Surgical issues of the Oesophagus Dr S Nishan
")
 to Gastro oesophageal junction")
 Esophageal Body (cervical & thoracic) Lower Esophageal Sphincter")













 to open when the peristaltic wave")




")


 • Reflux of gastric contents • Inflammatory changes are due to")
 • Metaplasia of the oesophageal mucosa.")



































*")

")

- Slides: 71
Surgical issues of the Oesophagus Dr. S. Nishan Silva ( MBBS )
Oesophagus – Normal Anatomy • Extends from Pharynx (C 6) to Gastro oesophageal junction (T 11/T 12) • 25. 0 cm in length. • 3 points of narrowing Cricoid cartilage L/S Bronchus Diaphragm. • UES – 3 cm segment at the cricopharyngeal muscle. • LES – 2 – 4 cm segment in the abdomen proximal to the anatomical GE sphincter.
Esophageal Anatomy Upper Esophageal Sphincter (UES) Esophageal Body (cervical & thoracic) Lower Esophageal Sphincter (LES) 18 to 24 cm
Oesophagus - Histology • Mucosa – non keratinizing squamous epithelium. • Submucosa – loose Connective tissue. • Muscularis propria – Inner – circular – Outer – Longitudinal Skeletal mm fibres in the initial 10 – 12 cms. (Cricopharngeus) • Serosal Coat - ABSENT
Normal Swallowing Frontal cortex Cortical Swallowing Areas Swallowing Center Brainstem Motor Nuclei Oropharynx & Esophagus
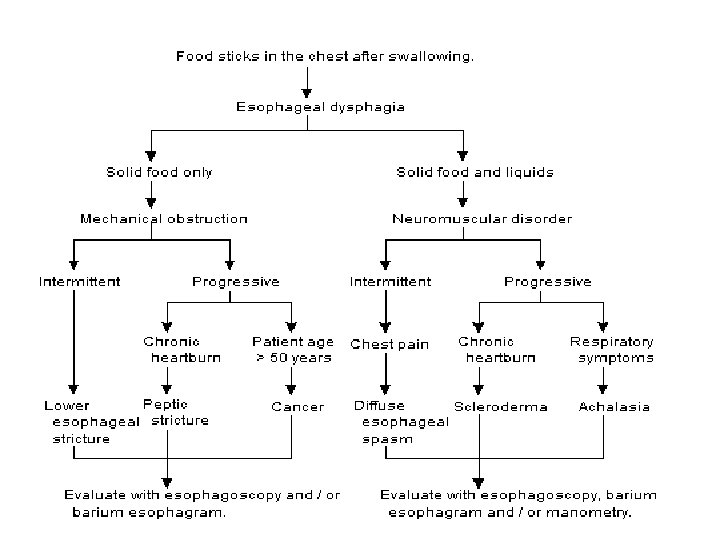
Symptoms of dysphagia Esophageal dysphagia Sensation of food sticking in the chest Oral or pharyngeal regurgitation Food sticking in the throat Drooling Unexplained weight loss Change in dietary habits Recurrent pneumonia
Causes of dysphagia • Neurologic disorders and stroke Cerebral infarction Brain-stem infarction Intracranial hemorrhage Parkinson's disease Multiple sclerosis Amyotrophic lateral sclerosis Poliomyelitis Myasthenia gravis Dementias. Psychiatric disorder Psychogenic dysphagia
Causes of dysphagia • Structural lesions Thyromegaly Cervical hyperostosis Congenital web Zenker's diverticulum Ingestion of caustic material Neoplasm
Causes of dysphagia • Connective tissue diseases Polymyositis Muscular dystrophy • Iatrogenic causes Surgical resection Radiation fibrosis Medications
Oesophageal disorders • Congenital abnormalities • Motility disorders – Achalasia cardia – Oesophageal diverticula – Rings and webs • Ulcerations and lacerations • Vascular lesions • Organic lesions – Strictures and tumours
Congenital abnormalities – Tracheo oesophageal fistula Commonest is Type C
Congenital abnormalities • Stenosis • Atresia • Heterotopia – Gastric mucosa Sebaceous glands. • Cysts – Inclusion cyst – Columnnar and squamous epithelial lined cysts Retention cysts.
Motility disorders • • • Achalasia cardia Diverticula Rings and webs Hiatus hernia * Gastro oesophageal reflux disease *
Diverticula Outpouchings of the mucosa at points of weakness PULSION DIVERTICULUM Epiphrenic – above the diagphragm Zenkers – Pharyngo oesophageal TRACTION DIVERTICULUM Pull due to attachement to extrinsic structures Eg: TB Lymph nodes
Diverticula • MULTIPLE – Diffuse intramural oesophageal diverticulosis. • COMPLICATIONS – Obstruction, infection, haemorrhage, perforation, increased incidence of malignancy.
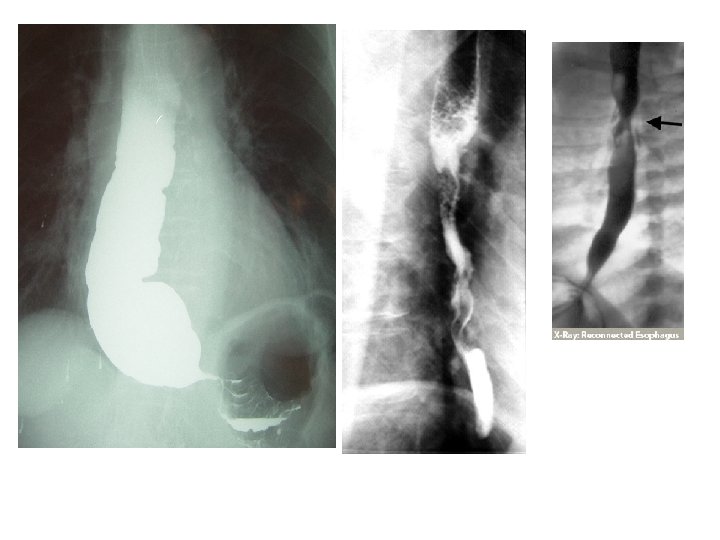
Achalasia Cardia
Achalasia cardia • Failure of the cardia (LES) to open when the peristaltic wave reaches it. • Major abnormalities in the Achalasia cardia Aperistalsis Partial / complete relaxation of LES Increased basal tone of LES
Achalasia cardia • Symptoms – Progressive dysphagia. Regurgitation of undigested food. Aspiration pneumonia. Retrosternal discomfort. Foetid flatulence.
Achalasia cardia - Pathology • Progressive dilatation of the upper segment • Wall – thickened proximally due to muscular hypertrophy. – Wall thinned out due to dilatation. – Normal in thickness • Ganglia – absent in upper segment. • Ulceration and inflammation of the oesophageal lining.
Hiatus Hernia
Hiatus Hernia • Sliding type – Disturbance of the normal relationship of the gastro oesophageal junction. Reflux. • Paraoesophageal / rolling type – Strangulation & Obstruction.
Ulceration of the Oesophagus • Mallory – Weiss Syndrome – ( laceration / tear) • Oesophagitis.
Mallory – Weiss Syndrome • Tear in the oesophageal mucosa which is oriented longitudinally astride the oesophagogastric junction: Common in alcoholics.
Inflammations – Oesophagitis. • • • Reflux oesophagitis. Prolonged gastric intubation. Ingestion of corrosive alkali, smoking. Uraemia. Bacteraemia / Viraemia. – HSV CMV, Fungal infection – Candida, Mucor, Aspergillus. Cytotoxic treatment. Pemphigoid and Epidermolysis Bullosa. Graft vs Host disease.
Relux oesophagitis (GERD/GORD) • Reflux of gastric contents • Inflammatory changes are due to – Frequent protracted reflux - ? Incompentance of the LES – Disordered oesophageal motility – contact of gastric contents with the oesophagus for longer periods – Elevated acid peptic levels in the gastric fluid
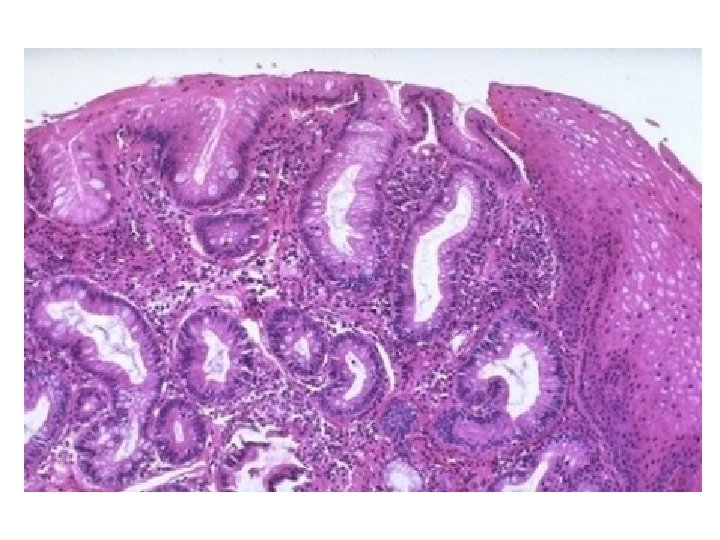
Barrett’s Oesophagus • Congenital / Acqiured (Reflux induced) • Metaplasia of the oesophageal mucosa. • Predisposition to Adenocarcinoma.
Prolonged reflux of gastric contents Inflammation and ulceration of the squamous epithelial lining Healing of the lining by formation of intestinal or gastric type epithelium – metaplasia. This epithelium is better able to withstand the effects of the gastric juices
Can progress to dysplasia and adenocarcinoma Its is an acquired condition due to gastro-oesophageal reflux Bile reflux appears to be an important aetiological factor 10% of patients with GORD develop Barrett's oesophagus Approximately 1% of patients with Barrett's oesophagus per year progress to carcinoma • Barrett's oesophagus increase the risk of cancer by x 30 • • •
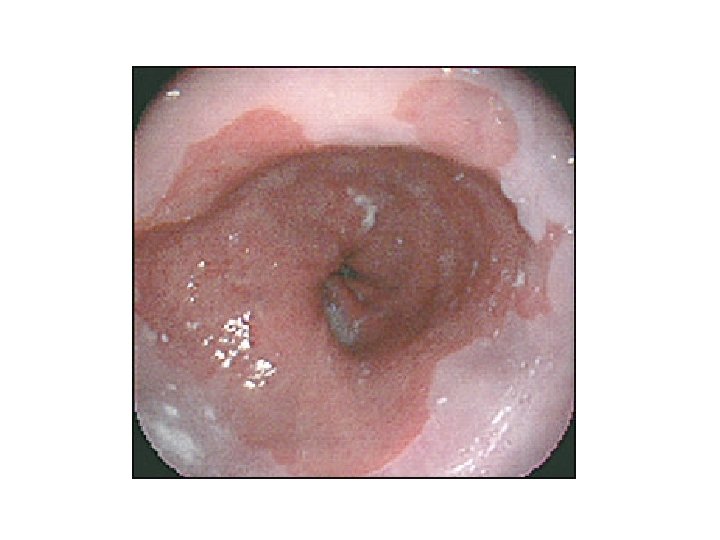
Clinical features • Barrett's per se is usually asymptomatic • Usually recognized as an incidental finding at endoscopy
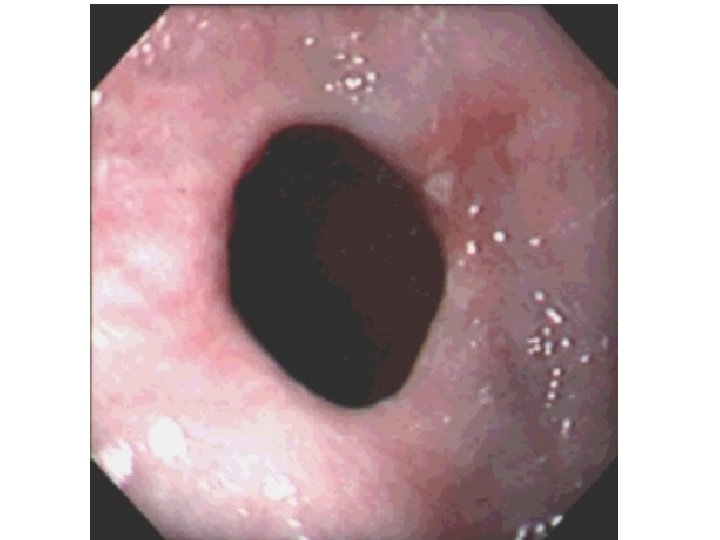
Barrett Esophagus Morphology �Endoscopically, it appears as “tongues” of red, velvety mucosa above the GE junction �Histologically, intestinal metaplasia is composed of goblet cells wit cytoplasmic mucus vacuoles �The diagnosis of Barrett esophagus requires both: Abnormal endoscopic findings and histology of intestinal metaplasia Normal gastroesophageal junction Barrett esophagus
• • Conservative treatment Lifestyle modification Stop smoking Avoid alcohol Loose weight Raise head of bed Drug treatment H 2 antagonists – Provide symptomatic relief in 60% at 6 weeks – Endoscopic evidence of healing seen in only 40% • Proton pump inhibitors – 80% healing at 8 weeks – More than 20% relapse despite maintenance therapy – Long term therapy often required
Surgical options • Indications: – Recurrent symptomatic relapse – Bile reflux – Poor response to pharmacological management • Fundoplication is operation of choice performed as open or laparoscopic procedure
Vascular lesions - Varices • Dilatation of oesophageal submucosal veins due to portal hypertension • Lower 3 rd of the oesophguse • Presents with haematemsis
Strictures of the oesophagus • • Congenital Reflux disease induced strictures Corrosive poisoning Tumors • Rare – Scleroderma
Oesophageal Tumors Benign Leiomyoma Malignant Squamous Carcinoma 85% Adenocarcinoma 15%
Oesophageal Carcinoma • Adults > 50 years • M: F = 4: 1 • Geographical distribution - North China, Iran, USSR, S. Africa
Squamous Carcinoma Predisposing factors – 1. Dietary - fungal contamination, High content of nitrites / nitrosamines, def of Vit & trace metals – 2. Oesophageal disorders - Achalasia cardia, Diverticula, Oesophageal stasis. – 3. Life style - Alcohol, Tobacco – 4, Genetic - Epidermolysis Bullosa, Coeliac disease, Ectodermal dysplasia
Clinical features • PROGRESSIVE DYSPHAGIA UNTIL PROVED OTHERWISE IS CARCINOMA OESOPHAGUS • Regurgitation. • Pain • Loss of weight - BUT NOT LOSS OF APPETITE.
Morphology • Site - Commonest in the middle 3 rd. • Macroscopy – 1. Polypoidal fungating. ) 15% – 2. Nodular mass. ) – 3. Diffuse infiltrative - flat lesion. – 4. Excavated /ulcerated – Superficial (in -situ)
Macroscopic Appearances
Microscopy • Squamous carcinoma. – Cell keratinization – Intercellular bridges /prickles. – Keratin pearls.
Metastases • Blood stream spread is uncommon. - Lung Brain & Bone • Lymph node – Upper 3 rd - Cervical – Middle 3 rd - Mediastinal, tracheobronchial, paratracheal – Lower 3 rd - Gastric & Coeliac node.
Causes of Death • Starvation & wasting. • Tracheo-oesophageal fistula - Aspiration pneumonia. • Rupture - Mediastinitis. • Haemorrhage • Distant spread.
Oesophageal carcinoma 90% are squamous cell carcinomas Occur in the upper or middle third of the oesophagus 8% are adenocarcinomas Occur in the lower third of the oesophagus Overall 5 year survival is very poor and is at best 20% Less than 50% patients are suitable for potentially curative treatment • Of those undergoing 'curative' treatment less than 40% survive one year • • •
Resectability and fitness for surgery assessed by: • Chest x-ray • Lung function tests(FEV 1 > 1 L) • CT thorax & abdomen • Liver ultrasound • Endoscopic ultrasound • Bronchoscopy • Laparoscopy
Management • Adenocarcinomas • surgery is mainstay of treatment • Upfront chemo irradiation may improve survival • Squamous cell carcinomas are more responsive to radiotherapy •
Surgery • Only 40% tumours are resectable • Operative mortality now less than 10% • Treatment should be in centres who perform operation regularly • Preoperative chemotherapy may be beneficial
Operative approaches • Need 10 cm proximal clearance to avoid submucosal spread. • Total oesophagectomy via thoracoabdominal approach (Adenocarcinoma) • Subtotal two-stage oesophagectomy (Ivor-Lewis) • Subtotal three-stage oesophagectomy (Mc. Keown) • Transhiatal oesophagectomy
Palliative treatment • Aim to relieve obstruction and dysphagia with minimal morbidity
Oesophageal intubation – Endoscopic or radiological placement of stents are now most commonly practiced – Recent increased use of self-expanding stents – Complications of stents • Oesophageal perforation • displacement or migration • blockage due to ingrowth or overgrowth
• Laser therapy – Produces good palliation in over 60% of cases – May need to be repeated every 4 to 6 weeks – Associated with oesophageal perforation in about 5% cases • • External beam radiotherapy Brachytherapy Diathermy Alcohol injection
Presentations of oesophageal disorders Symptoms – Dysphagia – Difficulty in swallowing • Organic disease (stricture and carcinoma) • Motilitiy disorders –Dysphagia for liquids more likely – Regurgitation – Odynophagia – localized pain associated with swallowing – Pain • Heart burn – due to reflux • Angina like tightening chest pain – occur in association with meals – Waterbrash – mouth being full of fluid which is salty in taste
Presentations of oesophageal disorders – Atypical symptoms • Anaemia • Pulmonary symptoms – due to aspiration pneumonia in reflux – Coughing – Choking – Repeated chest infections
Presentations of oesophageal disorders – Physical signs • Weight loss • Pallor • Neck swellings – pharyngeal pouch, enlarged lymph nodes • Chest signs on auscultation • Epigastric mass – carcinoma of cardia enlarging down • Others – Tylosis, koilonychia
Evaluation of a patient with dysphagia • • History Physical examination Investigations History Onset Progression Associated symptoms Past history/associated disases
Examination • For the cause – mouth, neck, larynx, neuro • Effects – dehydration, malnutrition investigations • Imaging • Endoscopy and biopsy • Other
endoscopy
videofluorographic swallowing study (VFSS)*
Management Depend upon the cause Definitive vs palliative Endoscopic/surgical Food & Drugs
Surgeries of Oesophagus ( Fundoplication)