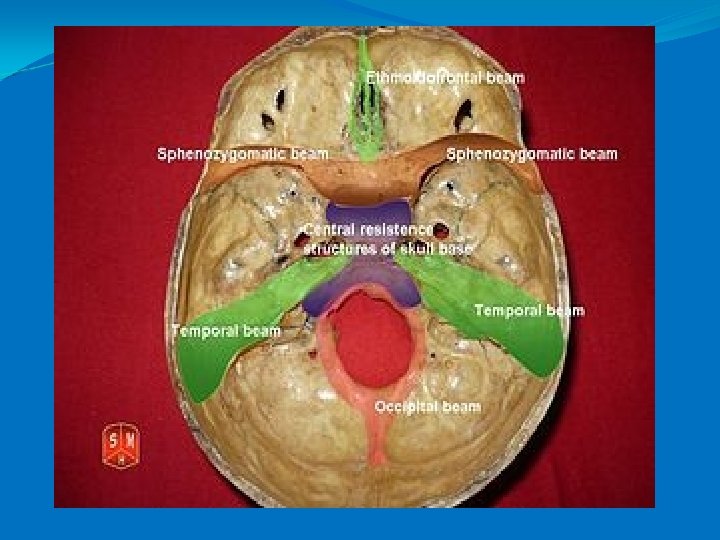
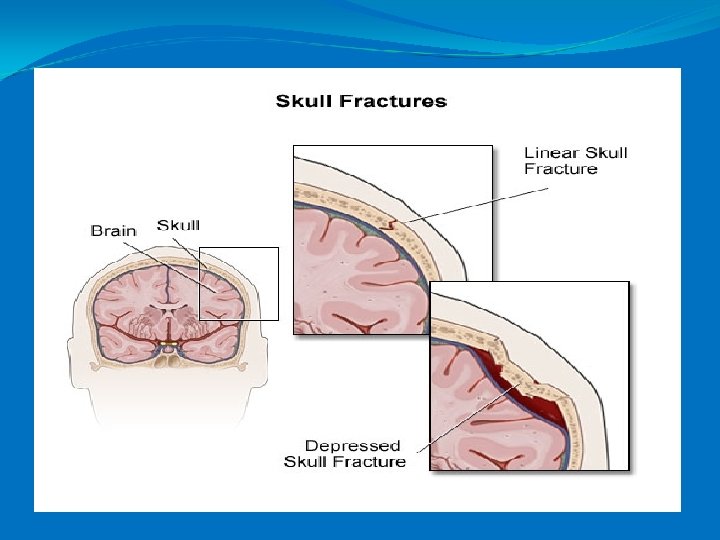
Types of skull fractures Liniar fractures - involve the skull vault, - overlying scalp bruising or swelling Depressed fractures - caused by blunt injuries, - the scalp is severely bruised Fractures of the base of the skull- anterior fossa - middle fossa - posterior fossa
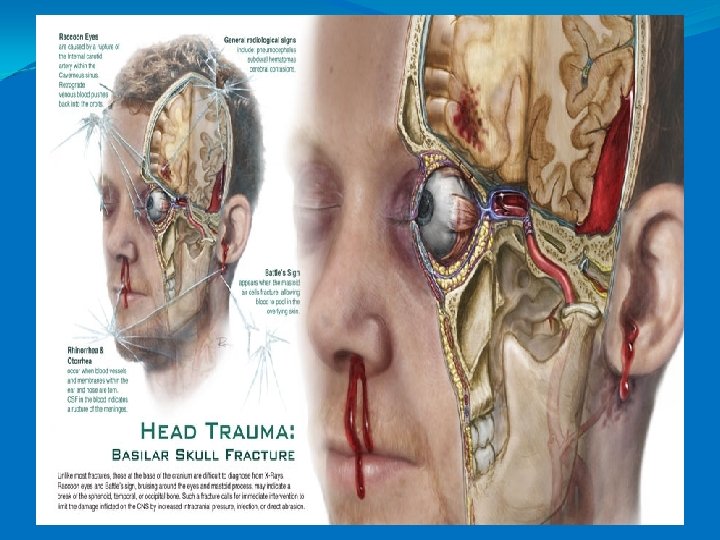
Basilar skull fractures a fracture of the base of the skull - the temporal, occipital, sphenoid and ethmoid bones. Such fractures can cause tears in the cerebral meninges - leakage of the cerebrospinal (CSF), hematoma formation and meningitis
Physical signs - pathognomonic for basilar skull fracture. 1. Otorrhea – leakage of CSF from the auditory canal 2. Leakage of CSF into the nasopharynx via the eustachian tube, causing a salty taste. 3. Rhinorrhea – leakage of CSF from the nasal passages 4. Hematoma presentation surrounding the orbits and ears as blood is flushed to the surface of the facial tissues. 5. Bleeding from the nose and ears 6. Deafness, nistagmus, vomitus 7. Battle’s sign is bruising over the mastoid sinus and is a delayed physical finding associated with basilar skull fractures. 8. Hemotympanum (blood behind the ear drum) 9. Periorbital bruising “raccoon eyes”
Fracture of the anterior cranial fossa Periorbital hematoma Subconjunctival hemorrhage CSF or blood running from the nose
Fracture of the middle cranial fossa CSF running from the ear or blood escaping from the ear Bruising behind the ear over the mastoid area Risk of facial paralysis or deafness
Fracture of the posterior cranial fossa Deep coma Bruising on the posterior wall of the pharynx
Raccoon eyes are always bilateral in closed-head trauma and appear in 2 -3 days Black eyes associated with facial trauma can affect one or both eyes and appear within hours from injury
Raccoon: medium-sized mammal native to North America
Battle sign Patients are prone to meningitis due to CSF leakage and meningeal trauma increasing the microbial portal of entry and menigeal integrity.
Basilar skull fractures, breaks in bones at the base of the skull, require more force to cause than cranial vault fractures. Thus they are rare, occurring as the only fracture in only 4% of severe head injury patients.
SKULL VAULT FRACTURES Linear skull fractures, the most common type of skull fracture, occur in 69% of patients with severe head injury. Usually caused by widely distributed forces. In rare cases, a linear fracture can develop and lengthen as the brain swells, in what is called a growing fracture. Diastatic fractures are linear fractures that cause the bones of the skull to separate at the skull sutures in young children whose skull bones have not yet fused. They are usually caused by impact with a wide area such as a wall.
SKULL FRACTURES Comminuted skull fractures, those in which a bone is shattered into many pieces, can result in bits of bone being driven into the brain, lacerating it. Depressed skull fractures, a very serious type of trauma are comminuted fractures in which broken bones are displaced inward. This type of fracture carries a high risk of increasing pressure on the brain, crushing the delicate tissue. Complex depressed fractures are those in which the dura mater is torn. Depressed skull fractures may require surgery to lift the bones off the brain if they are causing pressure on it.
Depressed skull fracture
Liniar skull fractures
Liniar skull fracture
Epidural hematoma
Subdural hematoma
Intracerebral hematoma
TRAUMA 1. Prehospital care 2. Primary survey 3. Resuscitation 4. Secondary survey
PREHOSPITAL CARE Prehospital providers- tasks: Assessment of the injury scene Stabilization of the injured patient Monitoring and transport of critically ill patient
Efficient method for reporting by the prehospital providers to the trauma team on arrival in A&E Unit: M I V T M= mechanism of injury I= injury V= vital signs T= therapy
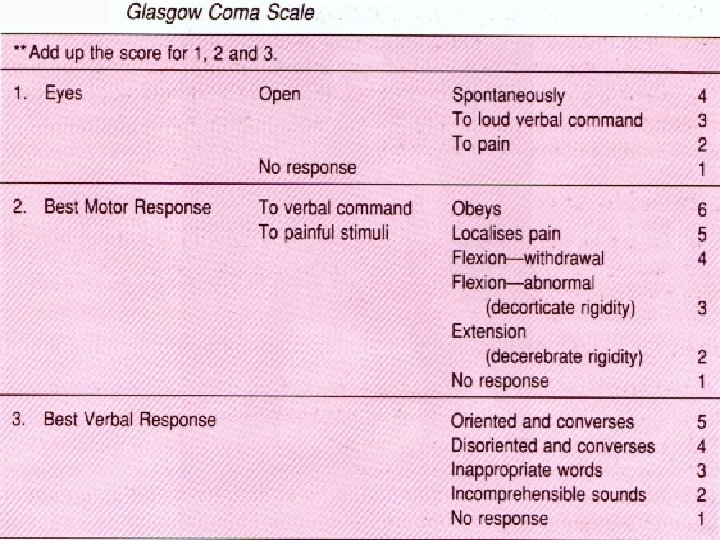
VITAL SIGNS LEVEL OF CONSCIOUSNESS- GLASGOW’S COMA SCORE STABLE / UNSTABLE HEMODINAMICALLY RESPIRATION- spontaneous or ventilated
GCS Less than or equal to 8 at 6 h. - 50% die Severe head injury 3 – 8 Moderate head injury 8 -13 Mild head injury 14 -15 False- hypothermia, intoxication, sedation Impossible to evaluate- dysphasic, intubated pts. and with facial or spinal cord injury
INITIAL EVALUATION AND PRIMARY SURVEY HISTORY: A M P L E PRIMARY SURVEY: A B C D E
HEAD LACERATIONS STEP-OFFS GCS PUPILS CT
NECK HARD NECK COLLAR SPINE X RAY LOCAL TENDERNESS HEMATOMAS SUBCUTANEOUS EMPHYSEMA