Swelling Itching Brain Management of Cerebral Edema and

Swelling, Itching Brain: Management of Cerebral Edema and Increased Intracranial Pressure Deepak S Nair, MD Stroke Neurology & Neurocritical Care OSF Healthcare – Illinois Neurological Institute
 conflicts of interest to disclose")
Disclosures • No financial (or other) conflicts of interest to disclose

Objectives • Describe the pathologic mechanism of malignant cerebral edema. • Review the current treatment modalities for cerebral edema/intracranial pressure. • Propose an algorithmic approach to ICP crisis in cerebral edema. • NOTE: this discussion is intentionally limited to ischemic stroke

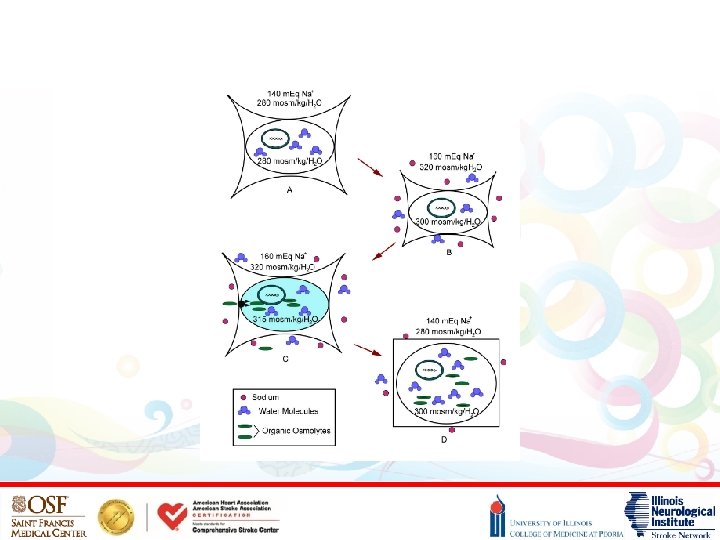
Stages of Cerebra l Edema

Pathophysiology of Cerebral Edema – part 1 • Cytotoxic edema – Occurs within minutes of tissue injury (ischemic cascade) – Water moves from extracellular space to intracellular space – NO increase in total brain volume – no significant “swelling” • Ischemic cascade – – Reduced oxygen & glucose reduced ATP Failure of Na/K pump influx of Na into cell (depolarization) Water follows Na cellular swelling Membrane failure influx of Ca into cell death/rupture

Can we stop this?

Can we stop this? • NOPE

Can we stop this? • Well… • Hyperacute intervention to stop the ischemic cascade – – Ischemic Stroke thrombolysis, endovascular thrombectomy Hemorrhagic Stroke prevent rebleeding, surgical resection? ? Status abort the seizures (benzo’s, AEDs, sedatives) Infection antibiotics, steroids? ? • This is most effective in the setting of ischemic stroke… • But, cytotoxic edema is inevitable, because it happens too fast…

Pathophysiology of Cerebral Edema – part 2 • Vasogenic edema, stage 1 (a. k. a. , Ionic edema) – Cytotoxic edema Na/water gradient across intact BBB – Edema of endothelial cells transcapillary flux of Na – Water follows Na increased extracellular water content • Vasogenic edema, stage 2 – Endothelial damage breakdown of BBB – Leakage of plasma & proteins/ions into extracellular space – Water follows proteins/ions increased water content of brain

Can we stop this? ?

Can we stop this? ? • NOPE

Can we stop this? ? • Well… • BBB disruption – Osmotic agents only effective if they are blocked by an intact BBB – Leakage of osmotic agents into tissue can worsen edema • Occluded capillary flow – Arterial flow may be already blocked by thrombus (ischemic stroke) – Tissue edema eventually compresses the capillaries – Limited movement of water from edematous tissue • In ischemic stroke, this tends to be ineffective, because of all the above

What the heck? ? • Is this the end of the talk? ?

What the heck? ? • Edema sucks, and we can’t do anything about it? ?

What the heck? ? • Maybe we should start over…

Swelling, Itching Brain: Management of Increased Intracranial Pressure Deepak S Nair, MD Stroke Neurology & Neurocritical Care OSF Healthcare – Illinois Neurological Institute
 conflicts of interest to disclose")
Disclosures • No financial (or other) conflicts of interest to disclose

Objectives • Describe the pathologic mechanism of ICP crisis. • Review the current treatment modalities for ICP crisis. • Propose an algorithmic approach to managing ICP crisis.

Increased Intracranial Pressure

Treatment Options for ICP Crisis • Standard measures • Surgery if/when indicated • Medical management – ICP monitoring – Ventilator optimization – Osmotherapy – Barbiturate coma – Therapeutic hypothermia • Investigational

Standard Measures • • ABC’s Head/neck position Mild sedation Avoid hyponatremia Avoid hypotonic fluids Avoid hyperglycemic fluids Avoid/prevent fever Avoid/prevent seizures

Decompressive Hemicraniectomy

Hyper-osmolar Therapy • Mannitol – Non-metabolized sugar alcohol, used for diuresis – Creates an osmotic gradient across an intact BBB – Diffusion of water into intravascular space, decreases brain water content – Lowers ICP, typically when s. Osm is ~320 m. Osm – Can induce renal failure, so must monitor osmolar gap • Hypertonic saline Multiple formulations (3% 23. 4%) Creates osmotic gradient, decreases brain water content Lowers ICP, when serum Na is 145 – 155, or higher in selected patients Increases intravascular volume beneficial effects on CPP/CBF/oxygenation – Rapid reversal can lead to rebound edema, so titrate off slowly – –

Putting it all together • Anticipate cerebral edema, based on stroke severity • Initiate “Standard Measures” for all severe strokes • Monitor for edema/ICP crisis – Serial neuro exams – Serial imaging – ICP monitoring, if/when appropriate • Team-based approach – Stroke/Neurology – Neurosurgery – Critical Care • Do not delay treatment

Goals of Care • ICP < 20 • CPP 60 -70 Signs/symptoms of increased ICP • Consider possible causes • Appropriate imaging Standard • Ongoing, unless superseded by other Measures measures Recognized • Emergent NSGY Consult Surgical • Consider EVD placement (see “ICP Monitoring”) Indications ICP Monitoring • Consider EVD placement • Coma with high ICP • TBI • Hydrocephalus • SAH • Many others • Verify ICP accuracy • Review waveform • Check tubing for air/blockage • EVD level • EVD accuracy drifts over time Standard Measures • ABC's • Head/Neck position • Mild sedation as necessary • Avoid hyponatremia (Na <140 mmol/L) • Avoid hypotonic fluids • Avoid hyperglycemia • Avoid fever • Avoid seizures • When pulmonary status allows – minimize PEEP & PIP & TV Ventilator • Maintain minute ventilation Management • Watch for pulmonary edema, ARDS, hemo/pneumo-thorax • HTS or Mannitol Osmotherapy • Consider urgent bolus of both followed by maintenance dosing of either or both Barbiturate Infusion Therapeutic Hypothermia

Questions…
")
References • Treadwell, S. D. , and B. Thanvi. "Malignant Middle Cerebral Artery (MCA) Infarction: Pathophysiology, Diagnosis and Management. " Postgraduate Medical Journal (2010): n. pag. Print. • Ryu, Justine H. , Brian P. Walcott, Kristopher T. Kahle, Sameer A. Sheth, Randall T. Peterson, Brian V. Nahed, Jean-Valery C. E. Coumans, and J. Marc Simard. "Induced and Sustained Hypernatremia for the Prevention and Treatment of Cerebral Edema Following Brain Injury. " Neurocritical Care 19. 2 (2013): 222 -31. Print. • Kahle, K. T. , J. M. Simard, K. J. Staley, B. V. Nahed, P. S. Jones, and D. Sun. "Molecular Mechanisms of Ischemic Cerebral Edema: Role of Electroneutral Ion Transport. " Physiology 24. 4 (2009): 257 -65. Web. • Torre-Healy, Andrew, Nicholas F. Marko, and Robert J. Weil. "Hyperosmolar Therapy for Intracranial Hypertension. " Neurocritical Care 17. 1 (2011): 117 -30. Print. • Lukitsch, Ivo. "Hypernatremia. " Background, Pathophysiology, Epidemiology. EMedicine/Medscape, 08 Sept. 2016. Web. 05 Apr. 2017.
- Slides: 28