Supporting Students with Mental Health Conditions in Job

Supporting Students with Mental Health Conditions in Job Corps Depression and Bipolar Disorders
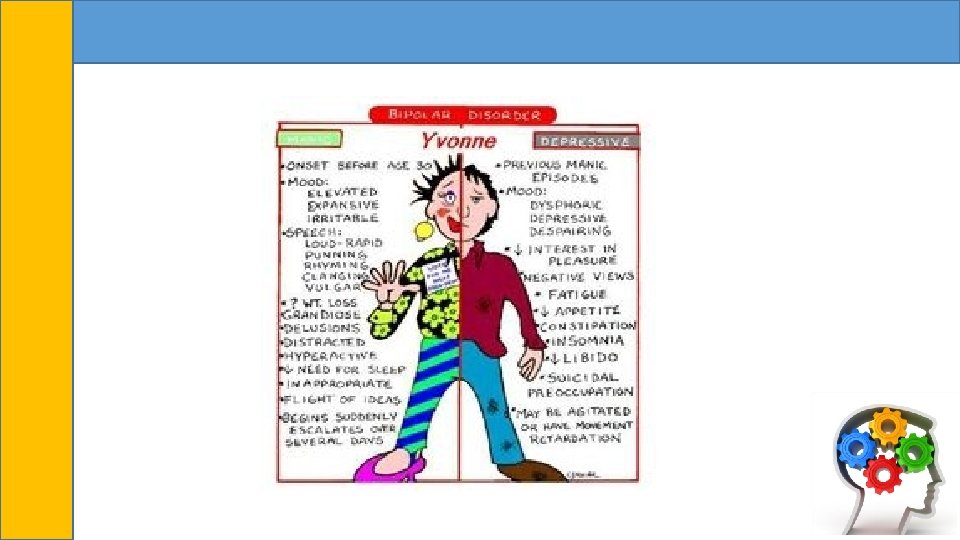
 Mental Health")
Presenter Information • Vicki Boyd, Ph. D • Region 6 (San Francisco) Mental Health Specialist 2

Learning Objectives • After this presentation, participants will be able to: • articulate applicable changes to titles and diagnostic criteria for depression and bipoloar disorders based on DSM-5. • recognize how clinical presentations for depression and bipolar disorders may vary for adolescents and young adults. • identify at least one evidence-based intervention for depression and bipolar disorders 3
-5 Overview Depressive and Bipolar Disorders 4")
Diagnostic and Statistical Manual (DSM)-5 Overview Depressive and Bipolar Disorders 4

Depressive Disorder in DSM-5 • Disruptive Mood Dysregulation Disorder • Major Depressive Disorder • Persistent Depressive Disorder • Premenstrual Dysphoric Disorder • Substance/Medication-Induced Depressive Disorder • Depressive Disorder due to Another Medical Condition • Other specified depressive disorder • Unspecified depressive disorder 5

DSM-5 Changes • To address concerns about potential overdiagnosis and overtreatment of bipolar disorder in children, a new diagnosis, disruptive mood dysregulation disorder, is included for children up to age 18 years who exhibit persistent irritability and frequent episodes of extreme behavioral dyscontrol. • Premenstrual dysphoric disorder has been moved from DSM-IV Appendix B, “Criteria Sets and Axes Provided for Further Study, ” to the main body of DSM-5. • Conceptualizes chronic forms of depression in a somewhat modified way. 6

Major Depressive Disorder Changes • The core criterion symptoms applied to the diagnosis of major depressive episodes has not changed from DSM-IV • The coexistence within a major depressive episode of at least three manic symptoms is now acknowledged by the specifier “with mixed features. ” 7

Bereavement Exclusion • In DSM-IV, there was an exclusion criterion for a major depressive episode that was applied to depressive symptoms lasting less than 2 months following the death of a loved one (i. e. , the bereavement exclusion). • Omitted for several reasons: • Bereavement commonly lasts 1 -2 years • Bereavement is recognized as a severe psychosocial stressor that can precipitate a major depressive episode in a vulnerable individual, generally beginning soon after the loss • Bereavement-related major depression is most likely to occur in individuals with past personal and family histories of major depressive episodes • The depressive symptoms associated with bereavement-related depression respond to the same psychosocial and medication treatments as non–bereavement-related depression 8

Specifiers • Suicide Risk: DSM V provides guidance on assessment of suicidal thinking, plans, and the presence of other risk factors in order to make a determination of the prominence of suicide prevention in treatment planning for a given individual. • Mixed Symptoms: Added across both the bipolar and the depressive disorders, allowing for the possibility of manic features in individuals with a diagnosis of unipolar depression • With Anxious Distress: Gives the clinician an opportunity to rate the severity of anxious distress in all individuals with bipolar or depressive disorders 9

Differentiating Between Depressive Disorders • Disruptive Mood Dysregulation Disorder: chronic, severe persistent irritability • Major Depressive Disorder: Symptoms including depressed mood, diminished interest or pleasure, etc. present nearly every day during a 2 -week period • Persistent Depressive Disorder: Depressed mood that last for at least 2 years in adults or 1 year in children/adolescents • Premenstrual Dysphoric Disorder: Irritability, dysphoria, and anxiety symptoms that occur repeatedly during the premenstrual phase of the cycle • Substance/Medication-Induced Depressive Disorder: Symptoms of major depressive disorder associated with ingestion of a substance • Depressive Disorder due to Another Medical Condition: Period of depressed mood that predominates in the clinical picture; direct pathophysiological consequence of another medical condition • Other specified depressive disorder: Symptoms are characteristic of a depressive disorder but do not fully meet criteria • Unspecified depressive disorder: Same as above; Used when clinician chooses not to specify reason criteria is not met 10

Bipolar and Related Disorders in DSM-5 • Bipolar I Disorder • Bipolar II Disorder • Cyclothymic Disorder • Substance/Medication-Induced Bipolar and Related Disorders • Bipolar and Related Disorder Due to Another Medical Condition • Other Specified Bipolar and Related Disorder • Unspecified Bipolar and Related Disorders 11

DSM-5 Changes • Criterion A for manic and hypomanic episodes now includes an emphasis on changes in activity and energy a well as mood. • Importance of behavioral observations. • It is no longer necessary to use DSM-IV diagnosis of mixed episode but rather use the specifier “with mixed features” from DSM-5 to more accurately support the diagnosis. 12

Other Specified Bipolar and Related Disorders • DSM-5 allows the specification of a specified bipolar condition for individuals with a documented past history of major depressive disorder if hypomania is present. • A secondition constituting an other specified bipolar disorder is that too few symptoms of hypomania are present but do last for more than four days. 13

Anxious Distress Specifier • In the chapter on bipolar and related disorders and the chapter on depressive disorders, a specifier for anxious distress is delineated. • This specifier is intended to identify patients with anxiety symptoms that are not part of the bipolar diagnostic criteria. 14

Differentiating Between Bipolar Disorders • Bipolar I Disorder: Criteria must be met for at least one manic episode and depressive episode • Bipolar II Disorder: One or more major depressive episodes and at least one episode of hypomania, with possible periods of level mood between episodes. • Cyclothymic Disorder: Chronic, fluctuating mood disturbance involving numerous periods of hypomanic symptoms and periods of depressive symptoms • Substance/Medication-Induced Bipolar and Related Disorders: Symptoms of bipolar associated with substance intoxication or withdrawal • Bipolar and Related Disorder Due to Another Medical Condition: Symptoms of bipolar associated with another medical condition • Other Specified Bipolar and Related Disorder: Symptoms of bipolar do not meet full criteria for any other disorder • Unspecified Bipolar and Related Disorders: Same as above; Used when clinician chooses not to specify reason criteria is not met 15

Disruptive Mood Dysregulation • Because of the newness of this diagnostic category, there are few studies available for the Job Corps age group. It is wise to consider this for JC students in spite of its “newness”. • Multiple studies exist on children ranging in age from 8 to 16 with the cautionary note to avoid diagnosing children with bipolar disorder. • This diagnosis is not given to adolescents over 18, therefore the following example is reflective of minor students in Job Corps.

Scenario for Disruptive Mood Dysregulation Disorder • Seventeen-year-old female is referred from academics because of unruliness in the classroom, disrespectful language towards to staff, verbal rants, social difficulties with peers, no one wants to room with her, unstable dating relationships and generalized lack of responsibility for her own actions. In order to pursue the above diagnosis, the following must be ruled out: • a. ADHD • b. Substance abuse • c. Other medical conditions • IACAPAP e-textbook of Child and Adolescent Mental Health Geneva: International Association for Child and Adolescent Psychiatry and Allied Professions, 2012.

Major Depressive Disorder • Definition: A period of two weeks or longer during which there is either depressed mood or loss of interest or pleasure, and at least four other symptoms that reflect a change in functioning, such as problems with sleep, eating, energy, concentration, and self-image. • While there are not precise statistics covering Job Corps 16 to 24 age group, NIMH (www. nimh. gov) suggests that major depressive disorders are common among these groups. (roughly 12 to 18 %)

Major Depressive Disorder Statistics • An estimated 15 to 18% of Job Corps students seeking mental health assistance will present with depression symptoms based on the prevalence in the general population. • Because Job Corps is a work-training program, it is of interest to note that an estimated cost of job productivity and related health care issues due to depression is approximately $80 trillion. • 50% of the general population with major depression do not seek treatment. Since JC is a residential program, the likelihood of early detection and diagnosis is probably much lower for JC students. • Suicide death statistics vary depending upon the age group and occupation group (e. g. veterans). The national rate in 2014 for suicide death in age group 15 -24 was 11. 5 per 100, 000 (overall rate in general population was 13. 4 per 100, 000). Most important, the Job Corps rate was 2. 0 per 100, 000.

Treatment Considerations for Depression • Most treatments will include collaboration with the utilization of medical and medication interventions. (Separate slide) • Psychosocial/Non-Pharmacological interventions include psychoeducation, cognitive behavior therapies and group supports. • Center-wide educational presentations are excellent venues for staff and students to participate in early detection and peer support. • Early detection of psychosocial stressors through the use of the SIF can aid staff in assessing stressors and risks. • Supportive, mood elevating activities can be achieved by collaborating with Job Corps own recreation department, its music programs, and HEALs programs.

Additional Treatment Considerations • Job Corps provides a variety of group programs through its Counseling department. These groups are frequently provided in collaboration with a center mental health consultant. • Utilization of programs outside of the Job Corps center are typically determined by the availability in each geographical area. For example, urban centers may have access to support programs that are free or of low cost. Rural centers may rely on their county mental health programs in their areas. • Utilization of Self-Help programs (Help. Guide. org) • Utilization of Job Corps’ own Youth 2 Youth Program (www. Job. Corps. Y 2 Y. com)
 • Most, if not all, major depressive disorders will require some")
Pharmacological Treatments (Antidepressants) • Most, if not all, major depressive disorders will require some form of medication support in order to achieve success in treatment. • It is important to assist students in obtaining an adequate medication evaluation and for you to maintain support especially through the initial portion of medication treatment. Remember, the PRH requires that the center MD, nursing staff, and CMHC must collaborate on monitoring students on psychotropic medications. (Some centers use a group format to monitor students). • As a non-prescriber (CHMC), it is strongly encouraged to establish a relationship with the student’s medication provider so that you may coordinate treatment for optimal results. • Pharmacological treatments will be covered in other webinars.

Major Depression Scenario • A twenty-year-old female refers herself to the CMHC because she is not eating and sleeping well, has recognized a definite change (for the worse) in her overall mood and lack of energy. She reports that the feelings are only getting worse and that she has felt this way for nearly a month. Her thoughts are dark and of wishing she were dead. She has withdrawn from her family and friends and can barely function at her trade (which she loves). Her increased thoughts of suicide initiated her self-referral. (Her dorm mates were also worried)

Working with a Student with Depression • Take a thorough history to rule out: • • Extenuating circumstances such as a recent loss ADHD Dampened mood because of recent social debacle Substance abuse and its consequences (consult with TEAP) • Consult with center MD regarding medication trials. • Establish a collaborative treatment plan for the student.

Bipolar I and Bipolar II • Bipolar I: The Individual has experienced one or more episodes of mania. Most will have depression as well but not all. Episode must last at least 7 days and present most of each day, nearly every day (or can be any duration if hospitalization is necessary). • Bipolar II: A subset of bipolar I during which individuals experience depressive episodes shifting back and forth with hypomanic episodes but never a full manic episode. (more likely to be observed in the JC population than bipolar I).

Teens and Young Adults with Bipolar Disorder • Less than 5% of children and young adults experience bipolar disorder but its symptoms include an ongoing combination of highs and lows that occur more rapidly than in their adult counterparts. • Manic symptoms include severe changes in mood like silliness, irritability, unrealistic highs in self-esteem, talks too fast, too much and uninterruptible, distractible, and can engage in high risk behaviors such as jumping off a roof believing no harm can come. • Depressive symptoms include persistent sadness, loss of enjoyment, low energy, poor concentration, and changes in sleeping and eating habits.

Treatment of Bipolar Disorder • The following treatment regimens are as follows: • Medications such as mood stabilizers, antipsychotics and antidepressants • Psychotherapies such as cognitive behavioral therapy and family-focused treatment • Electroconvulsive therapy (ECT) • Self-management strategies and education

Causes of Bipolar Disorder • Scientists have not discovered a single cause of bipolar disorder. • Contributors might be: • Genetics but nothing absolute. • Stress may be a trigger but not necessarily a cause. • Adverse childhood experiences are being considered more causal to the overall diagnostic picture. Recent study noted that people with the diagnosis of bipolar disorder are 2. 63 times more likely to have suffered emotional, physical, or sexual abuse as children than the general population (http: //www. mdlinx. com/neurology/printpreview. cfm/6901228)

Bipolar Scenario • A 24 -year-old female is referred by her trade instructor as being “all over the map. ” She has been diagnosed with the “question of bipolar disorder” by her provider of 3 years ago. She has pursued no treatment. She reports a poor school and work record, excelling at times and failing and getting fired at others. Social relationships are uneven and at times disastrous. She states that her family is populated with “kooks” and “drunks”. She has tried alcohol and marijuana to help with her moods but with no avail. She insists that Job Corps is her “last chance” and that she is determined to finish her trade.

Working with a Student with Bipolar Disorder • Obtain as thorough a history as possible, including any past mental health treatments. • Collaborate with the center MD to assist in the evaluation. • Invite the student to prepare a “family tree” with behavioral descriptors so that a genetic component may be reviewed. • Design a treatment approach with the center MD that would begin to help student manage her mood changes. Enlist support from her teachers, trade instructors, dorm staff, and career counselor. • Enlist any outside resources that may be available to your center, if any. (NAMI Helpline: 800 -950 -6264)

Cyclothymic Disorder • Definition: Individuals experiencing mood cycling over a two year period, but have not met the diagnostic criteria for Bipolar I, Bipolar II, or Depressive disorder. (please be careful to avoid ascribing “adult” symptoms to adolescents). • Symptoms include a two year period of hypomanic and depressive experiences, no history of diagnoses of manic, hypomanic, or depressive episodes, and are differentiated from medical and substance abuse conditions. They may impair social functioning. • Onset: Its prevalence is less than 1% of the population but does typically occur in adolescence and young adults.

Summary • We have just reviewed an enormous amount of material relating to Major Depressive Disorders and Bipolar Disorders and all of their relatives. • Probably the single most important lesson for Job Corp Health staff, especially the CMHC is to take a careful history and document it with any and all family history that is available to you. • Secondly, and also terribly important is to forge an alliance with the medication prescribers whoever they may be. (For some this will be a psychiatrist, for many, this will be a family practitioner). • A combination of therapies will serve your student best. This will likely include a combination of cognitive behavioral therapy, psychoeducation and medication.
 Diagnostic and Statistical Manual of Mental")
References and Linkages • American Psychiatric Association (2014) Diagnostic and Statistical Manual of Mental Disorders (5 th edition). Washington, DC. • Bressert, S. (2016). Teens and Bipolar disorder. Psych Central. (http: //psychcentral. com/lib/teans-and-bipolar -disorder/) • Cochrane Review (best evidence-based, standardized review available of more than 20 recent studies) Internet Mental Health. • Baldessarini, R. J. , and Vazques, G. Tondo, L. Treatment of Cyclothymic Disorder: Commentary. Psychotherapy Psychosomatic. 80: 131 -135. DOI: 10. 1159/000322234. • Centers for Disease Control and Prevention (an overview of depression). • Cochranelibrary. com for reviews of recent evidence-based studies on bipolar disorder.
. Major Depressive Disorder")
More References and Linkages • National Alliance on Mental Illness (NAMI). Major Depressive Disorder Among Adolescents: https: //www. nimh. nih. gov/health/statistics/prevalence/majordepression-with-severe-impairment-among-adolescents. shtml • Substance Abuse and Mental Health Services Administration: http: //www. samhsa. gov • World Health Organization Depression Treatment Guidelines: http: //www. paho. org/mhgap/en/depression. html

Self Help Resources Y 2 Y Job Corps. www. Job. Corps. Y 2 Y. com Depression and Bipolar Support Alliance. www. dbsalliance. org Help. Guide. www. Help. Guide. org National Alliance on Mental Illness (NAMI help line: 800 -950 -6264) Keeping Your Balance. http: //www. cci. health. wa. gov. au/resources/infopax. cfm? Info_ID=38 • Self Monitoring for Relapse Prevention (patient workbook) (http: //www. cci. health. wa. gov. au/docs/KYB-3 -Self%20 Monitoring. pdf) (PDF) • • •
- Slides: 36