Surgery for Diabetes Michel Gagner MD FRCSC FACS

Surgery for Diabetes. Michel Gagner MD, FRCSC, FACS Clinical Professor of Surgery, Florida International University , Miami, FL , Hopital du Sacre-Coeur (University of Montreal), Montreal, QC, Canada, Hamad General Hospital, Doha Qatar.

Obesity & T 2 DM Prevalence United States World Wide 2007 *2015 70 M 135 M 400 M 700 M Severe obese 16 M 32 M 75 M 130 M T 2 DM 30 M 180 M 320 M Obesity 22 M World Wide Diabetic 180 Mil In the United States Obese 400 Mil Obese 70 Mil Diabetic 22 Mil Severely Obese 75 Mil Diabetic& Severely Obese 16. 5 Mil Severely Obese 16 Mil Diabetic& Severely Obese 3 Mil Diabetic &Obese 14 Mil * 2015 estimates based on review of published health care industry trends Diabetic &Obese 54 Mil

Disease Overviews T 2 DM Ø 180 million worldwide, 22 million in the U. S. Ø 54 million with pre-diabetes in the US Ø Fifth largest cause of death in the U. S. Ø Estimated 30% T 2 DM are not obese in the U. S. Ø Estimated 70% T 2 DM are not obese outside the U. S. Ø Comorbidities include CVD, PVD, blindness, lower limb amputation, kidney failure and nervous system diseases Ø No cures other than weight loss surgery

Disease Burden of Diabetes Mellitus • • Leading cause of blindness (12. 5% of cases) Leading cause of ESRD (42% of cases) 50% of all non-traumatic amputations 2. 5 x increase risk of stroke 2 -4 x increase in cardiovascular mortality DM responsible for 25% of cardiac surgeries Mortality in DM: 70% due to Cardiovascular disease

U. S. Annual Cost Estimates Ø Twin Global Epidemics Ø Major Drivers of Healthcare Costs Worldwide T 2 DM (2002) Obesity (2001) $132 Billion $117 Billion - $92 Direct - $61 Direct - $40 indirect - $56 indirect

Surgery should be an accepted option in people who have type 2 diabetes and a BMI of 35 or more. Surgery should be considered as an alternative treatment option in patients with a BMI between 30 and 35 when diabetes cannot be adequately controlled. In Asian, and some other ethnicities of increased risk, BMI action points may be reduced by 2. 5 kg/m 2.

Ideal Operation? Easy to perform Low early mortality and morbidity Low Micronutrient deficiencies High resolution of T 2 DM Possible reoperation/conversion in case of failures

Surgery for Obesity in 2012 4 operations Lap band Sleeve gastrectomy Gastric bypass Duodenal switch
, 2004")
Efficacy Outcomes for Weight reduction Kg/m 2 Buchwald et al. JAMA, 292(14), 2004

Efficacy for Improvement in Diabetes-Related Outcomes by Surgical Procedure % Buchwald et al. JAMA, 292(14), 2004

Adjustable Gastric Banding and Conventional Therapy for Type 2 Diabetes A Randomized Controlled Trial John B. Dixon, MBBS, Ph. D; Paul E. O’Brien, MD; Julie Playfair, RN; Leon Chapman, MBBS; Linda M. Schachter, MBBS, Ph. D; Stewart Skinner, MBBS, Ph. D; Joseph Proietto, MBBS, Ph. D; Michael Bailey, Ph. D, MSc(stats); Margaret Anderson, BHealth. Man JAMA. 2008; 299(3): 316 -323.
")
Percentage of Weight Loss Achieved Over the 2 -Year Study Period (n = 60) and Individual Weight Measures at Baseline and at 2 Years Dixon, J. B. et al. JAMA 2008; 299: 316 -323.

Primary and Secondary Outcomes at 2 Years Remission of Diabetes was 73% vs 13% JAMA. 2008; 299(3): 316 -323. Copyright restrictions may apply.

T 2 DM & THE METABOLIC EFFECTS OF BARIATRIC SURGERY Laparoscopic Gastric Bypass & T 2 DM Fasting insulin (p. M) over time Fasting glucose (m. M) over time Diabetes P<0. 001 P<0. 171 Adapted from Wickremesekra K. et. al. Obes Surg 2005 14 |
: 236 -42")
Rubino, Gagner, et al. Ann Surg 2004; 240(2): 236 -42
: 236 -42")
Rubino, Gagner, et al. Ann Surg 2004; 240(2): 236 -42
: 236 -42")
Rubino, Gagner, et al. Ann Surg 2004; 240(2): 236 -42
: 631")
Patients requiring oral hypoglycemics after surgery J Am Coll Surg. 2007 Nov; 205(5): 631 -5.

T 2 DM & THE METABOLIC EFFECTS OF BARIATRIC SURGERY The Entero-insular Axis 1967 – Gastric Bypass 19 | Rehfeld J, 2004

T 2 DM & THE METABOLIC EFFECTS OF BARIATRIC SURGERY The Entero-insular Axis The Foregut Theory Exclusion of the duodenum results in inhibition of a “putative”signal that is responsible for insulin resistance and/or abnormal glycemic control (T 2 DM) Rubino et. al, Ann Surg, 2006 20 |

T 2 DM & THE METABOLIC EFFECTS OF BARIATRIC SURGERY The Entero-insular Axis The Hindgut Theory The more rapid delivery of undigested nutrients to the distal bowel upregulates the production of L-cell derivatives like GLP-1 Mason E. Obes Surg 2005 15, 459 -461 Rubino et. al, Ann Surg, 2006 21 |

T 2 DM & THE METABOLIC EFFECTS OF BARIATRIC SURGERY The Adipo-insular Axis Epidemiologic/scientific evidence supports the association of visceral adiposity and insulin resistance/diabetes and mortality Moderate debate about significance of visceral versus subcutaneous adiposity “Theoretical” mechanisms of action Increased release of free fatty acids into portal circulation Abnormal expression of fat-derived peptides Gabriely I. Diabetes 2002 Nielsen S. J Clin Invest, 2004 22 |

T 2 DM & THE METABOLIC EFFECTS OF BARIATRIC SURGERY The Adipo-insular Axis Fat-derived peptides – “Adipokines” TNF-alpha – impairs insulin signaling pathways / suppresses adipocyte differentiation Leptin – enhances insulin action / anorexigenic Resistin – Known to be elevated in obesity / IR – unknown action Adiponectin - enhances insulin action / glucose clearance / fatty acid oxidation IL-1/ IL-6 – undefined activity Pitombo C. Unpublished manuscipt 23 |
 • Glucagon-like peptide-1 (GLP-1) • Peptide")
Endocrine Changes in Obesity • Ghrelin (orexigenic hormone) • Glucagon-like peptide-1 (GLP-1) • Peptide tyrosine-tyrosine (PYY 3 -36)

Ghrelin Produced in gastric fundus and intestine n Appetite stimulant n Elevated in states of hunger n Rapid decline post-prandially n Ghrelin secretion suppressed by RYGB n Exclusion of gastric fundus? n

Human Ghrelin
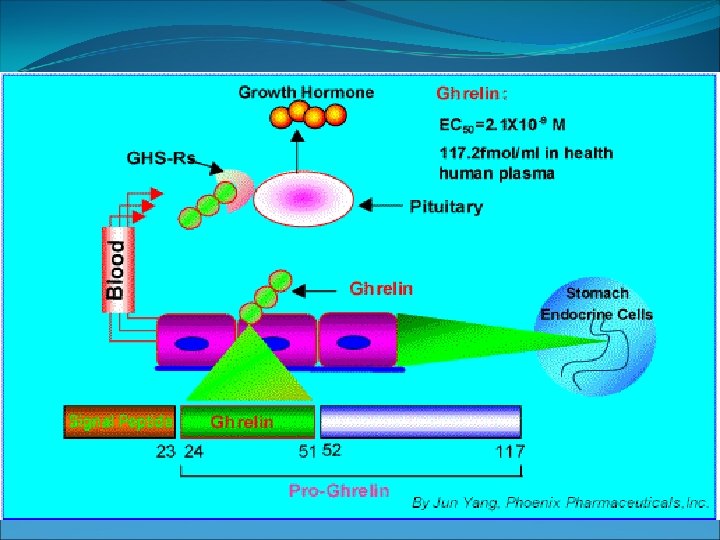

Research reported in New England Journal of Medicine – May 23, 2002 Conducted by VA Puget Sound Health Center & University of Washington – led by Dr. David Cummings -Endocrinologist Compared blood samples after six month period of time of two groups of obese patients 13 dieters & 5 gastric-bypass patients Dieters were on low-fat, low-calorie diet

Ghrelin and Gastric bypass
 Synthesized and released from")
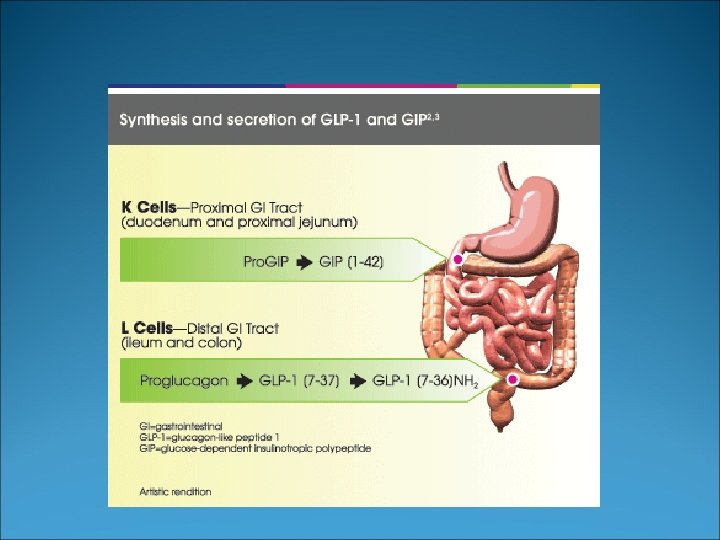
Peptide YY 3 -36 Found in distal GI tract (ileum) Synthesized and released from specialized endocrine cells (L cells) Levels increase with nutrient ingestion/ “ileal brake” Peak at 1 hour Remain elevated for 6 hours

Caloric intake after PYY injection l Batterham et al. NEJM 2003

PYY 3 -36 and Gastric Bypass

PYY 3 -36 in LGB and LSG n : 10

%EWL Ann Surg 2008; Feb. PYY

Effects of GLP-1 on food intake

Glucagon Like Peptide -1 Bypass Sleeve Medical

Ideal Operation? High resolution of T 2 DM Easy to perform Low early mortality and morbidity Low Micronutrient deficiencies Possible reoperation/conversion in case of failures

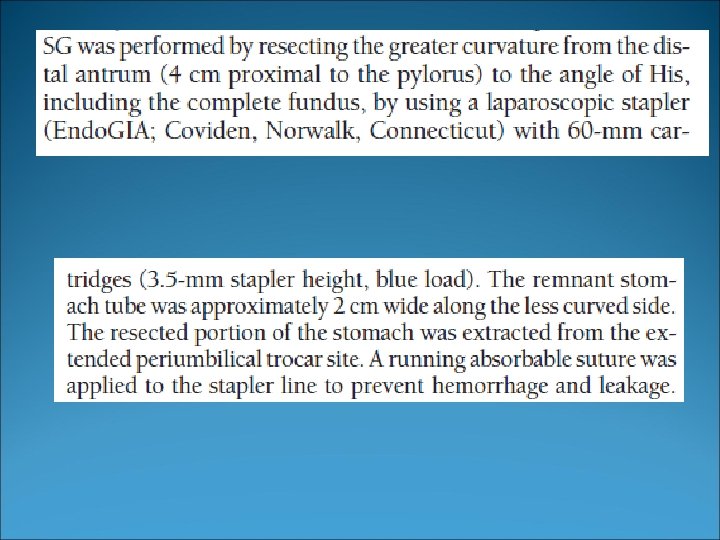
Laparoscopic sleeve gastrectomy: Technique. 40 Fr.

 P<0. 01 Plasma")
Lap Band versus Gastric Sleeve in BMI < 60 (mean 45) P<0. 01 Plasma Ghrelin levels fmol/ml Langer et al. : Obesity Surgery 2005; 15(7): 1024 -29

Small Bowel Transit Time -29% -28% Shah, Todkar et al. SOARD June 2009

Other Hormones Karamanakos Elevated PYY 3 -36 (Sleeve and Gastric bypass n. s. , Ghrelin reduction stronger after Sleeve. P<0. 0001). Ann Surg. 2008 Mar; 247(3): 401 -7 Ferreri (Tarragona) Elevated GLP-1

Short-term effects of sleeve gastrectomy on type 2 diabetes mellitus in severely obese subjects. Obes Surg. 2008 Sep; 18(9): 1077 -82 *At 12 months 85% resolution with BOTH operations

Effectiveness of laparoscopic sleeve gastrectomy on glycemic control in obese Indians with type 2 diabetes mellitus. 53 patients (24 men and 29 women), age 46. 5, BMI 45. 2 hemoglobin A 1 c 8. 4% Surg Obes Relat Dis. 2009 Jul 10. [Epub ahead of print]
 after sleeve gastrectomy vs Months")
% use of medication (oral) after sleeve gastrectomy vs Months

Laparoscopic sleeve gastrectomy for diabetes treatment in nonmorbidly obese patients: Efficacy and change of insulin secretion. Oral glucose loads in 20 severe diabetic patients (body mass index [BMI] >25 and <35, Hb. A 1 C >7. 5%) before and at 1, 4, 12, 26, and 52 weeks after sleeve gastrectomy. Remission of type 2 diabetes was defined as fasting glucose level <126 mg/d. L and Hb. A 1 C <6. 5% without any glycemic therapy. Lee WJ, Ser KH, Chong K, Lee YC, Chen SC, Tsou JJ, Chen JC, Chen CM. Department of Surgery, Min-Sheng General Hospital, Taoyuan City, Taiwan.

Mean BMI vs Weeks 69% EWL

Mean Hb. A 1 c vs Weeks
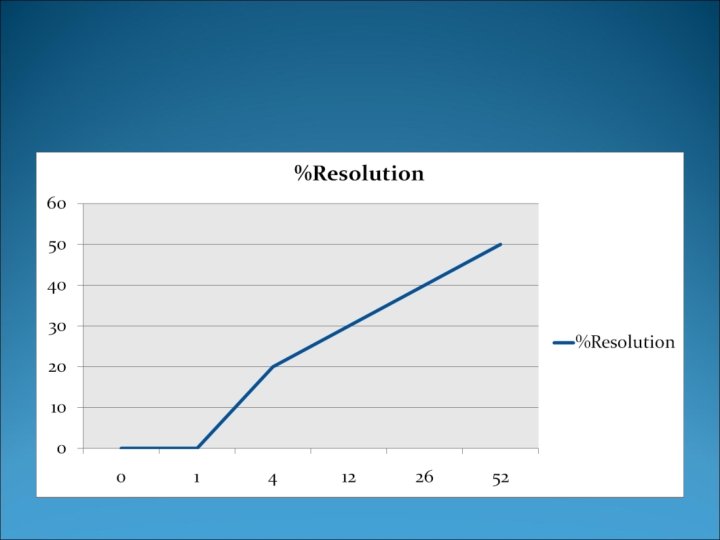

C-peptide levels and % Diabetes Resolution
: 707 -13. Epub 2010 Aug 6. Sleeve")
Surg Obes Relat Dis. 2010 Nov-Dec; 6(6): 707 -13. Epub 2010 Aug 6. Sleeve gastrectomy and type 2 diabetes mellitus: a systematic review. Gill RS, Birch DW, Shi X, Sharma AM, Karmali S. 27 studies, 673 patients The baseline mean BMI 47. 4 kg/m(2) The mean percentage of excess weight loss was 47. 3% (range 6. 3 -74. 6%), with a mean follow-up of 13. 1 months (range 3 -36). DM had resolved in 66. 2% of the patients, improved in 26. 9%, and remained stable in 13. 1%. The mean decrease in blood glucose and hemoglobin A 1 c after sleeve gastrectomy was -88. 2 mg/d. L and 1. 7%, respectively.
: 143 -8. Gastric Bypass vs Sleeve Gastrectomy for Type")
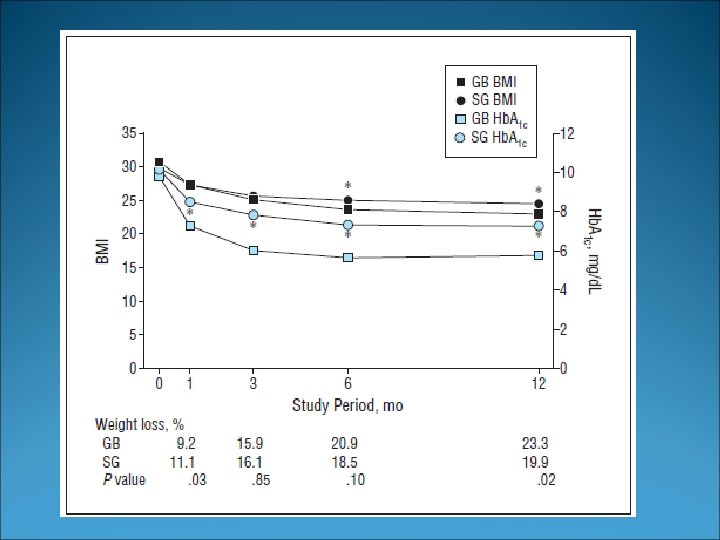
Arch Surg. 2011 Feb; 146(2): 143 -8. Gastric Bypass vs Sleeve Gastrectomy for Type 2 Diabetes Mellitus: A Randomized Controlled Trial. Lee WJ, Chong K, Ser KH, Lee YC, Chen SC, Chen JC, Tsai MH, Chuang LM. 60 patients enrolled, and 12 -month follow-up. Remission of T 2 DM was achieved by 28 (93%) in the gastric bypass group and 14 (47%) in the sleeve gastrectomy group (P =. 02). No equipoise, more weight loss from gastric bypass, makes it suspicious that the sleeve group did not have a proper sleeve? ? ? It makes the point that you CAN achieve resolution. . without duodenal exclusion
: 401 -7. Randomized study: Sleeve vs Gastric Bypass Ann")
Ann Surg. 2008 Mar; 247(3): 401 -7. Randomized study: Sleeve vs Gastric Bypass Ann Surg. 2008 Mar; 247(3): 401 -7
![Obes Surg. 2011 Aug 5. [Epub ahead of print] Randomized Clinical Trial of Laparoscopic](http://slidetodoc.com/presentation_image_h/1b08d5a4c9f10e8a7054c37465613147/image-59.jpg "Obes Surg. 2011 Aug 5. [Epub ahead of print] Randomized Clinical Trial of Laparoscopic")
Obes Surg. 2011 Aug 5. [Epub ahead of print] Randomized Clinical Trial of Laparoscopic Roux-en-Y Gastric Bypass Versus Laparoscopic Sleeve Gastrectomy for the Management of Patients with BMI < 50 kg/m(2). Kehagias I, Karamanakos SN, Argentou M, Kalfarentzos F There was no death in either group and there was no significant difference in early and late morbidity (10% in each group). Weight loss was significantly better after LSG in the first years of the study and at 3 years %EWL reached 62% after LRYGB and 68% after LSG (p = 0. 13). There was no significant difference in the overall improvement of comorbidities. Vitamin B(12) deficiency which was more common after LRYGB (P = 0. 05).

5 years results of randomized study No statistical difference in %EWL between gastric bypass and sleeve gastrectomy

Physiol Behav. 2011 Jun 12. Similar effects of roux-en-Y gastric bypass and vertical sleeve gastrectomy on glucose regulation in rats. Chambers AP, Stefater MA, Wilson-Perez HE, Jessen L, Sisley S, Ryan KK, Gaitonde S, Sorrell JE, Toure M, Berger J, D'Alessio DA, Sandoval DA, Seeley RJ, Woods SC. Control group (Sham) They ate less food and lost more weight, and they both had improved glucose parameters. The most intriguing aspect of the findings is that the two surgical procedures had such similar effects in spite of quite different rearrangements of the gastrointestinal system.
: 738 -43. Impact of laparoscopic sleeve gastrectomy and laparoscopic")
Obes Surg. 2011 Jun; 21(6): 738 -43. Impact of laparoscopic sleeve gastrectomy and laparoscopic gastric bypass on Hb. A 1 c blood level and pharmacological treatment of type 2 diabetes mellitus in severe or morbidly obese patients. Results of a multicenter prospective study at 1 year. Nocca D, Guillaume F, Noel P, Picot MC, Aggarwal R, El Kamel M, Schaub R, de Seguin de Hons C, Renard E, Fabre JM. The average (BMI) in the LGBP group was 47. 9 and 50. 6 in the LSG group. At 1 year after surgery, the average Hb. A 1 c lost was 2, 537 in the GBP group and 2, 175 in the SG group. T 2 DM had resolved (withdrawal of pharmacological treatment) in 60% of the LGBP group and 75. 8% of the LSG group.
: 506 -9. Epub 2011 Jan 28. Is")
Surg Obes Relat Dis. 2011 Jul-Aug; 7(4): 506 -9. Epub 2011 Jan 28. Is sleeve gastrectomy as effective as gastric bypass for remission of type 2 diabetes in morbidly obese patients? de Gordejuela AG, Pujol Gebelli J, García NV, Alsina EF, Medayo LS, Masdevall Noguera C. A total of 90 patients (60 RYGB and 30 SG). The body mass index was 46 kg/m(2) for the RYGB group and 57 kg/m(2) for the SG group. The fasting glycemia was 10. 6 mmol/L and 8. 1 mmol/L and the glycated hemoglobin was 8. 1% and 7. 3% in the RYGB and SG groups, respectively. No significant differences were seen in the amount of weight loss after 2 years between the 2 techniques.

T 2 DM resolution

Bariatric Surgery versus Intensive Medical Therapy in Obese Patients with Diabetes Philip R. Schauer, M. D. , et al. N Engl J Med 2012; 366: 1567 -1576 April 26, 2012 hemoglobin level of 7. 5± 1. 8% in the medical-therapy group, 6. 4± 0. 9% in the gastricbypass group (P<0. 001), and 6. 6± 1. 0% in the sleeve-gastrectomy group (P=0. 003). Weight loss was greater in the gastric-bypass group and sleeve-gastrectomy group (− 29. 4± 9. 0 kg and − 25. 1± 8. 5 kg, respectively) than in the medical-therapy group (− 5. 4± 8. 0 kg) (P<0. 001 for both comparisons). The primary end point was 12% in the medical-therapy group versus 42% in the gastric-bypass group (P=0. 002) and 37% in the sleeve-gastrectomy group (P=0. 008).
 randomized to best medical treatment vs surgical therapy (Gastric")
60 patients (BMI < 35) randomized to best medical treatment vs surgical therapy (Gastric bypass or BPD) 5 years duration of diabetes, Hb. A 1 c >7% End point remission at 2 years Remission at 2 years was 0% in medical group, 75% in gastric bypass and 95% in BPD

SGIT: Sleeve Gastrectomy with Ileal Transposition: The next generation of Weight Loss Surgery?

Hypothesis Accelerated stimulation of ileum by transposing a segment into the proximal small bowel may signal earlier release of PYY 3 -36 & GLP-1 Combined with gastric Sleeve restriction, decreased ghrelin levels this combination may produce a more optimal (less nutritionally deficient) option for bariatric surgery

Ileal Transposition AJP Endocrinol Metab, 228; p E 449, 2005

Body weights after IT

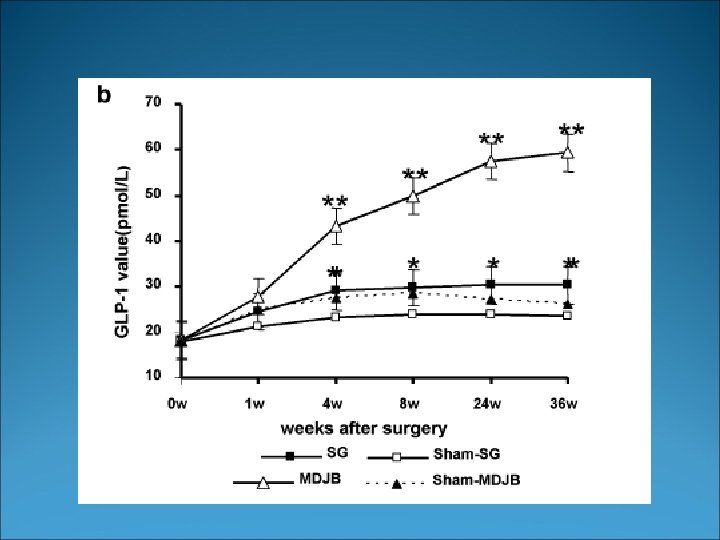
GLP-1 levels after IT

PYY levels after IT

Best of both worlds Decrease in Ghrelin Increase in PYY-3 -36 and GLP-1 Double effect on Neuropeptide Y SGIT NO micronutrients deficiencies

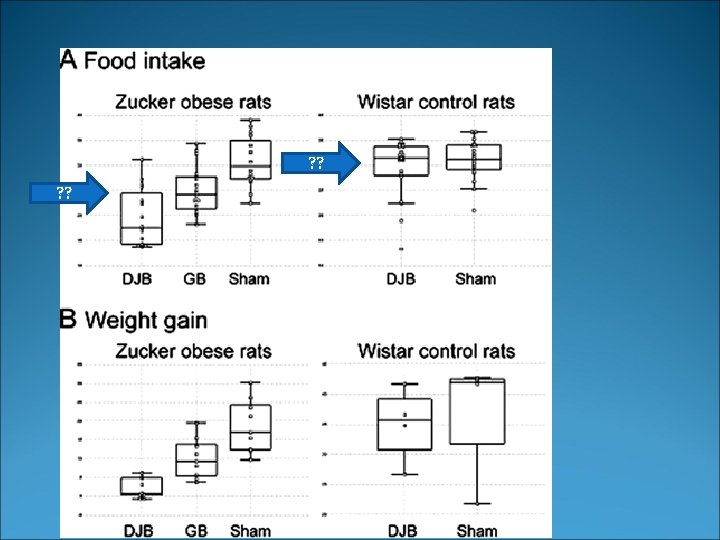
Weight progression of Pigs Weeks T 4 Sham Control: Ileal reanastomosis T 1 Ileal transposition Alone T 2 SGIT: Sleeve Gastrectomy with ileal Transposition T 3 RYGP: Roux en Y Gastric Bypass

Mineral absorption % P<0. 05

Weight change • 131. 8 ± 2. 6% • 117. 8 ± 8. 6% • 100. 4 ± 6. 7% • 88. 4 ± 12. 8% • p<0. 001 compares to SHAM • ° p<0. 001 compares to IT

Fasting glucose • 288. 5 ± 76. 3 • 218. 5 ± 52. 7 • 119 ± 36, 8 • 134. 7 ± 38. 7 • * p<0. 001 compares to SHAM International Surgical Week 2007, Montreal August 29, 2007
 Boza et al, DDW 2007")
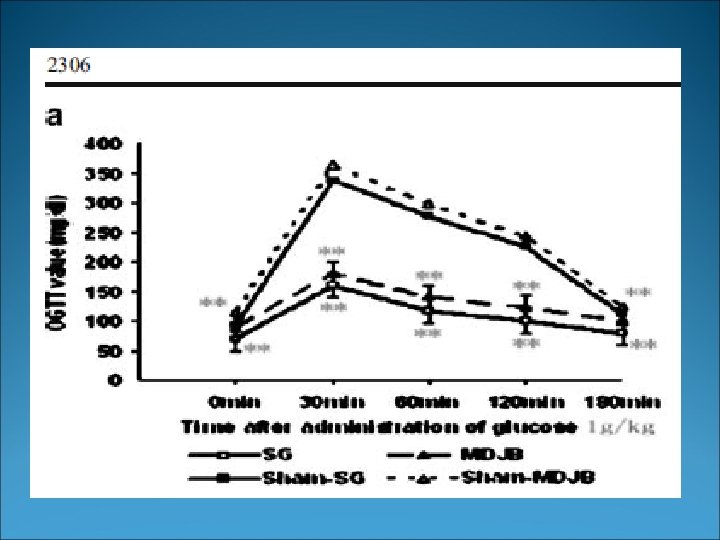
Glucose tolerance test (Zucker Diabetic) Boza et al, DDW 2007

Insulin tolerance test Procedur e SHAM RYGB IT 0 minutes 444 ± 19 209 ± 9. 9 125. 3± p value 30 minutes p value 60 minutes p value NS* <0. 001* 417 ± 80 213. 1 ± 61. 6 <0. 001* 105. 7 ± 24. 2 <0. 001* 373. 3± 48. 1 189. 3± 33. 2 <0. 001* 146± 54 <0. 001*
 : La")
La transposition iléale avec ou sans gastrectomie par laparoscopie chez l'homme (TIG) : La troisième génération de chirurgie bariatrique GAGNER M. L'échec sévère d'un switch duodénal chez un sujet de 155 kg avec un IMC de 50 kg/m 2 aboutissant à un amaigrissement incontrôlable (66 kg, IMC 23, 6 kg/m 2), avec carence malabsorptive, n'a pu être corrigé que par l'interposition duodénale d'un segment d'iléon terminal. Cette efficacité thérapeutique fait proposer par l'auteur la technique de la transposition duodénale de l'iléon, associée à une gastrectomie en manchette (sleeve). Après les opérations "restrictives" et "malabsorptives", il s'agit de la naissance de la troisième génération de procédures bariatriques à visée hormonale; cette action est basée essentiellement sur la stimulation hormonale précoce des hormones anorexigènes PYY 3 -36, GLP et OXM au niveau de l'iléon terminal transposé, et sur la diminution de l'hormone anti-anoréxigène Ghreline par la gastrectomie, avec donc peu de "restriction" et pas de "malabsorption". Cette voie thérapeutique nouvelle est appelée à un grand développement mais ses résultats doivent être confirmés par des recherches expérimentales et par des études complémentaires chez l'animal et chez l'obèse. Revue Le Journal de coelio-chirurgie 2005, no 54, pp. 4 -9

Laparoscopic SGIT: Sleeve Gastrectomy with Ileal Transposition in Humans Different types Of Transposition Possible ! a) Inter Esophago-Gastric b) Inter Gastro-Gastric c) Inter Duodenal d) Inter Jejunal Gagner M: J Coelio. Chirg 2005.
 De Paula, Surg Endsoc 2007")
Ileal Interposition in BMI less than 35 (n=39) De Paula, Surg Endsoc 2007

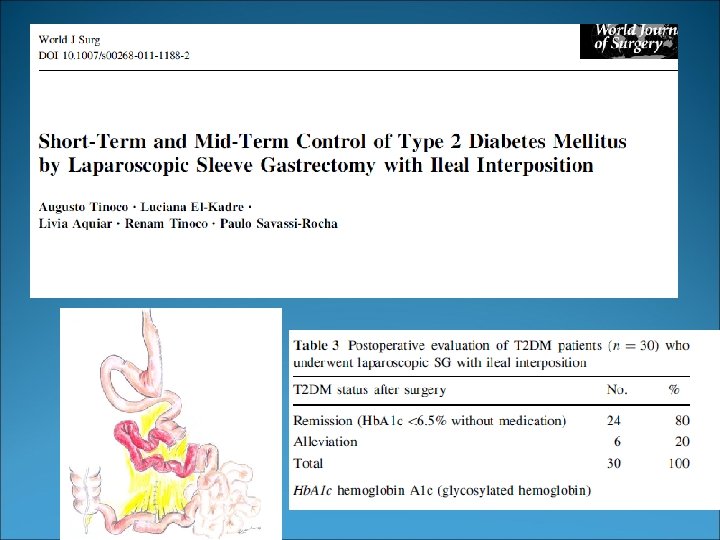
Diabetes Control SGIT provided a weight control comparable to standard gastric bypass without malabsorption SGIT induced high levels of GLP 1 after the meal test The diverted form is very close to a duodenal switch 2010

Ileal Interposition – Sleeve Gastrectomy Ileal Interposition – Diverted Sleeve Gastrectomy 1

Ileal Interposition – Sleeve Gastrectomy Ileal Interposition – Diverted Sleeve Gastrectomy 1

Ileal Interposition – Sleeve Gastrectomy Ileal Interposition – Diverted Sleeve Gastrectomy 2

Ileal Interposition – Sleeve Gastrectomy Ileal Interposition – Diverted Sleeve Gastrectomy 2

Ileal Interposition – Sleeve Gastrectomy Ileal Interposition – Diverted Sleeve Gastrectomy 3

Ileal Interposition – Sleeve Gastrectomy Ileal Interposition – Diverted Sleeve Gastrectomy 3

Ileal Interposition – Sleeve Gastrectomy Ileal Interposition – Diverted Sleeve Gastrectomy 4 4
 Four Internal hernias Diverted Sleeve gastrectomy")
Issues Reproducibility Four anastomosis and a stump (leaks) Four Internal hernias Diverted Sleeve gastrectomy plus ileal interposition. . . Duodenal switch More human studies need to be done, especially compared to a short DS which is easier

A Duodenal Switch !!! Duodeno-ileostomy

A Duodenal Switch !!! Sleeve Gastrectomy
")
A Duodenal Switch !!! Biliopancreatic limb(excluded duodenum+prox jejunum)

A Duodenal Switch !!! Common channel

Efficacy for Improvement in Diabetes. Related Outcomes by Surgical Procedure % Buchwald et al. JAMA, 292(14), 2004
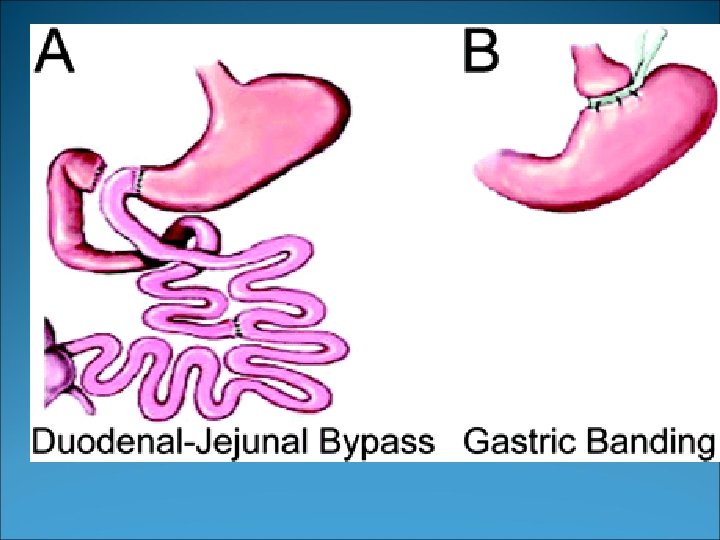
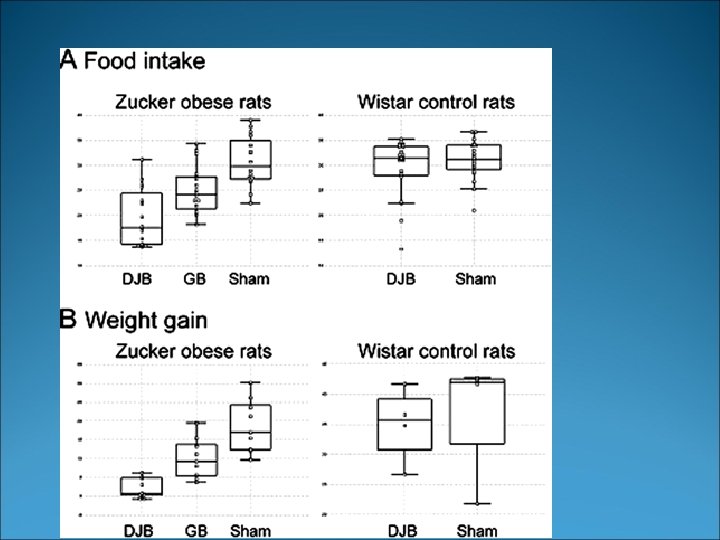
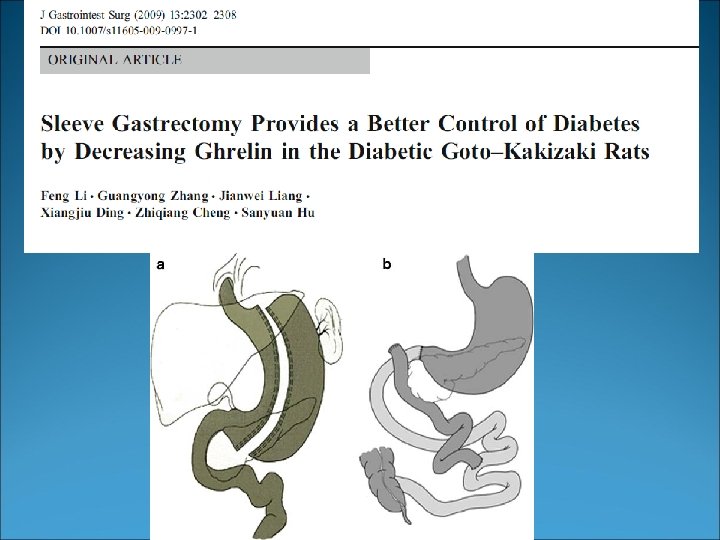
 for Type-2 Diabetes mellitus Goto-Kakizaki rats (spontaneous Type-2 DM) DJB vs")
Duodeno-Jejunal Bypass (DJB) for Type-2 Diabetes mellitus Goto-Kakizaki rats (spontaneous Type-2 DM) DJB vs Sham Plasma Glu 159 mg/d. L to 96. 3 at 3 weeks. 40% reduction Proximal gut origin? Rubino F et al. Ann Surg 2004; 239(1): 1 -11

Pause Should the rat study been confirmed by other groups? Should a larger mammals study been done before doing this in Humans? Should an ulcerogenic operation been done (Mann. Williamson)?
 for Type-2 Diabetes mellitus Duodeno-jejunal bypass for the treatment of type-2")
Duodeno-Jejunal Bypass (DJB) for Type-2 Diabetes mellitus Duodeno-jejunal bypass for the treatment of type-2 diabetes in patients with Body Mass Index of 22 -34 kg/m 2: a report of 2 cases. Cohen R et al. SOARD 2007; 3(2): 195 -7
 Hosp. Stay :")
Prospective study 35 patients Mean OR time 46 minutes (33 -78) Hosp. Stay : 30 hours 1 mortality Complications 14. 2% (obstruction, pancreatitis, bleeding) 37% prolonged nausea , and half needed readmission Cohen Ret al: Hospital Sao Camilo, Sao Paulo, Brazil

Minimal improvement in Glycemic Homeostasis-12 months after DJBypass 7 subjects, BMI 22 -33 Glu 209 to 154 mg/d. L Cho and Trig inc. ? Clinical improv. Ferzli GS, et al: World J Surg 2009; 33: 972 -979

Diabetic medication requirements, preop and 1 year Ferzli GS, et al: World J Surg 2009; 33: 972 -979
: 409 -22.")
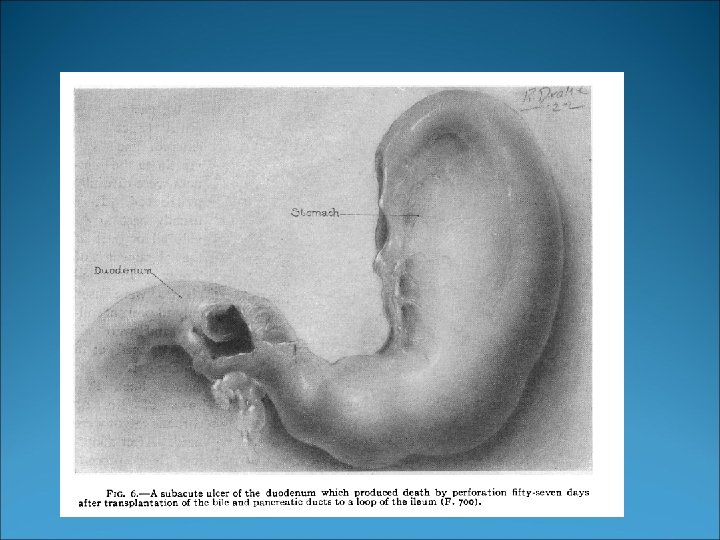
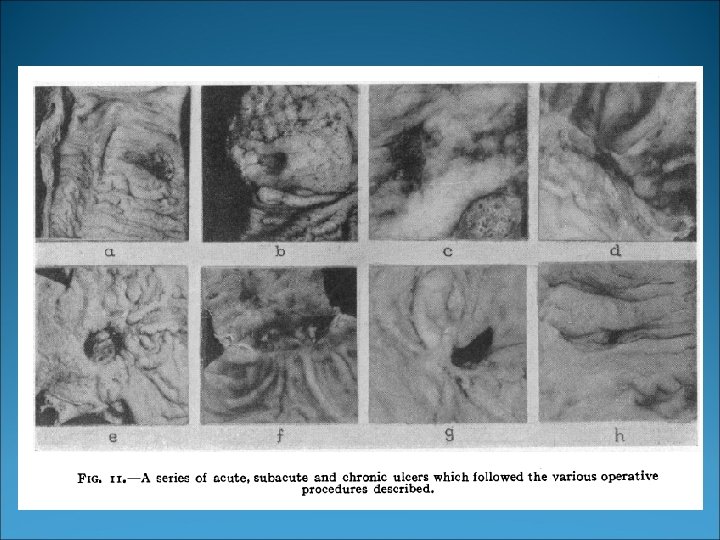
Ann Surg. 1923 Apr; 77(4): 409 -22.
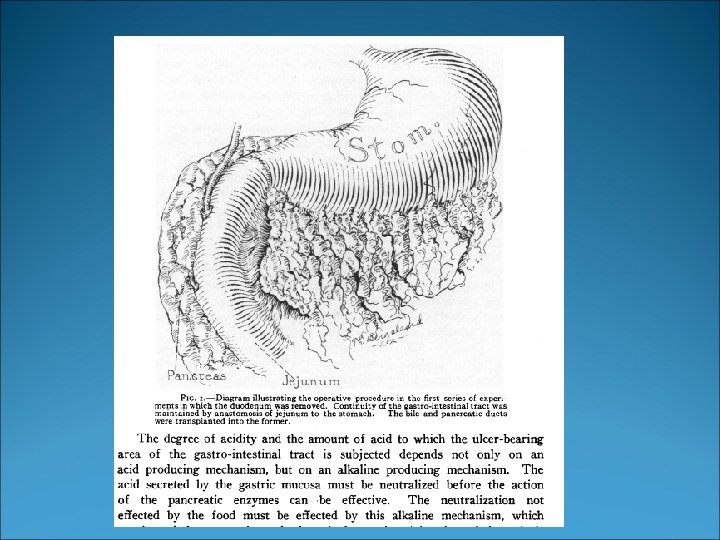

Laparoscopic sleeve gastrectomy and duodeno-jejunal bypass. A new surgical procedure for weight control in a porcine model. Gianmattia del Genio 1, M. D, Ph. D, Michel Gagner 2, M. D. , F. A. C. S. , F. R. C. S. C. , Federico Cuenca-Abente 3, M. D. , Laurent Biertho 3, M. D. , Maurizio Grillo 1, M. D. , Ph. D, David Nocca, M. D 3. . Obes Surg. 2008 Oct; 18(10): 1263 -7. Epub 2008 Jun 18.

Preliminary results of Human experience with Sleeve+DJB 21 patients over 19 months period 108 kg , or BMI 41 kg/m 2 Weight loss of 37 kg or % EWL 96 One leak Resolution of DM was 96% Resolution/improvement of hypertension was 86% Kasama K et al. : Obes surg 2009; 19: 1341 -45
![Obes Surg. 2011 Aug 27. [Epub ahead of print] Is Laparoscopic Duodenojejunal Bypass with](http://slidetodoc.com/presentation_image_h/1b08d5a4c9f10e8a7054c37465613147/image-115.jpg "Obes Surg. 2011 Aug 27. [Epub ahead of print] Is Laparoscopic Duodenojejunal Bypass with")
Obes Surg. 2011 Aug 27. [Epub ahead of print] Is Laparoscopic Duodenojejunal Bypass with Sleeve an Effective Alternative to Roux En Y Gastric Bypass in Morbidly Obese Patients: Preliminary Results of a Randomized Trial. Praveen Raj P, Kumaravel R, Chandramaliteeswaran C, Rajpandian S, Palanivelu C. 57 patients Randomized. The mean BMI and % EWL at 3, 6, and 12 months between the groups were not statistically significant. The operating times were higher in the DJB group. The rate of resolution of diabetes, hypertension, and dyslipidemias were also similar with no statistical significance. There was 100% resolution of dyslipidemias in both groups.

Glp 1 Ileal versus Duodenal Bypass

Getting closer to the best surgery for Type-2 Diabetes SGIT very close to Short Duodenal switch, very close to Sleeve with Duodeno-jejunal Bypass !!!
 had type-2 DM")
Type-2 DM will recur after GB if weight regain? 153/172 (89%) had type-2 DM resolution after Gastric Bypass 66/172 (43%) had recurrence They had a drop of EWL from 66% to 49%. Males have a more durable pattern. *IN SPITE OF DUODENAL EXCLUSION Chikunguwo et al. SOARD 2009; 5: S 1
")
Sleeve Gastrectomy: Beyond 5 years (5 -9 years studies)

Can Laparoscopic Sleeve Gastrectomy replace Gastric Bypass for type 2 DM? Easier procedure to perform Less mortality and morbidity Similar weight loss and resolution of co-morbidity (5 years). Minimal nutritional impact Minimal long-term complications (ulcer, bowel obstruction) No remnant to follow (access to bile duct, gastric ca? ) Easier to revise or convert for weight regain Can be used in staged approaches

Surgery has the potential to cause a resolution of type-2 diabetes in 320 million patients in 2015… We have a manpower problem, as it takes 10 years to create a surgeon, and another 10 years for great experience and expertise! A simpler procedure is needed!

th 4 Sleeve Consensus meeting, December 6 -7 -8 th, 2012 ICSSG. COM

- Slides: 129