Surgical anatomy of the hepatobiliary tract and congenital

Surgical anatomy of the hepatobiliary tract and congenital anomalies Moderated by : Dr. Shreesha Rao Presented by : Dr. Muddappa P. P.

Dimensions • The healthy adult liver weighs between 1. 0 kg and 2. 0 kg • Anteroposteriorly, the distance extends 10. 0 cm to 12. 5 cm from the area related to the anterior abdominal wall to its rounded posterior surface • The transverse diameter is 20. 0 cm to 25. 5 cm from the right paracolic gutter to the midpoint of the left diaphragmatic leaflet • The anteroinferior edge stretches vertically 15. 0 cm to 17. 5 cm to the top of the dome of the right hepatic lobe

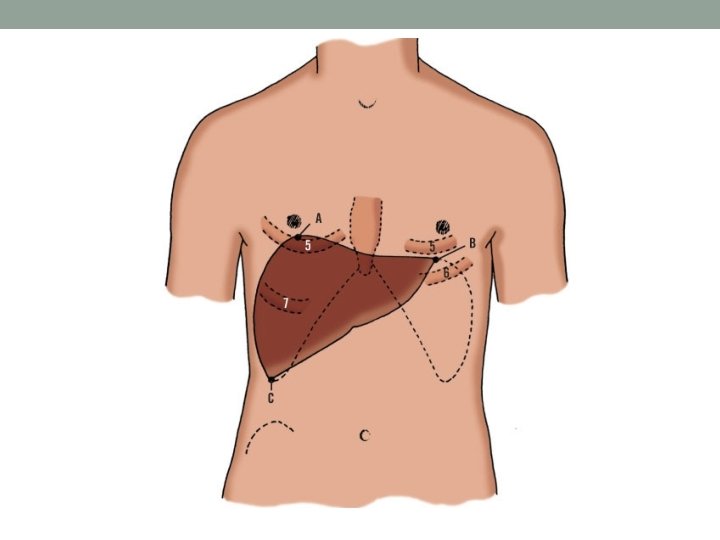
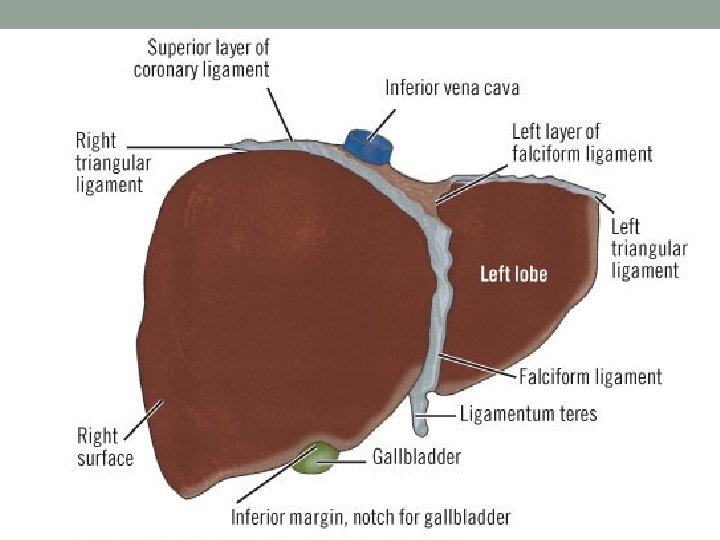
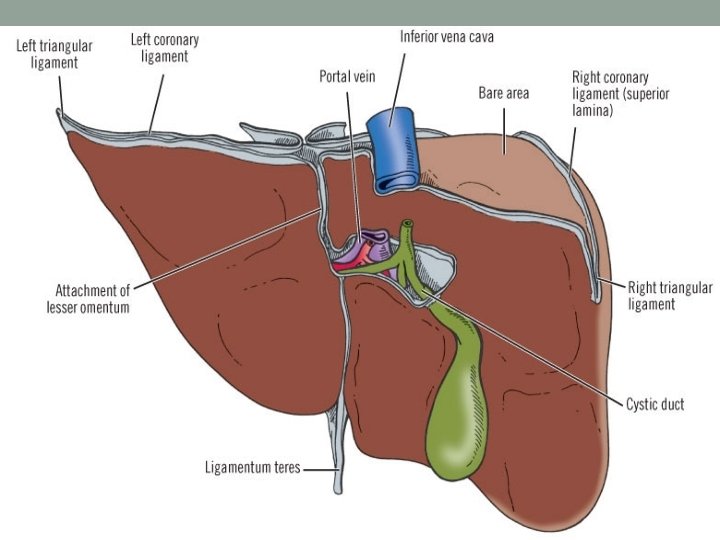
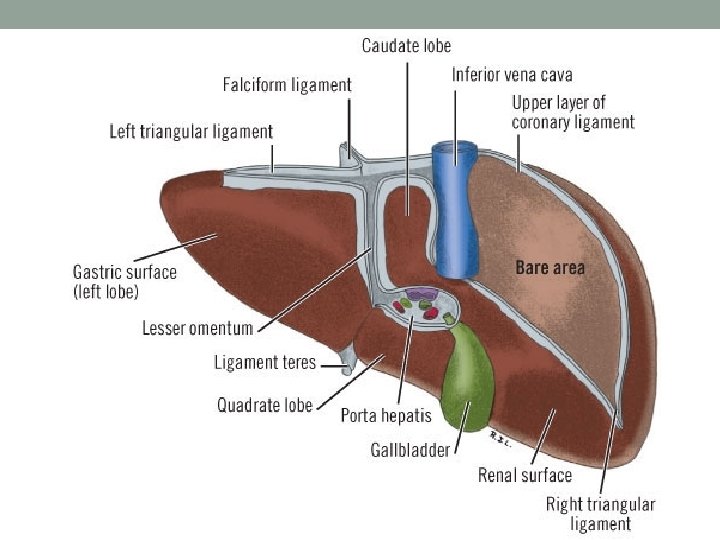
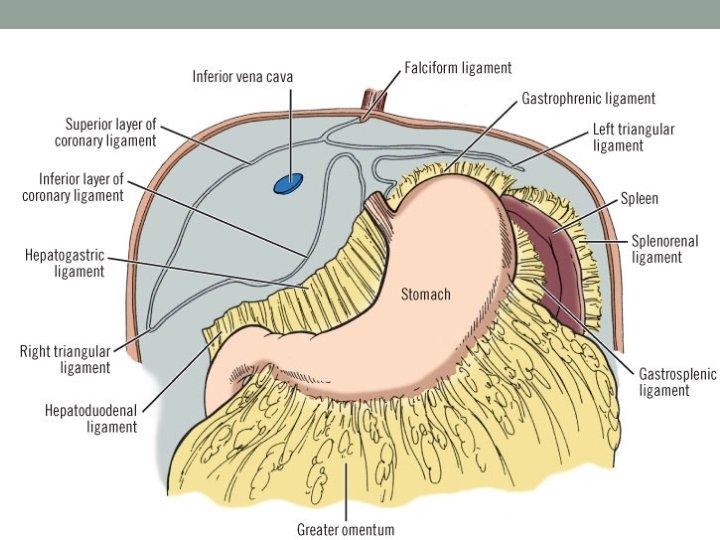
Relations
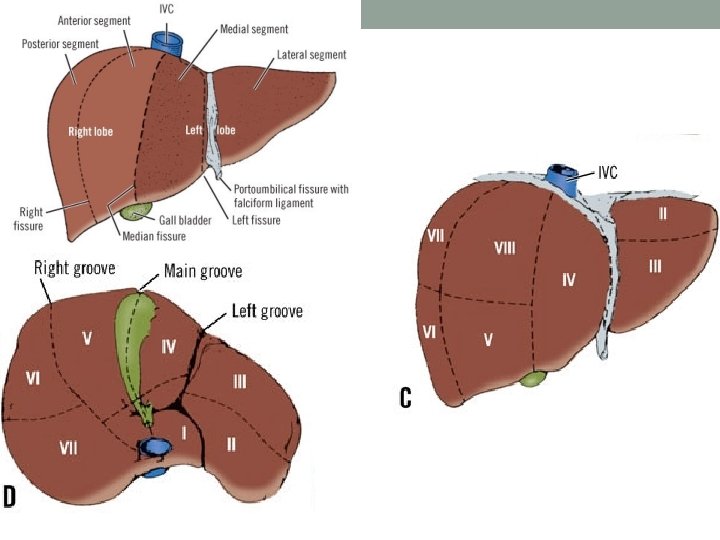

Segments Couinaud, 1957 Goldsmith & woodburne, 1957 Brisbane, 2000 V-VIII Rt hepatectomy Rt hepatic lobectomy Rt hemi-hepatectomy IV-VIII Rt lobectomy Extended Rt hepatic lobectomy Rt trisectionectomy II-IV Lt hepatectomy Lt hepaticlobectomy Lt hemi-hepatectomy II, III Lt lobectomy Lt lateral segmentectomy Lt lateral sectionectomy II, IV, V, VIII Extended Lt hepatectomy Lt trisectionectomy

Congenital Anamolies • Complete absence of the liver • Transposition – situs inversus • Anomalous lobes of the liver • • • - Riedel’s lobe - Supradiaphragmatic liver - Accessory or ectopic lobes Mesenchymal hamartoma Intrahepatic biliary atresia Cysts Congenital hepatic fibrosis Vascular malformations - Solitary hemangiomas - Multiple hemangioendothelioma

Common hepatic duct • The common hepatic duct is formed by the union of the right and left hepatic ducts in the porta • Its lower end is defined as its junction with the cystic duct. • The distance between these points varies from 1. 0 cm to 7. 5 cm. • The diameter of the duct is about 0. 4 cm.

Right hepatic duct • The right hepatic duct is formed by the union of the anterior and posterior segment ducts at the porta hepatis.

Left hepatic duct • The left hepatic duct is formed by the union of the medial and lateral segment ducts

Variations and Anomalies of the Biliary Ducts Extrahepatic Biliary Atresia • Congenital biliary atresia is the most serious malformation of the biliary tract. • A short segment, an entire duct, or the whole system may be atretic. • All possible combinations may be encountered. • The atretic duct may be hypoplastic, stenosed, or reduced to a fibrous band
 • A local balloon-shaped or")
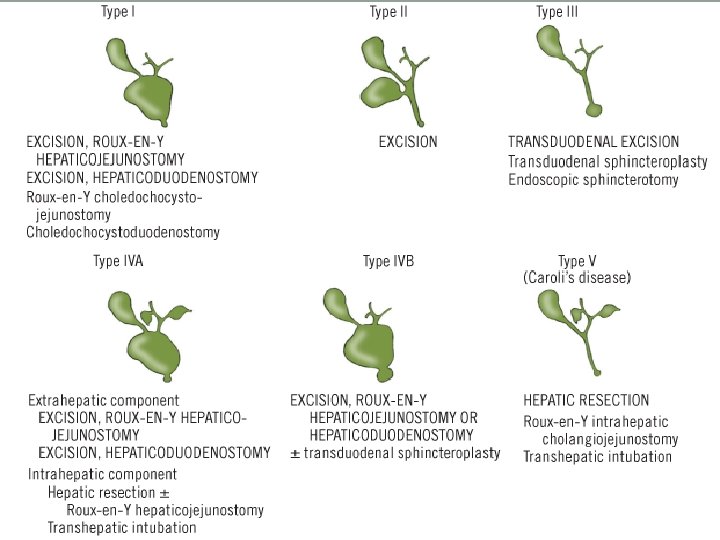
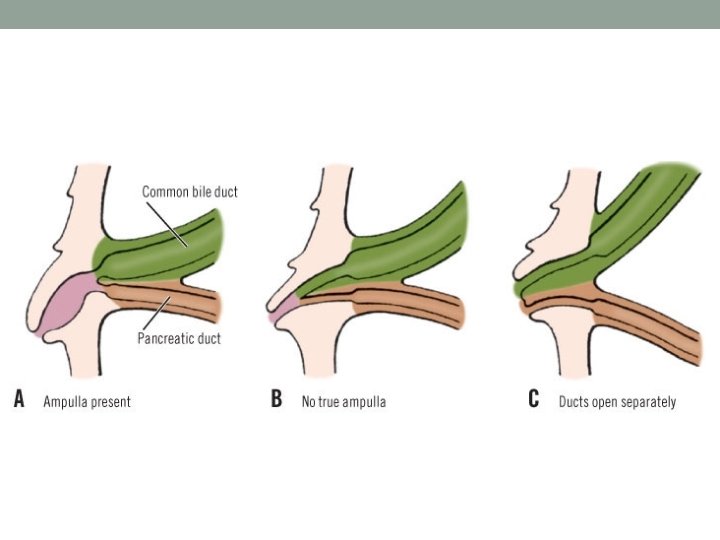
Congenital Dilatation of the Common Bile Duct (Choledochal Cysts) • A local balloon-shaped or cylindrical enlargement of the common bile duct is probably congenital • Todani's classification of five types of choledochal cysts is summarized as follows I, Solitary fusiform extrahepatic cyst.

II, Extrahepatic supraduodenal diverticulum. Double gallbladder, with one element sessile without cystic duct III, Intraduodenal diverticulum/choledochocele. Cystic biliary dilatation within the duodenal wall (5%)
 V,")
IV, Any combination of multiple cysts, i. e. , types I, III (10%) V, Caroli's disease/multiple intrahepatic cysts (very rare)

Miscellaneous Asymptomatic Anomalies • Variations of hepatic ducts. A, Intrahepatic union of right and left hepatic ducts. B, Extrahepatic (normal) union of hepatic ducts. C, Distal union of hepatic ducts resulting in absence of common hepatic duct.

• Accessory hepatic duct

• Duplication of common hepatic duct

• Duplications of common bile duct

• A, Absence of cystic duct, with sessile gallbladder. • B, Atretic cystic duct with normal gallbladder
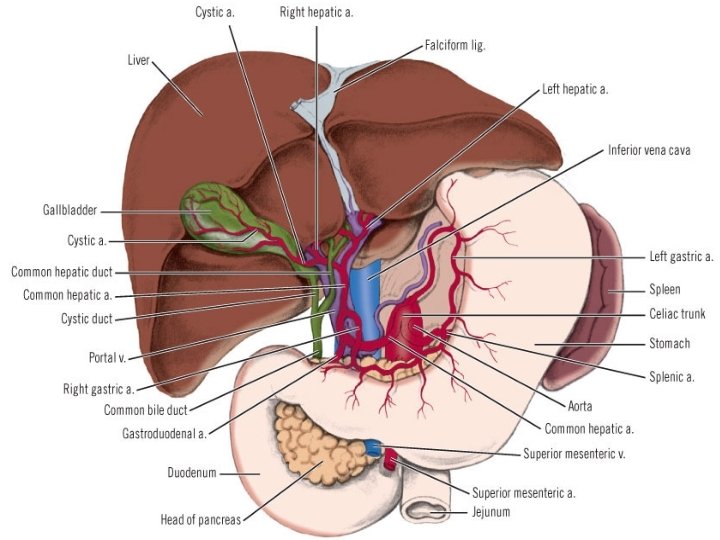

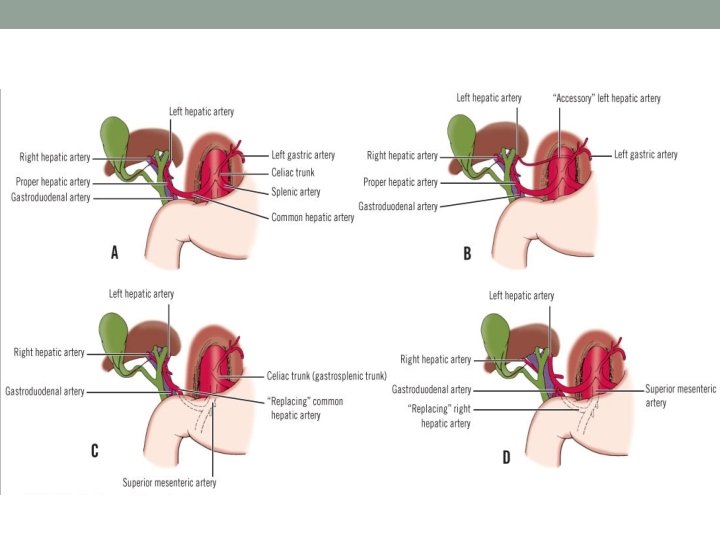
Hepatic artery

Portal vein

Portal vein anomalies • Anterior to neck of pancreas and duodenum • Enter directly into IVC • Absence of left portal vein

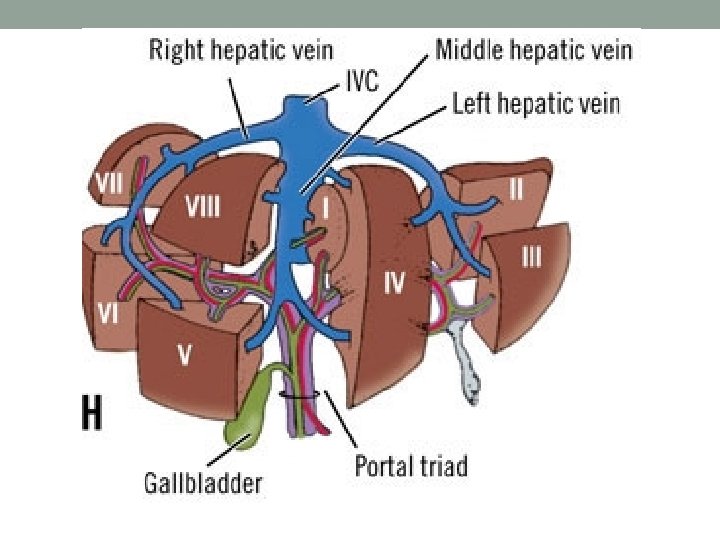
Hepatic vein • Right hepatic vein drains – Most of Rt side of liver (segment VI, VII, most of V & VIII) • Left hepatic vein drains – Segment II & III • Middle hepatic vein drains – Segment IV and segments V & VIII • Middle hepatic vein drains to left hepatic vein or directly to IVC • Caudate lobe drains directly to IVC or left hepatic vein

Lymphatic drainage of the liver & biliary tract • Most of the lymphatic drainage of the liver is to the hepatoduodenal ligament, celiac nodes and cisterna chyli • Follow the hepatic veins to lymph nodes in the area of the suprahepatic inferior vena cava and through the diaphragmatic hiatus • Gallbladder and most of the extrahepatic biliary tract drain into hepatoduodenal ligament. Can also drain to nodes behind head of pancreas or in the interaortocaval groove

Innervation of the liver & biliary tract • Receives both sympathetic from T 7 to T 10 and parasympathetic fibers from both vagal nerves • Sympathetic innervation is through the celiac ganglion • Rt celiac ganglion & Rt vagus form anterior hepatic plexus and run along the hepatic artery • Lt celiac ganglion & Lt vagus form posterior hepatic plexus and runs posterior to bile duct & portal vein

Gall bladder • Measures about 7 to 10 cms in length • 3 to 5 cms in diameter • 30 to 60 ml in quantity • Located in the inferior surface of segment IV & V

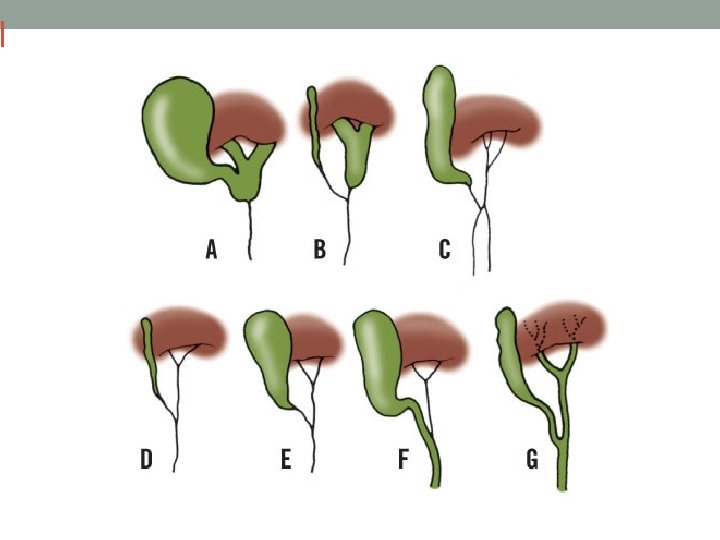
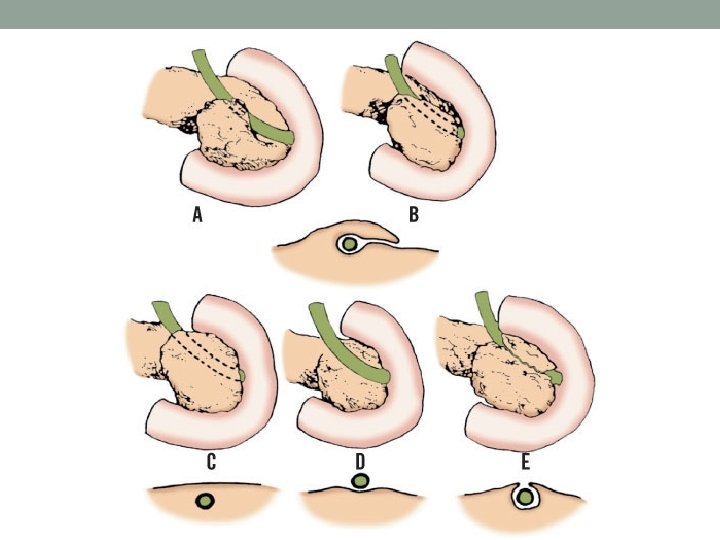
Multiple Gall Bladder • Split Primordium Group Septate gallbladder - A & B Bilobate "V" gallbladder - C "Y" duplication – D & E

Multiple Gall Bladder • Accessory Gallbladder Group Ductular "H" duplication – A & C Trabecular duplication – D & E Triple gallbladder

Absence of Gall Bladder

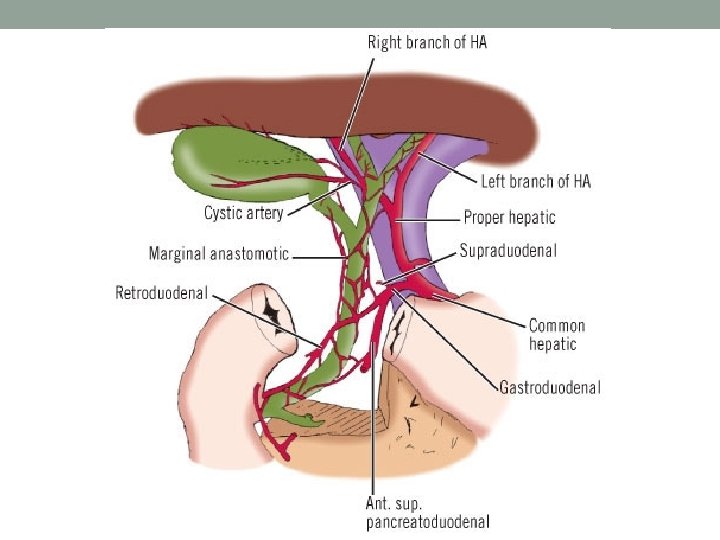
Cystic artery

Calot’s triangle

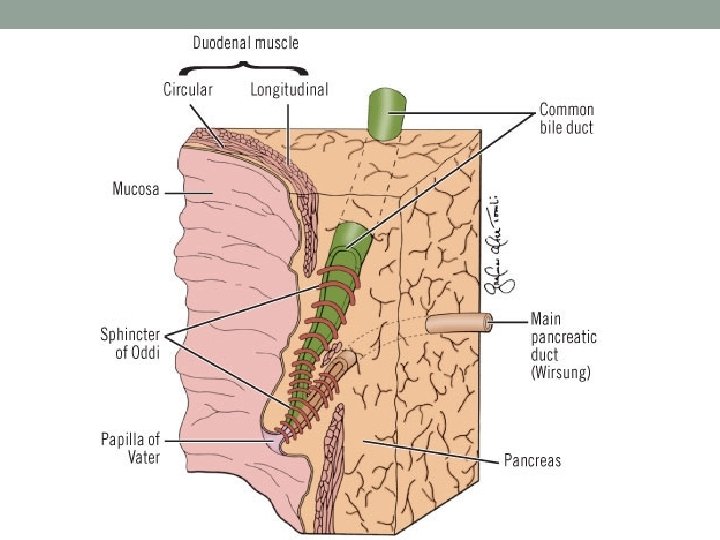
Common Bile Duct

Venous drainage of the gall bladder & CBD • They follow the vessels which supply them and do not drain directly to the portal vein

Muddappa. P. P
- Slides: 47