SYMPTOMATIC IMPROVEMENT OF CHILDHOOD ASTHMA VERSUS OCCUPATIONAL ASTHMA


 how does removal of asthma exposures (I)")

















- Slides: 21
SYMPTOMATIC IMPROVEMENT OF CHILDHOOD ASTHMA VERSUS OCCUPATIONAL ASTHMA AFTER REMOVAL OF CAUSATIVE AGENTS Capstone Project, MPAS 218 2020 Spring 2020 Brandon Wong April 3, 2020
DISCLOSURES § I have no actual or potential conflict of interest in relation to this presentation § Advising was provided by Dr. Mark Christiansen
PICOT QUESTION In children with asthma (P) how does removal of asthma exposures (I) affect reduction of asthma symptoms (O) compared to adults with occupational asthma (C) after removal from exposure (T)
KEY ISSUES • Understand childhood asthma vs occupational asthma • Identify rates of recovery after removal of exposure • Understand importance of asthma education • Identify possible outcomes of asthma from childhood to adulthood • Prognosis of childhood asthma followed into adulthood
DEFINITIONS • Asthma is a respiratory condition marked by spasms in the bronchi of the lungs, causing difficulty in breathing. It usually results from an allergic reaction or other forms of hypersensitivity. • Occupational asthma (OA) is a form of work-related asthma characterized by variable airflow obstruction, airway hyper-responsiveness, and airway inflammation attributable to a particular exposure in the workplace and not due to stimuli encountered outside the workplace
BACKGROUND INFORMATION • How common is Asthma? • In 2017 it was estimated to affect 25. 1 million Americans • 6. 1 million children • 19 million adults • Most common chronic illness of children < 18 years old • Areas of concern: • Missed school • Missed work • Outcomes of asthma into adulthood
BACKGROUND INFORMATION • From 2008 -2013 the average cost of asthma was $81. 9 billion per year including: • Medical costs • Lost days of work • Lost days of school • Children with asthma average 2. 3 days of school per year • Adults with asthma miss on average 1. 8 days of work per year • Averaging a loss of $1. 9 billion per year from 2008 -2013
COMMON TRIGGERS CHILDHOOD ASTHMA • Ozone • Diesel exhaust • Tobacco • Nitrous oxide • Pollen OCCUPATIONAL ASTHMA • Low molecular weight (LMW) agents • High molecular weight (HMW) agents • Wood dust • Animal and vegetal origin proteins • Drugs • Cockroaches • Metals • Dust mites • Chemicals • Pet dander • Flour • Latex • Grain dust
COMMON TREATMENTS • Short Acting • Short acting beta 2 agonists • Long Acting • Inhaled corticosteroids • Long acting beta 2 agonists • Other agents • Leukotrienes • Oral steroids • Theophylline
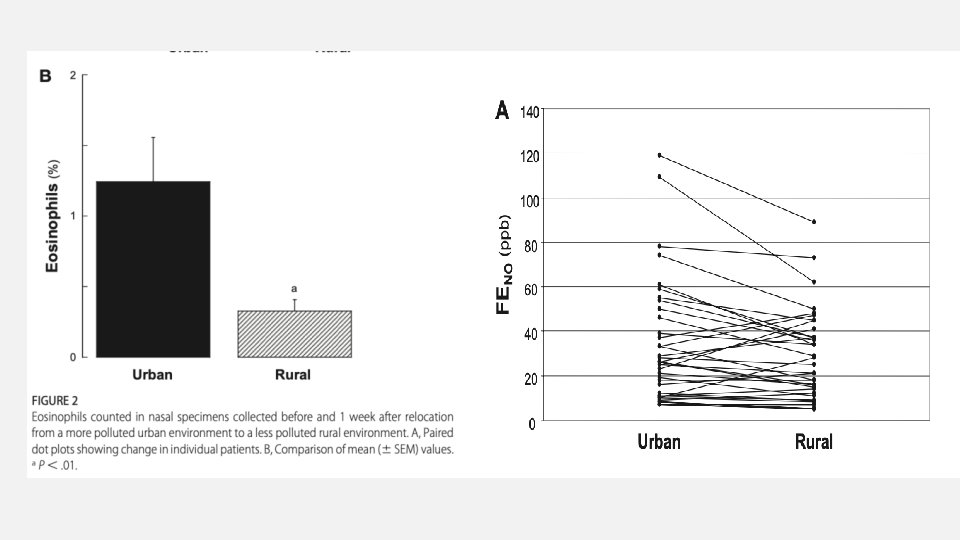
CHILDREN AFTER REMOVAL • Renzetti et al took 37 untreated children with asthma from a highly polluted urban area and relocated to a less polluted rural area for seven days • Clinical parameters measured the day of relocation and seven days after • Results • Fourfold decrease in nasal eosinophils • Significant improvement in Peak Expiratory Flow (PEF) • Increase of approximately 80 L/min (P <. 001)
ADULTS WITH OA AFTER REMOVAL • Systematic review by Rachiotis et al of adults who avoided workplace exposures found: • A pooled estimate of 32% of workers experienced symptomatic recovery • Recovery rates were lower with increasing age • A pooled estimate of 73% had persistent bronchial hyperresponsiveness after exposure removal • Limitations: • Studies analyzed for this systematic review were variable in size and methods
ADULTS WITH OA AFTER REMOVAL • A cross-sectional study conducted by Munoz et al found that: • Avoiding exposure did not significantly improve the prognosis of these patients • 44% of participants who avoided exposure saw improvement compared to 22% who remained exposed • However these findings were not statistically significant • The study did not support the recommendation that patients with OA should change their work place
WHAT ABOUT ADULTS WHO HAD ASTHMA AS A KID? • A longitudinal cohort study performed by Sears et al assessed children with from age 9 to 26 • Findings: • 26. 9% of participants continued to have symptoms by their final evaluation • Only 15% reached and stayed in remission from wheezing • Evidence suggested that outcomes in asthma may be determined in early childhood
WHY IS THIS IMPORTANT? • If outcomes in adult asthma are determined in childhood, management should focus on prevention of exposures more so than treatment of symptoms • The READY* study illustrated that low cost interventions could significantly improve outcomes • Children who received the low cost remediation interventions: • Decreased ED visits per year by 46% • Children who had at least 2 ED events prior experienced a decrease of 63% • Limitations • Study relied on community health worker to make five home visits over a six month span *The Reducing Ethnic/Racial Asthma Disparities in Youth (READY)
LIMITATIONS OF STUDIES • Heterogeneity of studies • No standard in evaluation between studies • Triggers evaluated are different between childhood and occupational asthma
CONCLUSIONS • Children appear to have increased capacity to rapidly improve asthma symptoms compared to adults who experience OA • Outcomes of adult asthma may be determined during childhood • Home remediation can be achieved with low cost solutions • Asthma education is paramount early in childhood
IMPLICATIONS FOR PRACTICE • Education… Education • Home remediation techniques for parents and children • Workplace hazard awareness for those with OA, or simply adult asthma • Pharmacologic treatments are widely utilized but often trigger education is missed due to: • Lack of time • Patient compliance
FURTHER QUESTIONS • A longitudinal study of children who receive home remediation vs. those who did not followed into adulthood. • This would help determine if childhood control could predict disease course in adulthood.
REFERENCES • Renzetti G, Silvestre G, D'Amario C, et al. Less air pollution leads to rapid reduction of airway inflammation and improved airway function in asthmatic children. Pediatrics. 2009; 123(3): 1051 -1058. doi: 10. 1542/peds. 2008 -1153 [doi]. • Nurmagambetov T, Kuwahara R, Garbe P. The economic burden of asthma in the united states, 2008 -2013. Ann Am Thorac Soc. 2018; 15(3): 348 -356. doi: 10. 1513/Annals. ATS. 201703 -259 OC [doi]. • Rachiotis G, Savani R, Brant A, Mac. Neill SJ, Newman Taylor A, Cullinan P. Outcome of occupational asthma after cessation of exposure: A systematic review. Thorax. 2007; 62(2): 147 -152. doi: thx. 2006. 061952 [pii]. • Munoz X, Viladrich M, Manso L, et al. Evolution of occupational asthma: Does cessation of exposure really improve prognosis? Respir Med. 2014; 108(9): 1363 -1370. doi: 10. 1016/j. rmed. 2014. 08. 001 [doi].
REFERENCES • Sears MR, Greene JM, Willan AR, et al. A longitudinal, populationbased, cohort study of childhood asthma followed to adulthood. N Engl J Med. 2003; 349(15): 1414 -1422. doi: 10. 1056/NEJMoa 022363 [doi]. • Centers for disease control and prevention. data, statistics, and surveillance: Asthma surveillance data 2017. https: //www. cdc. gov/asthma/most_recent_national_asthma_data. htm. Accessed 1 December, 2019.