Surveillance of Abdominal Hysterectomy Surgical Procedures Presented by

Surveillance of Abdominal Hysterectomy Surgical Procedures Presented by: Audrey Adams, RN, MPH, CIC Director of Infection Prevention & Control
 • Significant economic consequences: Ø Estimated cost of")
Background of Hospital Acquired Infections (HAI) • Significant economic consequences: Ø Estimated cost of $4. 5 billion. • Fifth leading cause of death in hospitals.
 2. Surgical site")
Four leading categories of infection: 1. Catheter-associated urinary tract infections (CAUTIs) 2. Surgical site infections (SSIs) 3. Central line associated bloodstream infections (CLABSIs) 4. And ventilator-associated pneumonia (VAP).
 • Incidence of HAIs has increased by 36%")
Background of Hospital Acquired Infections (HAI) • Incidence of HAIs has increased by 36% in the last 20 years • A major public health problem worldwide • Affect >10% of hospitalized patients annually with over 2 million infections and >90, 000 deaths.

Burden of HAI Major Site of Infection Total Infections Hospital Cost Per Infection Total Annual Hospital Cost (in millions) Deaths Per Year Surgical Site Infections 290, 485 $25, 546 $7, 421 13, 088 Central Line-Associated Bloodstream Infections 248, 678 $36, 441 $9, 062 30, 665 Ventilator-Associated Pneumonia (lung infection) 250, 205 $9, 969 $2, 494 35, 967 Catheter-Associated Urinary Tract Infection 561, 667 $1, 006 $565 8, 205 Source: U. S. Department of Health & Human Services 2009
 • It has been demonstrated that many HAIs")
Background of Hospital Acquired Infections (HAI) • It has been demonstrated that many HAIs are preventable by implementing evidence base prevention strategies. • To ensure that hospitals recognize their role in preventing HAIs, State and national regulatory agencies have required reporting of specific HAIs.

Affordable Care Act Hospital Acquired Conditions Sec. 3008. PAYMENT ADJUSTMENT FOR CONDITIONS ACQUIRED IN HOSPITALS • Penalizes hospitals for hospital-acquired conditions (HACs) Ø Beginning in 2015 CMS subtracts 1% of payments from hospitals with the highest rates of HACs (bottom quartile performers when compared to the national average). Ø Results in system-wide reduction of $1. 5 billion over 10 years.

CMS Mandated HAI Reporting to NHSN YEAR HAI REPORTING 2011 • CLABSI – Acute Care ICUs (Jan) 2012 • • • CAUTI – Acute Care ICUs (except NICUs) (Jan) CAUTI – LTCH, IRF, Cancer Hospitals (Oct) SSI – Colon and Abdominal Hysterectomy Surgeries – Acute Care (Jan) Dialysis Events – ESRD (Jan) CLABSIs – LTCH, Cancer Hospitals (Oct) • • C. Difficile Lab. ID Events – Acute Care (Jan) MRSA Bacteremia Lab. ID Events – Acute Care (Jan) HCP Influenza Vaccination – LTCH (Jan) 2013 2014 2015 • HCP Influenza Vaccination – ASCs (Oct) • SSI – Cancer Hospitals (Jan) • HCP Influenza Vaccination – IRF (Oct) • • CLABSI – Acute Care Med, Surg, Med/Surg Units (Jan) CAUTI – Acute Care Med, Surg, Med/Surg Units (Jan) MRSA Bacteremia Lab. ID Events – LTCH (Jan) C. Difficile Lab. ID Events – LTCH (Jan)

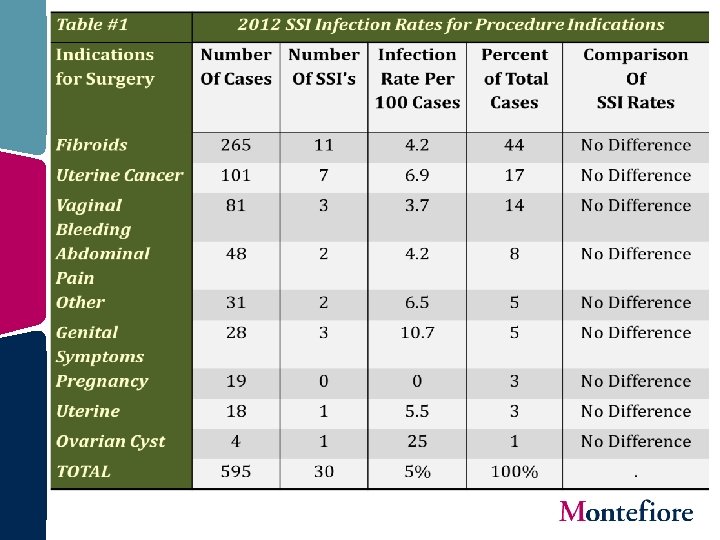
Objectives • To perform an overall analysis of SSIs related to total abdominal hysterectomies (TAH) in 2012. • Investigation of indicators for TAH and associated infection risk.

Methods • The NHSN Patient Safety Component was used to perform surveillance of TAH. • Using inpatient procedure codes, each procedure was classified into 1 of 9 procedure codes. • The NHSN data base was used to identify specific SSI events, along with the mode of detection and organisms associated with the SSIs. • The use of prophylactic antibiotics for SSIs was determined by chart review.
 Defined SIP - Super incisional primary surgical site")
NHSN - Surgical Site Infections (SSIs) Defined SIP - Super incisional primary surgical site infection SIS - Superficial incisional secondary surgical site infection DIP - Deep incisional primary surgical site infection DIS - Deep incisional secondary surgical site infection IAB - Intraabdominal surgical site infection

SSI Detection Table 3 Detection of SSIs Number of SSIs Total SSIs Percent Of Total During Admission 2 30 7 Post Discharge Surveillance 10 30 20 Readmission 16 30 53 Readmission to Another Facility 2 30 7
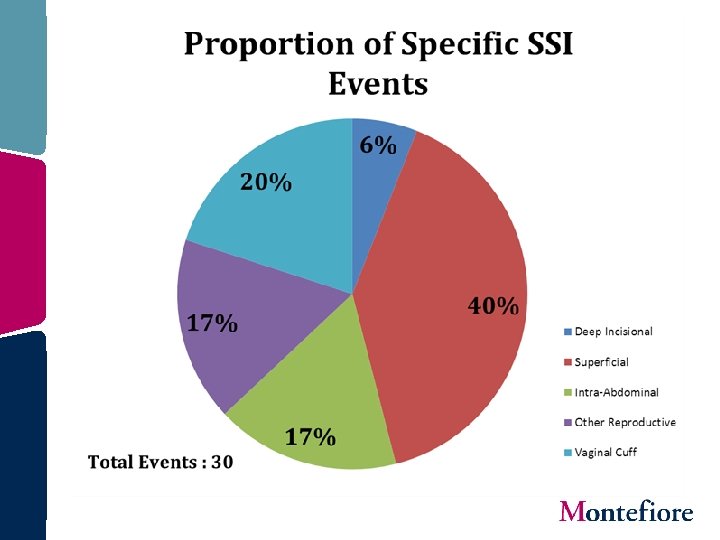
 of the SSIs were superficial. • Electronic medical records,")
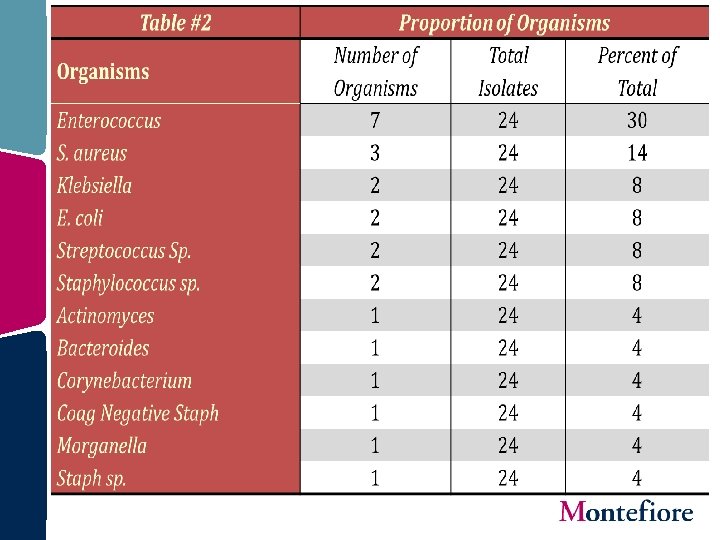
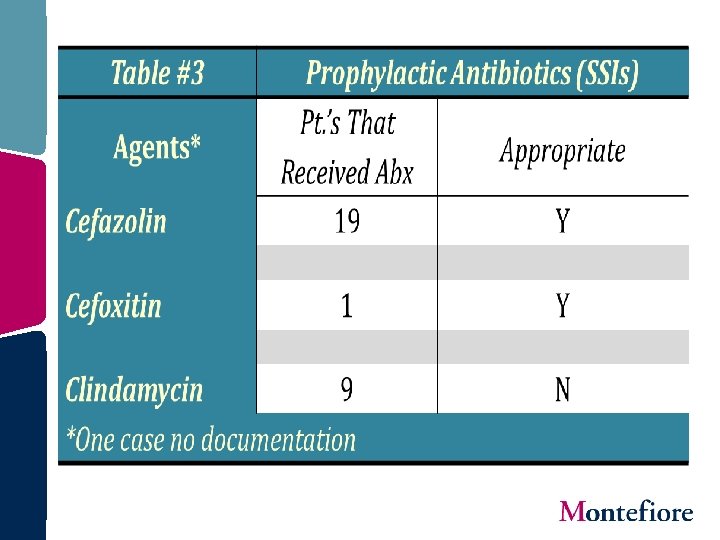
Conclusions • Forty percent (40%) of the SSIs were superficial. • Electronic medical records, which extend to ambulatory sites, facilitated the identification of 10 (33%) SSIs via post discharge surveillance. • Enterococcus (30%) and S. aureus (14%) were the highest proportion of organisms identified. • Of the 29 prophylactic antibiotic agents given for those with SSIs, 69% were appropriate.
 • Of the 30 SSIs identified, 29 received prophylactic antibiotics. Thirty-one")
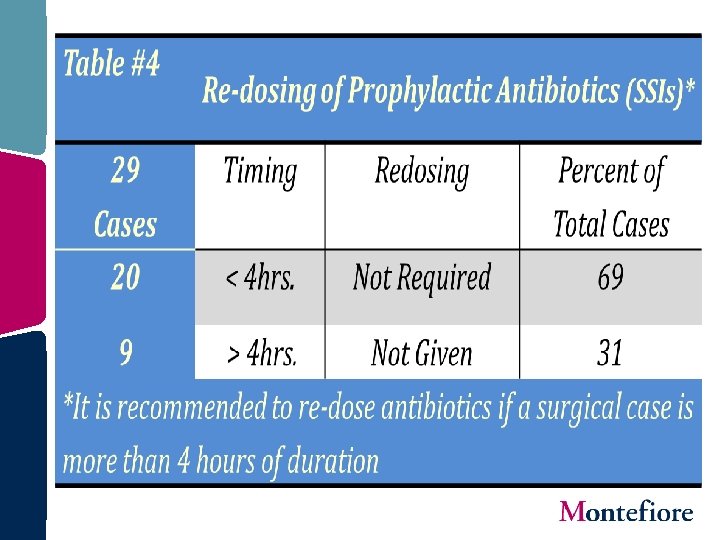
Conclusions (cont. ) • Of the 30 SSIs identified, 29 received prophylactic antibiotics. Thirty-one percent (31%) of these did not receive required re-dosing after 4 hours of surgery. • Although TAH are performed for a variety of indications, it appears that no one indication carries a higher infection risk than others. However, this conclusion should be tempered by the small sample sizes. • There may be risk factors for TAH SSIs as yet to be determined. Further investigation is required for risk stratification of TAH with larger sample size.

Hysterectomy Surgical Site Infection Rates 3. 3 2. 6 2. 1 1. 4 Einstein Campus Moses Campus MMC - Hysterectomy Total SSI Rates 0. 5 6 1. 8 5. 8 Percent 5. 6 5. 4 5. 2 5. 1 5 Rates 4. 8 4. 4 4. 6 Wakefield Campus 4. 4 4. 2 2013

Infection Prevention & Control is in YOUR hands!
- Slides: 21