Surgical abdomen Preparation for Finals Casebased Learning Tutor

Surgical abdomen Preparation for Finals – Case-based Learning Tutor name

Tu. BS attendance • https: //tutorialbooking. com/

Session overview • • Common surgical conditions for the OSCE How to present your findings Overview of clinical signs/surgical scars Case presentations and viva questions

What is the purpose of an OSCE? “This station tests a student’s ability to perform an appropriate focussed physical examination, demonstrating consideration for the patient, and to report back succinctly describing the relevant findings. It also tests a student’s clinical judgement i. e. the ability to decide the differential diagnosis, choose investigations and formulate a management plan. ”

Common surgical conditions in the OSCE • Hernias • Stomas • Surgical scars

Presenting your findings • • • What were you asked to do? What were your key positive findings? What were the important negative findings? What does this mean? How would you complete your examination, and what investigations would you do?

Example case presentation • • • I was asked to examine the abdomen of this ___ year old ___ On examination this patient has a mass in the right groin. It is medial to and above the pubic tubercle, and did not reappear after being reduced when the deep ring was occluded. Bowel sounds were auscultated over the mass. I therefore think this is a direct inguinal hernia. My differential would include an indirect inguinal hernia and a femoral hernia.

Completing your examination • Examine the contralateral groin • Transilluminate the mass • Full GI examination in particular look for causes of raised intraabdominal pressure

Investigations • Bedside • ECGs, urine dip, spirometry • Bloods and urine • Biochemistry, haematology, M, C&S • Imaging • Plain XR, CT, MRI, US, echo • Other • Biopsy

Clinical signs Practise presenting!






Abdominal scars • Present what you see, described the scar if you do not know the name • Give a differential diagnosis

Presentation of a surgical scar • Describe: this is a xxx incision which is consistent with a previous xxx such as a xxx • Age - old or new? • Healing - well healed, hypertrophic or keloid? • Complications - infected or dehisced? Evidence of incisional hernia?

Scar 1

Scar 1 • Mercedes-Benz incision • Major upper GI or HPB surgery • E. g. liver transplant , Whipples procedure

Scar 2

Scar 2 • Midline laparotomy • Major intra-abdominal surgery

Scar 3

Scar 3 • Laparoscopy ports • 1 port = diagnostic laparoscopy

Scar 4

Scar 4 • Rutherford-Morrison incision • Renal transplant

Scar 5

Scar 5 • Loin incision • Renal surgery • E. g. nephrectomy

Scar 6

Scar 6 • Pfannenstiel incision • Open gynae surgery • E. g. C-section

Scar 7

Scar 7 • Suprainguinal incision • Open mesh repair of inguinal hernia

Scar 8

Scar 8 • Lanz incision • Appendicectomy • Lanz now favoured as hidden in skin creases compared to Gridiron which is more oblique

Scar 9

Scar 9 • Kocher’s incision • Open cholecystectomy

Scar 10

• Laparoscopy ports Scar 10 • Laparoscopic cholecystectomy

Case 1

Please present your findings.

Case 1 - general • Middle aged man, with walking stick • Very slim • No lymphadenopathy

Case 1 - abdomen

Case 1 – more abdo • • Abdo soft, non tender No palpable masses Bowel sounds normal Legs normal Please present your findings.

Case 2

Case 2 - general 45 Year old male, on examination…. Looks well at rest, average BMI. Face – Pale conjunctivae Legs – Nil of note

Case 2 - abdomen • • • Palpable mass in LIF – 8 x 6, smooth Tender Bruit present overlying it No other masses No other organomegaly, non-palpable bladder Bowel sounds present, normal

Case 3

Case 3 observation Case 2 65 Year old male, on examination…. Looks well at rest, high BMI.

Case 3 - abdomen • • Abdomen soft Liver edge palpable 3 cm below costal margin No spleen/kidneys/bladder Bowel sounds present Please present your findings.

What is a hernia? ‘a protrusion of a viscus through a defect of the walls of its containing cavity into an abnormal position’

Describe the anatomy of the inguinal canal • Deep ring = midpoint of inguinal ligament (halfway between ASIS and PT) • Superficial ring = above PT • Femoral pulse at mid-inguinal point (halfway between ASIS and PS) • Hesselbachs triangle = inferior epigastric artery, rectus abdominus, inguinal ligament

Anatomy of the inguinal canal • Walls of the inguinal canal • • Floor = inguinal ligament Roof = internal oblique Anterior = external oblique Posterior = transversalis fascia

What is your differential diagnosis for a groin lump? • • • Hernia – inguinal, femoral, other Vascular: saphena varix, femoral artery aneurysm Lymph node Psoas abscess Undescended testes

How would you tell a direct from an indirect hernia? Very inaccurate but liked in exams • Reduce hernia and cover the deep ring with fingers then ask to cough… • Hernia controlled = indirect • Not controlled = direct

What are the complications of a hernia? • Incarceration/irreducibility • Obstruction • Strangulation

Describe the demography of hernias Direct inguinal Indirect inguinal Femoral Men Above and medial to PT 20% inguinal Older – weak muscle wall Superficial ring Through Hesselbachs triangle Rarely descend into scrotum Rarely strangulate Men Above and medial to PT 80% inguinal Younger – PPV Deep ring Have all 3 layers and descend into scrotum Women (wider femoral canal) Below and lateral to PT Often irreducible Frequently strangulate

Richter’s hernia • Rare but dangerous • Part, not all, of bowel wall herniates • Therefore do not obstruct, but can strangulate

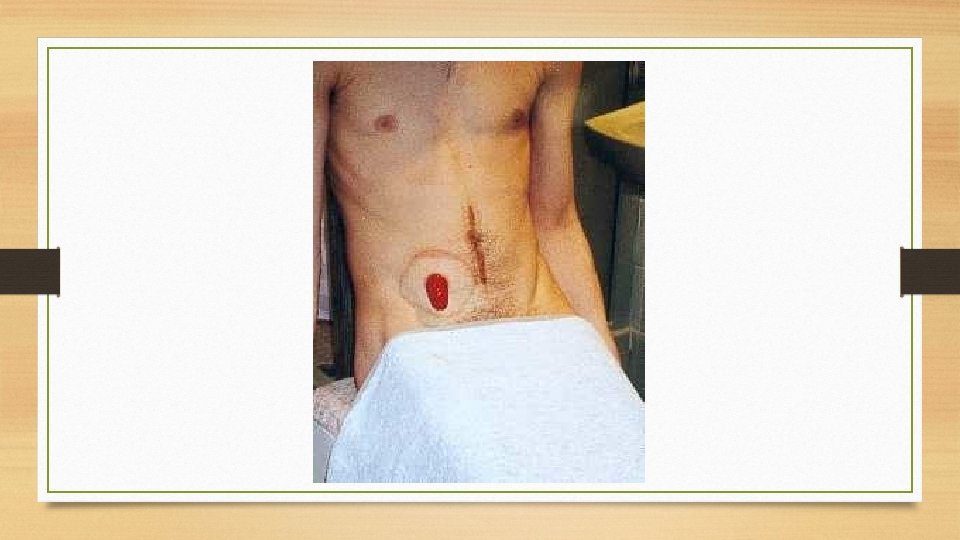
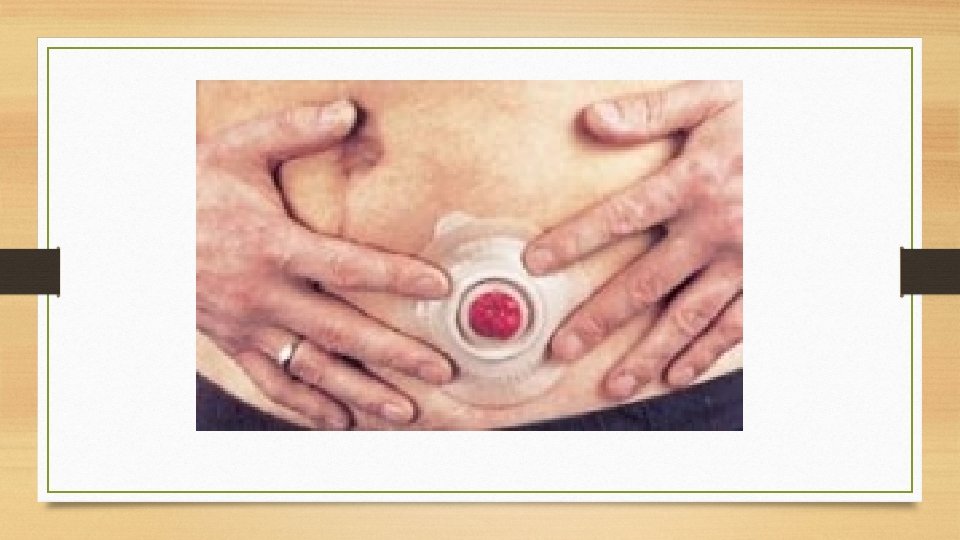
What is a stoma? ‘an artificial union between conduits or between a conduit and the outside’ • Greek for ‘mouth’

What are the different types of stoma? Content Site Surface Ileostomy Liquid stool RIF Spout Colostomy Formed stool LIF Flush Urostomy Urine RIF Flush

End vs defunctioning stomas

How can you tell what operation someone with a stoma has had? • Colostomy… • Hartmanns (temporary) or AP resection (permanent) • Ask if they still have an anus • Ileostomy… • Panproctocolectomy (permanent) • Anterior resection (temporary)

Previous OSCE stations • • AAA managed by EVAR Kidney transplant Liver transplant Laparoscopic port site scars Colostomy Ileostomy Urostomy Hernias

Summary • • Common surgical conditions for the OSCE How to present your findings Overview of clinical signs/surgical scars Case presentations and viva questions

Please complete Tu. BS feedback • Tutor details • For more information on Examining for Finals sessions: • examiningforfinals@gmail. com • www. sefce. net/pulse • With thanks to previous contributors: • Dr Emma Claire Phillips (FY 2) • Dr Kristina Lee (FY 2) • Dr Aman Shams (GI Sp. R)
- Slides: 65