Surgical Treatment of Stress Urinary Incontinence Dr Cecilia


 - Involuntary leakage on effort or")
 - Involuntary leakage of urine during increased")

 •")







 Abdominal Laparoscopic")







")


 • Ulmsten et al in 1996 • Treats stress incontinence")

 • Delorme 1 in transobturator procedure 2001 described the (outside-in :")
")



 • A variation of the technique has been described in 2003")
")


 to various procedure Tension-Free Midurethral Slings in the Treatment")
 Colposuspension Mid-urethral Sling 222 402 50. 74")










- Slides: 68
Surgical Treatment of Stress Urinary Incontinence Dr Cecilia Cheon Consultant, Department of Obs. & Gyn. Queen Elizabeth Hospital, Hong Kong, China President, HK Urgynaecology Association
Definition of Urinary Incontinence Urinary incontinence is the complaint of any involuntary leakage of urine. Abram P et al. Neuro Urodyn 02
Terminology - Symptoms • Stress urinary incontinence (SUI) - Involuntary leakage on effort or exertion, or on sneezing or coughing
Urodynamic Terminology • Urodynamic stress incontinence (USI) - Involuntary leakage of urine during increased abdominal pressure, in the absence of a detrusor contraction - Old term: Genuine stress incontinence (GSI)
Impact on Quality of Life • Embarrassment • Reduced Self esteem • Impaired emotional & psychological wellbeing • Poorer sexual relationships • Impaired social activities and relationships
Economic Issues • USA – estimated to be $8. 1 billion (Hu, 1984) • Active evaluation and treatment of nursing home residents resulted in considerable cost savings • Indirect benefit : improve QOL of sufferers, difficult to quantify
Stress incontinence : Weakness of the pelvic floor muscles
Treatment Strategy in women with USI / SUI Conservative treatment is the first line of treatment for women with SI International Consultation on Incontinence 01, Paris
Treatment for SUI 1. General measures 2. Pelvic floor exercises, PFEs 3. Biofeedback - perineometer, vaginal cones 4. Electrical stimulation treatment 5. Mechanical devices 6. Pharmacological treatment 7. Surgery
Surgical Treatment • Paravaginal repair • Bladder neck suspensions • Bladder Neck Slings / Midurethral slings • Periurethral injections • Artificial sphincter
Surgical Treatment benefit Best long term result risk minimal complication
Bladder Neck Suspensions To use the anterior vagina as a hammock to elevate the bladder neck • Needle suspensions • Retropubic suspensions - abdominal - laparoscopic
Retropubic Suspensions • Burch’s • MMK
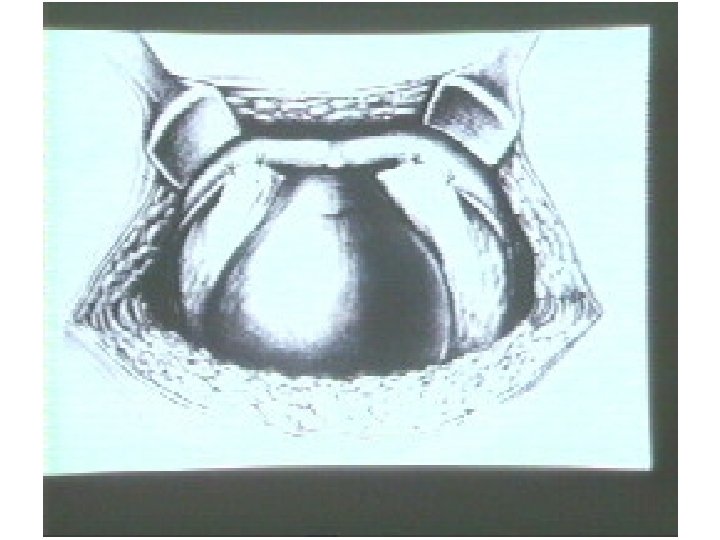
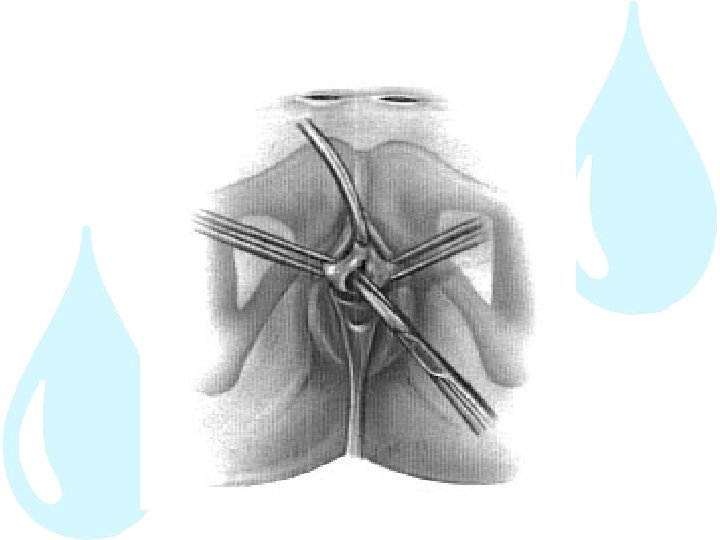
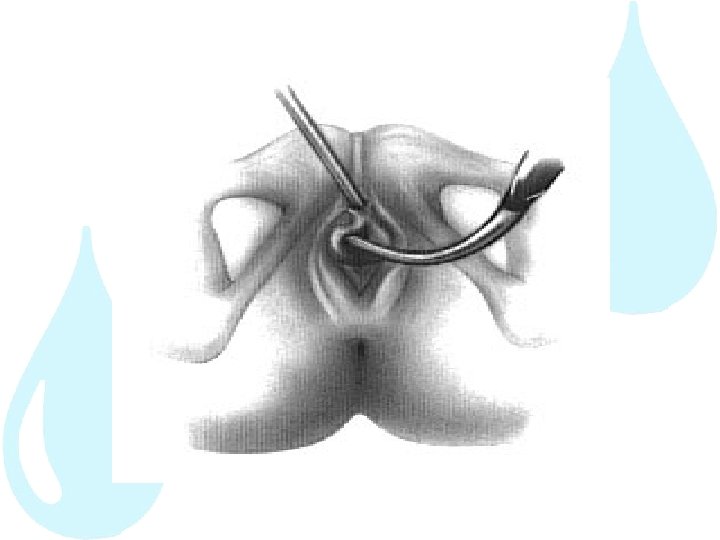
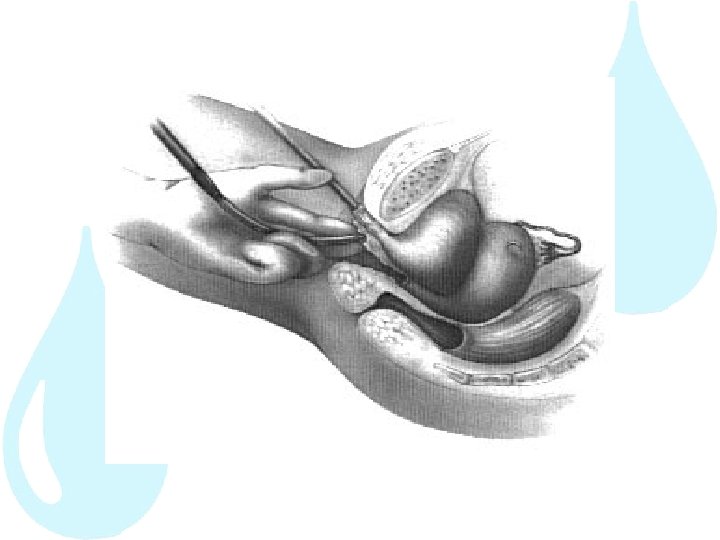
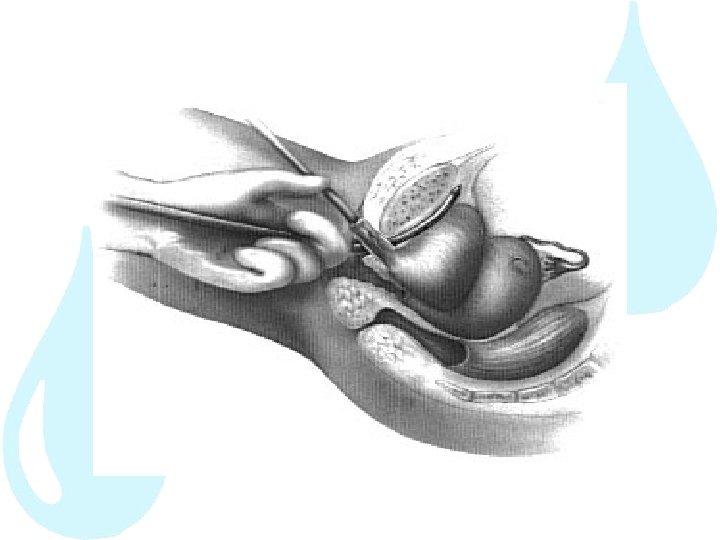
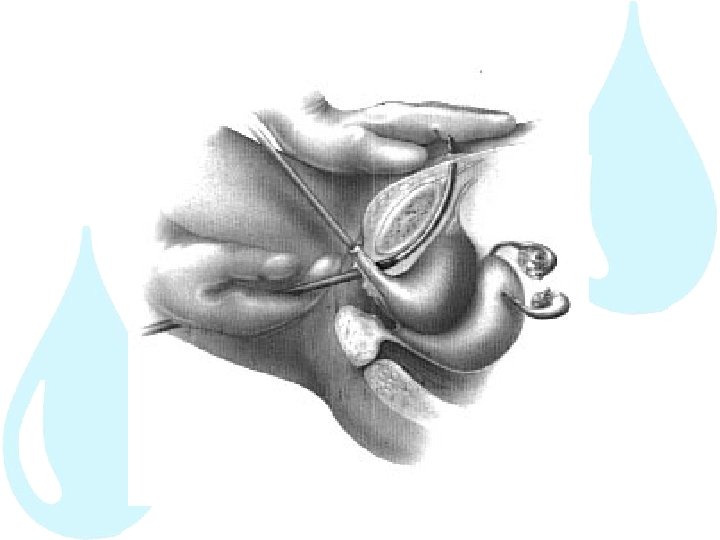
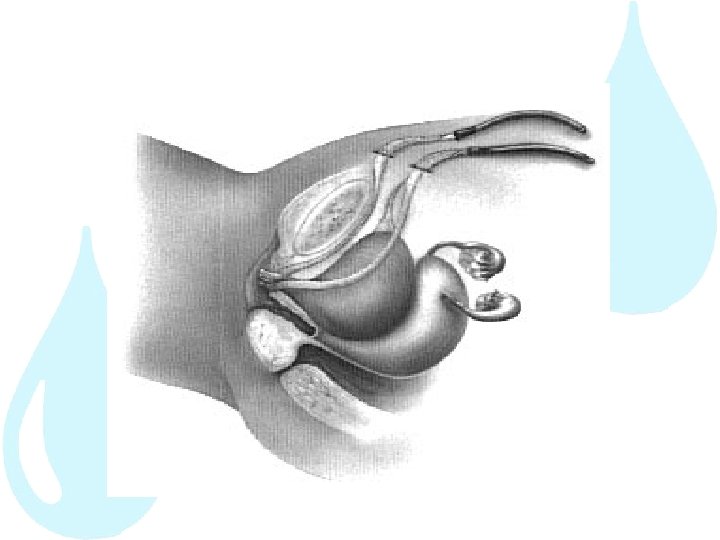
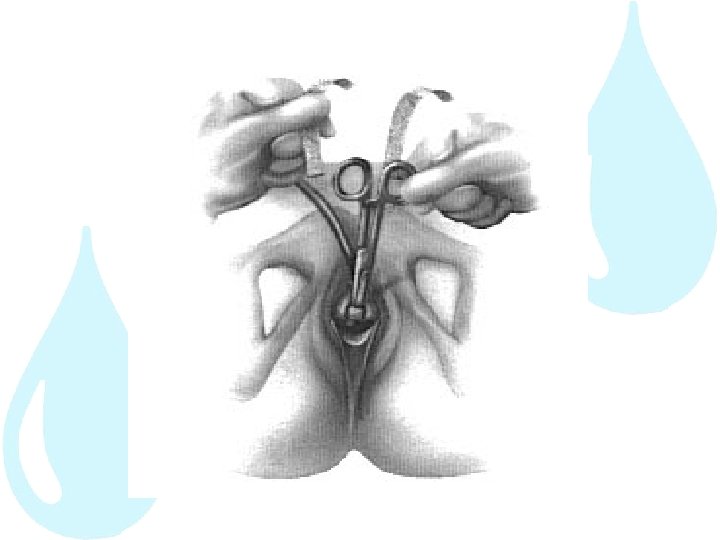
Burch’s Colposuspension Suspension of anterior vagina to the iliopectineal ligament(Cooper’s ligament) Abdominal Laparoscopic
Burch Colposuspension
Burch Colposuspension
Subjective Cure Rate for Burch’s Operation
Objective Cure Rate for Burch’s Operation
Burch’s Success rate • 39 trials, 3, 301 women • 1 st year 85 – 90% • 5 year 70% • No significant difference between open and laparoscopic approach Lapitan et al, Cochrane Database Systematic Reviews 2008
Burch’s Colposuspension Complications • Detrusor overactivity 5 – 10% • Voiding difficulty 10 – 15% • Apical / posterior 5 – 17% compartment prolapse
Slings Sling under the bladder neck or mid-urethra • Correct hypermobility • Increase sphincter closure pressure
Midurethral-slings • To date, three major slings available - Tension-free vaginal tape (retropubic approach) – TVT - Tension-free vaginal tape (transobturator approach) – TOT / TVT-O - Minisling
The Integral Theory of Continence • Pelvic organ prolapse mainly caused by connective tissue laxity in the vagina or its supporting ligaments • Stress urinary incontinence is essentially due to pelvic floor muscle weakness
The pictorial diagnostic algorithm summarizes the relationships between structural damage in the three zones and urinary and fecal symptoms. Arrows represent directional muscle forces. Anterior zone: external urethral meatus to bladder neck; middle zone: bladder neck to cervix; posterior zone: vaginal apex, posterior vaginal wall, and perineal body. PRM = m. puborectalis; PCM = pubococcygeus; PUL = pubourethral ligament; ATFP = arcus tendineus fascia pelvis; N = bladder base stretch receptors
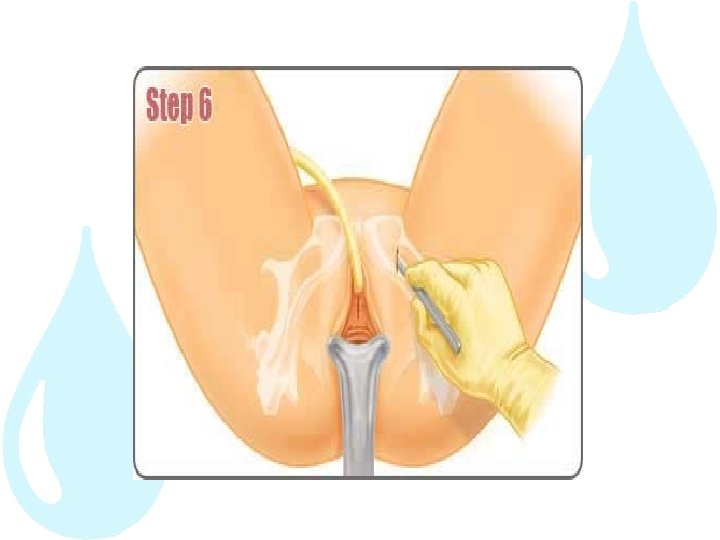
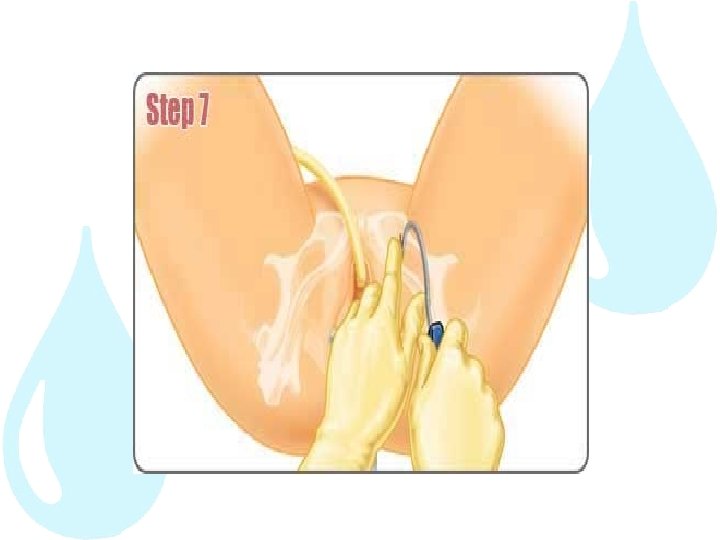
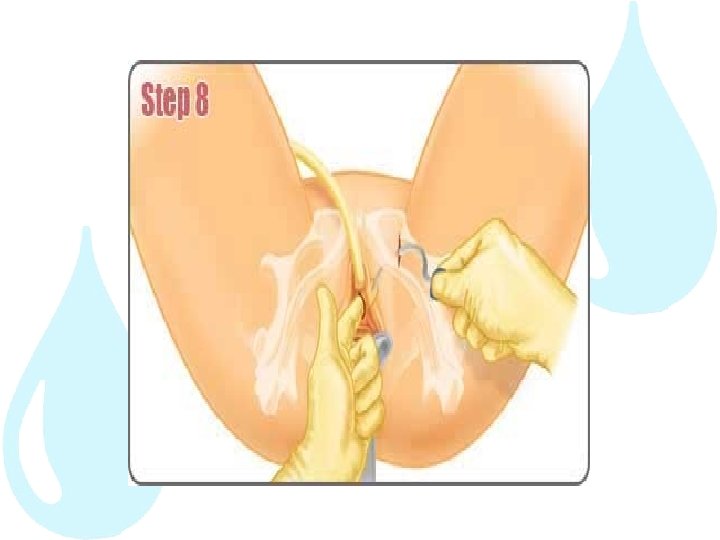
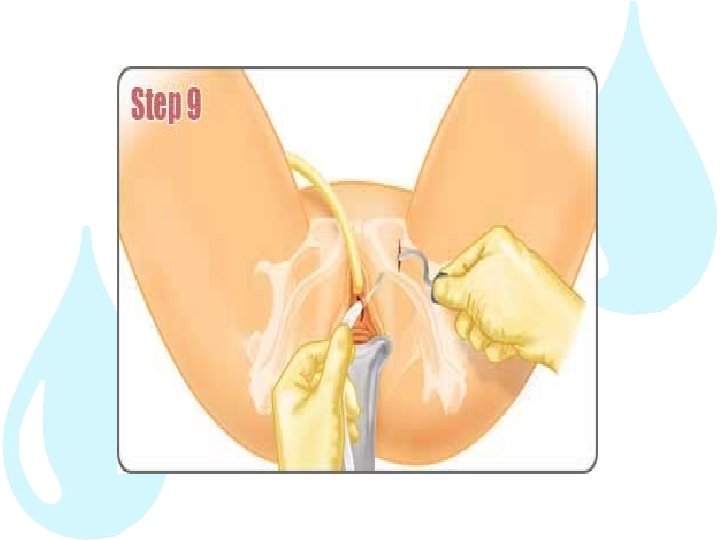
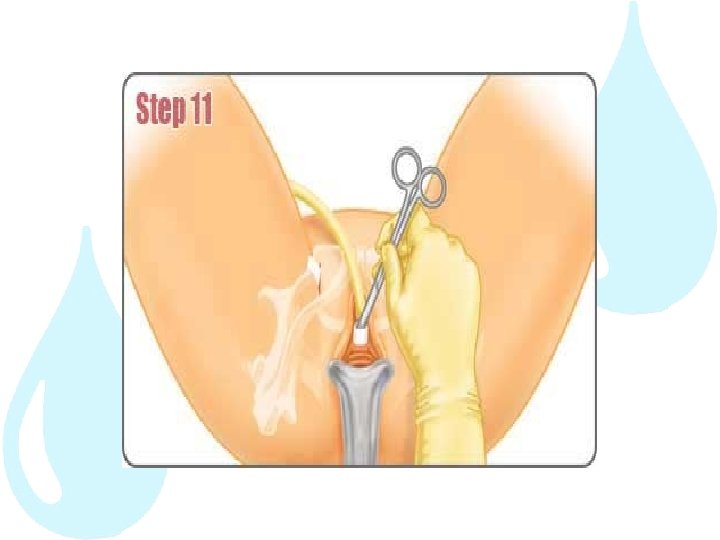
Tension-free Vaginal Tape (TVT) • Ulmsten et al in 1996 • Treats stress incontinence by positioning a polypropylene mesh tape underneath the urethra • Monofilament, macroporous, >75 microns • Free passage of marophages • In growth of fibroblast • Minimize erosion / infection
Tension-free vaginal Tape
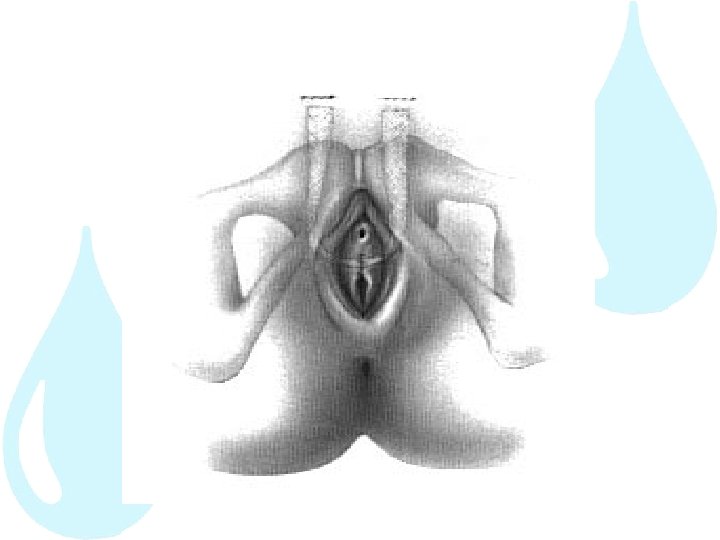
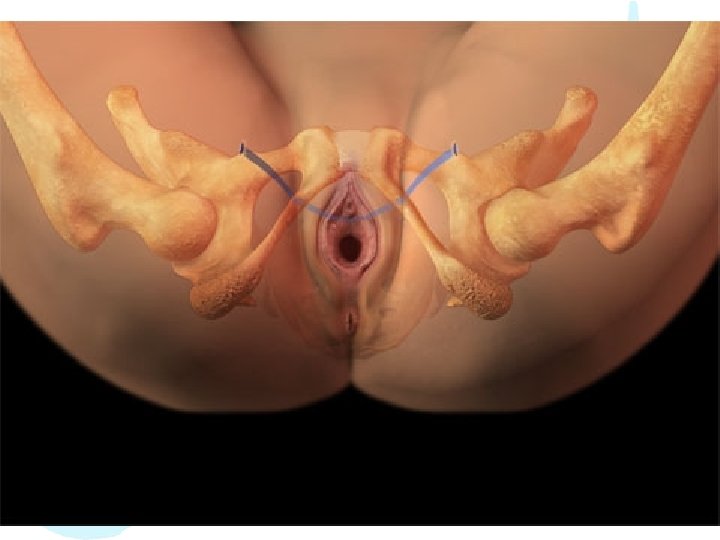
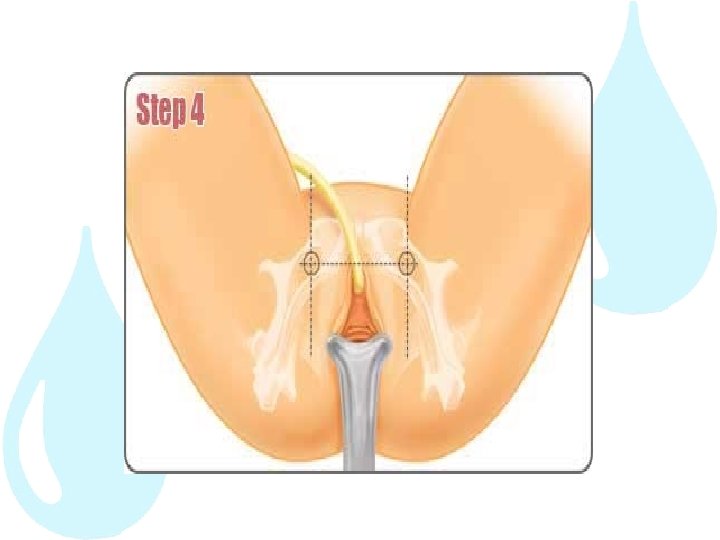
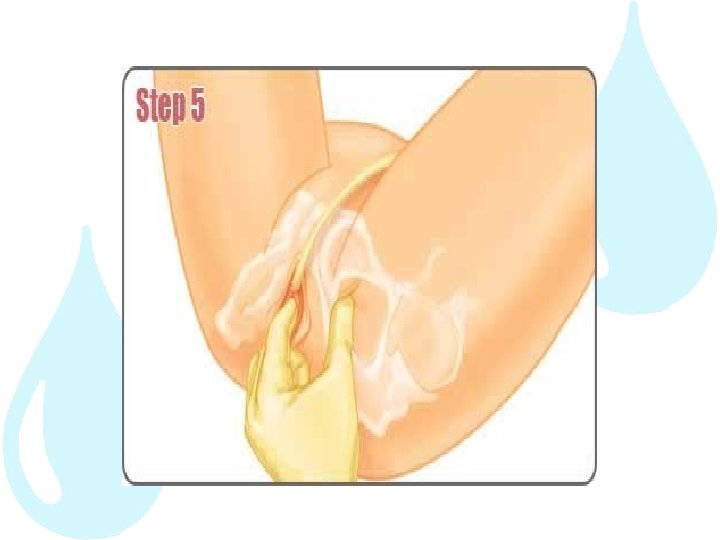
Transobturator Tape (TOT) • Delorme 1 in transobturator procedure 2001 described the (outside-in : TOT) • Insert mesh tape under the urethra through small incisions in the groin area • eliminates retropubic needle passage
Transobturator Tape (outside in)
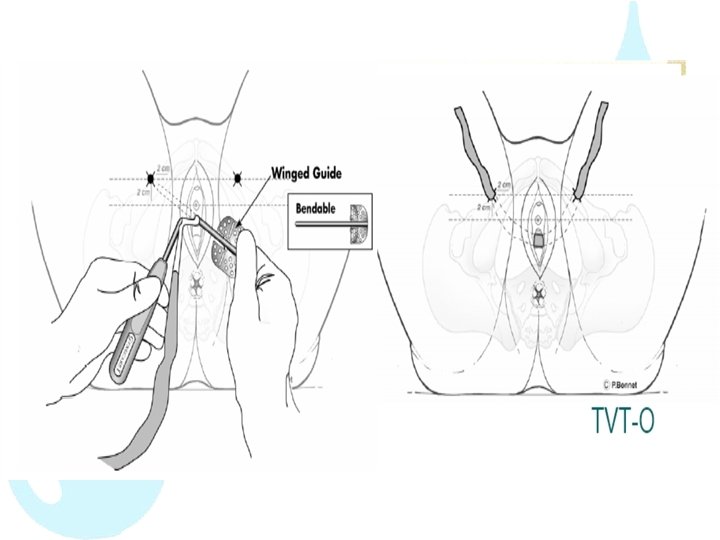
Transobturator Tape (TOT-O) • A variation of the technique has been described in 2003 by de Leval termed the TOT vaginal tape ‘‘inside-out’’ technique (TVT-O)
Transobturator Tape (inside out)
Imaging
TVT / TOT / TVT-O Complications • 3% • Voiding hematoma, difficulty, bladder hemorrhage, perforation, infection • No report of rejection, erosion or fistula
Comparison of Mid-urethral sling (TVT) to various procedure Tension-Free Midurethral Slings in the Treatment of Female Stress Urinary Incontinence: A Systematic Review and Metaanalysis of Randomized Controlled Trials of Effectiveness Giacomo Novara et al. (Italy) 2007
Comparison of Mid-urethral Sling vs Colposuspension (QEH) Colposuspension Mid-urethral Sling 222 402 50. 74 60. 36* (p<0. 001 ) Bladder injury (%) 0. 9 4* (p=0. 03) Days of bladder training (mean) 3. 96 3. 41 1 year subjective success (%) 82. 7 89* 1 year objective success (%) 89. 1 83. 4 1 year DO (%) 27. 7 30. 2 3 years subjective success (%) 76. 3 (169) 87. 7 (173)* (p=0. 007 ) 3 years objective success (%) 77. 1 85. 6* (p=0. 04) 5 years subjective success (%) 75. 8 (95) 89. 2 (74)* (p=0. 03) No. of patients Age (p=0. 03)
• Today, mid-urethral slings not only have replaced the Burch colposuspension as the gold standard in the treatment of SUI but also are even more often performed than colposuspension • Easy to perform, superior in terms of operation time, postoperative pain, and hospital stays • but similar cure rates
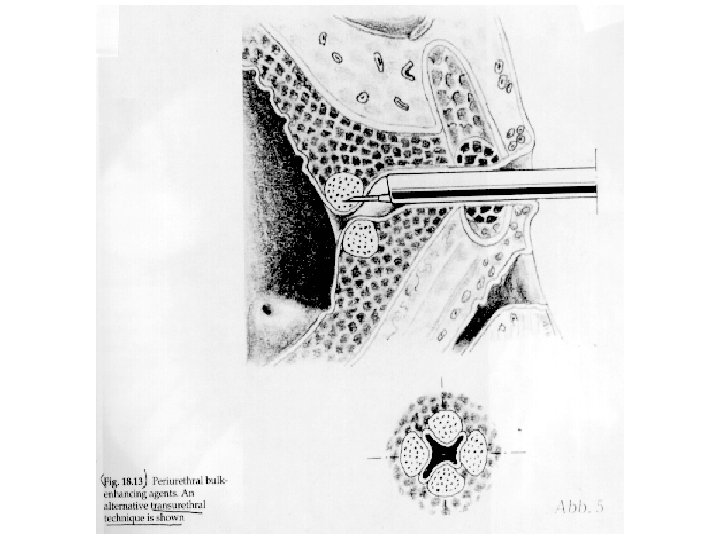
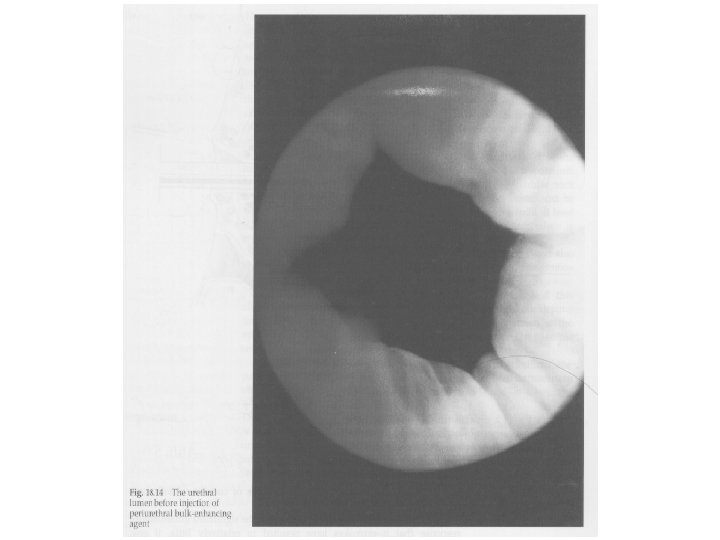
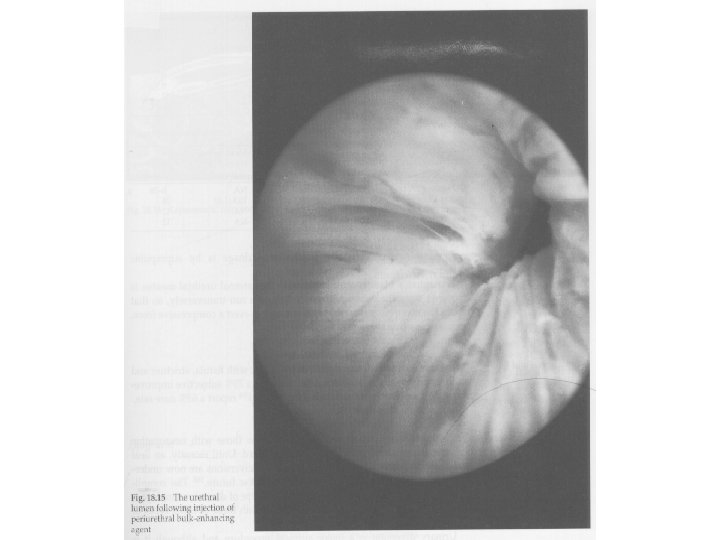
Peri-urethral Injection Use of injectable bulk forming agents to increase the urethral closure pressure
Peri-urethral Injection Material • Fat • Collagen • Silicone
Peri-urethral Injection Advantages • Safe Disadvantages • Low success rate 25 – 60% • Expensive • Need to be repeated every 1 -2 year
Artificial Sphincter • Last resort • Use when all the other operation have failed
Artificial Sphincter
Conclusions • 1 in 2 women in HK has urinary symptoms 1 in 3 women has SUI • Much advances made in the care of female urinary incontinence • Effective treatment available which can significantly improve women’s Qo. L
Conclusion • The concept of the midurethral sling has revolutionized surgical treatment of SUI. Its minimally invasive approach and success rates have led to an increasing acceptance of the technique • TVT and TOT are both comparable in cure rate • The TOT approach is a potentially safer method owing to the avoidance of the retropubic space: bladder, vessels, bowel injury • Pregnancy is not contraindicated and cesarean is not abolute
• Long-term studies and RCTs are needed to identify the proper indications for the various types of slings and to assess efficacy and complication rates over time.