SURGERY IN PAEDIATRIC RHEUMATIC CARDITIS DR VILJEE JONKER







 HYSTOLOGICAL Exudative, inflammation Fibrinoid degeneration (lasts 2 -3")






























- Slides: 39
SURGERY IN PAEDIATRIC RHEUMATIC CARDITIS DR VILJEE JONKER DEPT CARDIOTHORACIC SURGERY YUNIVESITHI YA FREISTATA
NATURAL HISTORY n n n ARF : 5% < 5 y Rare >35 y 85% ARF major manifestations- Carditis Valvar disease rather than myocarditis M&M Thomas: if no heart disease in hosp/ no recurrence – no cardiac involvement @ 15 y If no recurrence up to 68 -76% MR may disappear; less likely if cardiomegaly MS only after 3/ more attacks Carapetis, JR: Lancet 2005; 366: 155 -68 Antunes MJ: Mitral valve repair; 31 -43 Thomas, GT: Br Med J I: 1961; 1635
PATHOGENESIS Lancefield Group A B -hemolytic Streptococcus pharyngitis n Auto-immune response n Post n Factors dictate attack rate of RF § Quantitative factors § Variations in Group A Strep infections § Geography § Host factors Braunwald, E : Heart Disease; 1706 -17 Walter, JB: Pathology of human disease; 471 -74
n Antibodies § § Streptolysin O Streptokinase DNA’se Hyaluronidase AB’s initial endothelium damage activates lymphocyte adhesion molecules n AB’s cross react n § Cardiac myocin in myocardium § Laminin on valve surface (laminin=Strep M Protein) n Laminin & other cross reactive protein trap AB on valve surface
Cunningham, Int Congrss Series 2006; 1289: 14 -19
n VCAM upregulated on valve surface promotes lymphocyte adhesion-respond to Strep M Protein n Repetitive Strep infections through neovascularised scar n Repeat infection necessary to prime immune response Cunningham, Int Congrss Series 2006; 1289: 14 -19
Cunningham, Int Congrss Series 2006; 1289: 14 -19
3 Stages IMMUNOLOGICAL Acute ( Active) HYSTOLOGICAL Exudative, inflammation Fibrinoid degeneration (lasts 2 -3 w) Proliferative/ Healing Granulomatous, exudative degenerative Progressive fibrosis Braunwald, E : Heart Disease; 1706 -17
Carapetis, Lancet 2005; 366: 155 -68
PATHOLOGY: AUTE CARDITIS n Pericarditis § “bread and butter”, fibrous exudate § NO Constriction
n Myocarditis § Remarkably normal § Aschoff lesions § Interstitial cellular infiltrate, oedema Antunes MJ: Mitral valve repair; 31 -43 Walter, JB: Pathology of human disease; 471 -74
n Endocarditis § Verrucous lesions -MV: Atrial aspect -AV: Ventricular aspect – DO NOT EMBOLISE Antunes MJ: Mitral valve repair; 31 -43 Walter, JB: Pathology of human disease; 471 -74
§ Annular dilation- Ant valve prolapse- chordal enlongation § Mac. Cullum’s Patch: MR jet leads to posterior leaflet LA thrombus deposition Antunes MJ: Mitral valve repair; 31 -43
n Thickening and fusion of Triangular base of chordae tendineae Antunes MJ: Mitral valve repair; 31 -43
CHRONIC PHASE n Depends on original involvement & predominant healing process n Fibrous tissue- commisural fusion/ contraction leaflets n Calcification
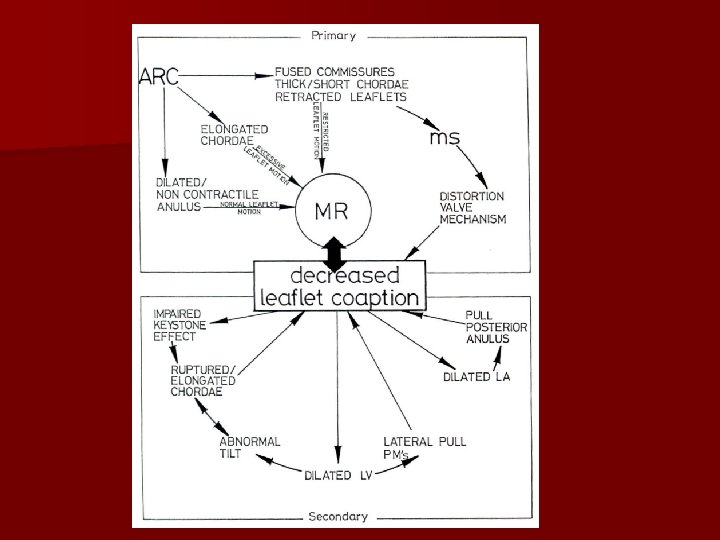
PATHOPHYSIOLOGY MITRAL VALVE n Carpentier: – Normal leaflet Motion – 88% – Excessive leaflet motion- 73% ( co-exist in 78%) – Restricted leaflet motion n MR § § n Annular Dilation Enlongation/ rupture of chordae Restricted movement post leaflet Secondary Ventricular dilation (MR begets MR) MS § Rare 2 -10 y – recurrent attacks § Commisural fusion § Both leaflets, chordae thickened
AORTIC VALVE n 25 -30 % Children with severe RHD n AR – Annular dilation – Leaflet retraction n AS – Commisural fusion Hillman, ND: Ann Thorac Surg 2004; 78: 1403 -8
SURGERY REPAIR VS REPLACEMENT
n Repair n Replacement – – – – – Safe Allows annulus growth (annuloplasty dependent) Preserves chordal/ ventricular function No anticoagulation (Pt compliance) Worse haemodinamics Thrombo-embolism Anticoagulation Growth of annulus impaired Rapid degeneration bioprosthesis Unsuitability of Pulmonary autograft Kumar, S: Ann Thorac Surg 2005; 79: 1921 -5 Essop, MR: Circulation 2005; 112: 3584 -91
SURGERY: MV Repair – ANNULAR DILATION § § Annuloplasty Ring > 28 -30 mm Partial/ posterior annuloplasty Teflon felt annuloplasty Kolangos – COMMISSURAL FUSION § Commissurotomy – VALVE § Cusp thinning & leaflet enlargement – CHORDAE § Cusp-level shortening & transfer Kumar, S: Ann Thorac Surg 2005; 79: 1921 -5
Cuspal thinning
Annuloplasty Ring
Chordal shortening
Chordal Transfer
Posterior Leaflet extension
Commisuroplasty
Posterior Commisuroplasty
Video
MITRAL VALVE REPAIR Kumar-2005 – 278 Pt Age 2 – 15 y – Reoperation 6% @ 56 m FU – Mortality 4. 8% Carpentier-2001 – 951 Pt Subgroup < 19 y – Reoperation 19% @ 10 y FU – Total Mortality 6. 2% (early 2%) Kumar, S: J Cariovasc Surg 2005; 129: 875 -9 Carpentier, A: Circulation 2001; 104(1): 1 -15
Grinda-2002 – 21 Pt Mean age 11+-4 y – Reoperation 10% 5 y FU – Mortality 4. 7% Hillman- 2004 – 26 Pt Age: <21 y – Reoperation 23% @ 5. 3 +-3. 3 y – Mortality (late 7. 7%) Hillman, ND: Ann Thorac Surg 2004; 78: 1403 -8 Grinda, J: Eur J Cardiovasc Surg 2002; 21: 447 -52
n Cause of failure – Judgment error – Inherent complexity of disease – Recurrence/ progression of disease n Treatment post repair – Regular FU – 3 weekly IMI Bensatine Pen till 40 y Hillman, ND: Ann Thorac Surg 2004; 78: 1403 -8 Carpentier, A: Circulation 2001; 104(1): 1 -15 Kumar, S: Ann Thorac Surg 1995; 60: 1044 -7
AORTIC VALVE REPAIR n Criteria for possible repair – – – n Minimal/ no calcifications Mobility >2 -3 mm of central coaptation TECHNIQUES – – Subcommissural annuloplasty Cusp thinning Commissural plication- Trusler Leaflet extension Hillman, ND: Ann Thorac Surg 2004; 78: 1403 -8 Kumar, S: Ann Thorac Surg 2005; 79: 1921 -5
Commissuroplasty
Cuspal thinning
Leaflet extension
REPALCEMENT n Mitral valve – Bioprosthesis – Homograft – Metallic valve n Aortic valve – Bioprosthesis – Ross – Metallic - early degeneration - midterm failure
AV + MV n REPLACE BOTH Kuwaki, K 2007: Ann Thorac Surg 2007; 83: 558 -63
Conclusion n Patient repair selection determines success of n Surgery n Active for decompensated ARC carditis: ? replacement