SUPPLEMENTAL OXYGEN A little oxygen never hurt anybody

SUPPLEMENTAL OXYGEN “A little oxygen never hurt anybody, right? ” Kyle Morgan, MD TSPAN State Conference St. Jude Children’s Research Hospital August 25 th, 2018

OUTLINE • Role of oxygen in the body • Free radicals • Beneficial aspects of hyperoxia • Role of anesthesia • Special Considerations • Infants • Middle aged • Elderly • COPD • Alveolar Hypoventilation • Clinical Studies • Recommendations

The best “antioxidant” is…. . …. preventing oxidant formation!!!

BUT LET’S BACK UP… How much oxygen do we need? (and, to review, why do we need it? )

OXYGEN • Final electron acceptor in the electron transport chain in the production of ATP • The key piece in the production of our body’s main energy source! • Goals of respiration: • Get enough O 2 to the mitochondria • Get rid of byproduct of metabolism (CO 2)

OXYGEN • Final electron acceptor in the electron transport chain in the production of ATP • The key piece in the production of our body’s main energy source! • Goals of respiration: • Get enough O 2 to the mitochondria • Get rid of byproduct of metabolism (CO 2)

Get enough O 2 to the mitochondria • We see a low Sa. O 2 and think, “I must increase the Fi. O 2!” • BUT, it’s not just about the saturation… • Delivery of O 2 (DO 2) = Cardiac Output (CO) x Arterial Oxygen Content (Ca. O 2) • CO = HR x SV (or MAP –CVP/SVR) • Ca. CO 2 = (Hb x (sat/100) x 1. 39) x (0. 003 x Pa. O 2) • Oxygen delivery (DO 2) depends on 7 different variables!!! • Hb, Pa. O 2, HR, SV, MAP, CVP, SVR

Leach 2002

SO, THAT’S HOW WE USE IT AND WHY WE NEED IT… But, how much do we need?

HEMOGLOBIN-OXYGEN DISSOCIATION CURVE

HEMOGLOBIN-OXYGEN DISSOCIATION CURVE • DO 2 depends more on Hb saturation rather than Pa. O 2 90% • Due to the 0. 003 multiplier in the oxygen content equation • Therefore, there is little extra benefit in increasing Pa. O 2 above 67 mm. Hg due to the sigmoid shape of the curve • At 67 mm. Hg, about 90% of Hb is saturated 67

But I’m not measuring Pa. O 2, how much O 2 will get me to a Pa. O 2 of 67 mm. Hg? Approximate Pa. O 2 100 150 250 375 450.

HEMOGLOBIN-OXYGEN DISSOCIATION CURVE 90% • At 100% Sa. O 2, the Pa. O 2 can vary 6 fold! (100 mm. Hg to 600 mm. Hg) • Due to flattened shape of the curve • The tone drop from 100 to 97% is disproportionate to its physiologic significance!!! 600 mm. Hg

“BUT I FEEL GOOD WHEN I HEAR THAT NICE HIGH TONE OF 100% ON THE PULSE OX” There’s no harm in that, right?
 Superoxides Peroxides Reactive oxygen metabolites (ROM) _________________")
“Free Radicals” AKA: Reactive oxygen species (ROS) Superoxides Peroxides Reactive oxygen metabolites (ROM) _________________ ___ OXIDANTS
 • 90% of the oxygen in the body is utilized")
REACTIVE OXYGEN SPECIES (ROS) • 90% of the oxygen in the body is utilized in the mitochondria • 80% of that is used for making ATP • 1 -2% of that isn’t used effectively Superoxide and hydrogen peroxide formation
 • Superoxide and hydrogen peroxide react with lipids, proteins, DNA")
REACTIVE OXYGEN SPECIES (ROS) • Superoxide and hydrogen peroxide react with lipids, proteins, DNA and transition metals that are present in the cell • Abnormal levels of ROS amplify toxicity in all cell types • Lung and nervous system cells are especially affected
 • O 2 toxicity occurs when oxidant/antioxidant factors are unbalanced")
REACTIVE OXYGEN SPECIES (ROS) • O 2 toxicity occurs when oxidant/antioxidant factors are unbalanced • Excessive ROS overwhelm antioxidants, which decline with age, which leads to cell death Bottom line: More oxygen ----> more unused oxygen ----> more ROS ----> more cell death

OK, BUT THAT’S AT THE CELLULAR LEVEL…I CAN’T SEE ALL THAT!

ROS damage is invisible, undetected or misinterpreted!

BUT HYPEROXIA CAN’T BE ALL BAD, RIGHT?
 Decreased wound infection 1) Oxidative process")
BENEFICIAL ASPECTS OF HYPEROXIA Related to ROS: 1) Decreased wound infection 1) Oxidative process is how our immune system kills pathogens 2) 2009 meta-analysis: 1) supplemental periop oxygenation is beneficial in preventing wound infections in colorectal surgery 3) Subsequent meta-analyses haven’t been as conclusive Related to increased Pa. O 2: 1) Increased tolerance to apnea 2) Decreased PONV? 1) 2013 meta-analysis: 1) high Fi. O 2 had weakly beneficial effect on nausea

“THAT ALL SOUNDS GREAT, BUT MY PATIENT JUST HAD ANESTHESIA…. THEY’RE SPECIAL RIGHT? ? ? ” RIGHT!

BUT WHAT HAPPENS WITH ANESTHESIA? Under/post-anesthesia: • p. H will likely be lower • Look at orange/green line • CO 2 will likely be higher (unless ventilated) • Look at green line • Temperature will usually be lower • Between red and yellow lines • DPG will be unchanged ____________________ • NET= • If temp normal, right shifted • If temp low (CO 2 benefit is cancelled out), not shifted =FAVORS TISSUE UNLOADING OF OXYGEN

A “RIGHT-SHIFTED” HB-O 2 DISSOCIATION CURVE • For the same Sa. O 2, Pa. O 2 will be higher! 70% 45% • This means that the pulse oximeter can read lower and the tissues will get the same amount of oxygen!

AND WHAT ELSE HAPPENS WITH ANESTHESIA? • There is a variable change in metabolic rate (and therefore, oxygen consumption) • The brain, the organ most susceptible to low oxygen levels, has a decreased metabolic rate under anesthesia • It uses less oxygen • Hypothermia also decreases the metabolic rate • There is a left shifted Hb-O 2 curve but the oxygen consumption is lower
 Right shifted Hb-O 2 curve = more unloading 2) Variable")
ANESTHETIC EFFECTS SUMMARIZED 1) Right shifted Hb-O 2 curve = more unloading 2) Variable (decreased? ) O 2 consumption
")
So, they probably need less oxygen (but most likely not more)

SPECIAL CONSIDERATIONS

CARDIOVASCULAR EFFECTS • Hyperoxia causes an acute decrease in SVR followed by a sustained increase in SVR • Systemic vasoconstriction, including the coronaries! • Increased left heart afterload • Also dilates pulmonary vessels • Decreased right heart afterload

CARDIOVASCULAR EFFECTS • Hyperoxia causes an acute decrease in SVR followed by a sustained increase in SVR • Systemic vasoconstriction, including the coronaries! • Also dilates pulmonary vessels • Decreased cardiac afterload/decreased preload • Hyper-oxygenation can reduce tissue perfusion and compromise O 2 transport !

CEREBRAL PERFUSION • Hyperoxia reduces cerebral blood flow • Recent multicenter study concluded that hyperoxic ventilation of CVA pts worsens mortality (Rincon 2014) • Traumatic Brain Injury- as evidenced by PET scan, blood flow is found to be reduced with 100% oxygen • Normoxia is advisable!
 are most susceptible")
INFANCY • Neonates and infants (particularly low birth weight or preemies) are most susceptible to damage from hyperoxia: • Retinopathy of prematurity • Bronchopulmonary dysplasia • Increased L -> R shunting in acyanotic heart disease (decreased PVR, increased SVR) • Can jeopardize a patent ductus arteriosus in ductal dependent lesions • Increased cerebral inflammation • Decreased cerebral blood flow ( decrease if concomitant hypocarbia)
 are most susceptible")
INFANCY • Neonates and infants (particularly low birth weight or preemies) are most susceptible to damage from hyperoxia: • Retinopathy of prematurity • Bronchopulmonary dysplasia • Increased L -> R shunting in acyanotic heart disease (decreased PVR, increased SVR) • Can jeopardize a patent ductus arteriosus in ductal dependent lesions • Increased cerebral inflammation • Decreased cerebral blood flow ( decrease if concomitant hypocarbia) Reynolds 2016

INFANCY • Bronchopulmonary dysplasia “Alveolar Simplification” Reynolds 2016

ELDERLY • Hallmark changes- altered transport, exchange and utilization of O 2 • Significantly increased production and accumulation of ROS and reduced antioxidant function • Higher Fi. O 2 leads to higher amounts of ROS potentially worsening conditions that are a result of ROS • Lungs in elderly are more susceptible to hyperoxia (increased ROS, enhanced pro-inflammatory cytokines, irreversible structural changes with degeneration of elastic fibers) • Hyperoxia compromises the contractile function of the diaphragm in aged subjects (hyperoxiainduced exacerbation of already present skeletal muscle destruction with age)
 • Possibly related to decreased cerebral blood")
ELDERLY CONTINUED… • Postoperative Cognitive Decline (POCD) • Possibly related to decreased cerebral blood flow/cerebral saturations • Animal models have incriminated periop high O 2 use as factors contributing to the development of Alzheimer’s disease (Oxidative stress obviously implicated, more studies needed to link hyperoxia to Alzheimer’s)

COPD • Oxidative stress may play a role in the development of COPD • Even a modest increase in FIO 2 (30%) for a short period (<1 hour) leads to oxidative stress and airway inflammation in COPD patients • O 2 suppresses hypoxic ventilatory drive which is crucial in maintaining alveolar ventilation in the presence of COPD • Pts at risk of hypercapnia should have O 2 saturation carefully titrated between 88 -92% “Alveolar Simplification”

One last thing to think about…. n o i t la i t n e v • O 2 suppresses hypoxic ventilatory drive which is crucial in maintaining alveolar ventilation in the presence of COPD A r a l o e lv o p y H • Pts at risk of hypercapnia should have O 2 saturation carefully titrated between 8892%
, the body will not")
CO 2 RESPONSE CURVE Under anesthesia (or after receiving opioids), the body will not respond to increased CO 2 with increased ventilation

ALVEOLAR GAS EQUATION PAO 2 = ( Fi. O 2 * (Patm – PH 2 O)) – (Pa. CO 2 / RQ). Pa. CO 2=((Fi. O 2 x (Patm-PH 2 O)) – Pa. O 2 ) RQ

ALVEOLAR GAS EQUATION PAO 2 = ( Fi. O 2 * (Patm – PH 2 O)) – (Pa. CO 2 / RQ). Pa. CO 2=((Fi. O 2 x (Patm-PH 2 O)) – Pa. O 2 ) RQ
) – PAO 2 ) RQ Fi. O")
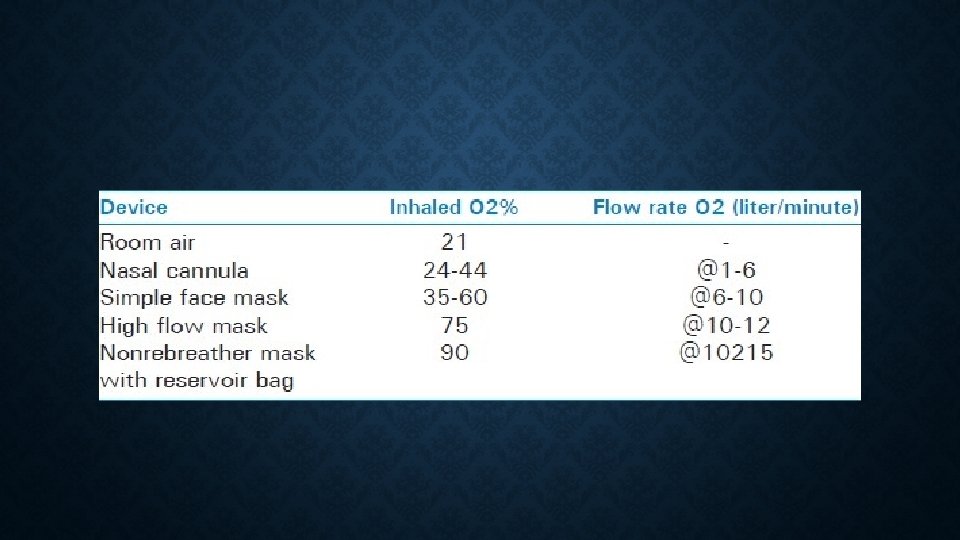
PACO 2=((FIO 2 X (PATM-PH 2 O)) – PAO 2 ) RQ Fi. O 2 of: = hypoxia at Pa. CO 2 of: 1) 21% (Room air) 1) 65 mm. Hg 2) 28% (2 L NC) 2) 105 mm. Hg 3) 60% (Non-rebreather) 3) 288 mm. Hg With a pulse oximeter, you can discover hypoventilation much earlier!** (**That is, unless you are blasting the patient with oxygen)

CLINICAL STUDIES

EMERGENCY MEDICINE • 688 patients arrived to ED requiring intubation/mechanical ventilation • Those who received hyperoxia (Pa. O 2 of 189 mm. Hg ~35% Fi. O 2) had a 29% mortality rate! • Versus 19. 4% in the “normoxia” • AND, 13. 2% in the HYPOXIA group!!! Page et al. 2018

• Cross-sectional study looking at Fi. O 2 practices during 1500 general anesthetics • FIO 2 <30% for 1% of patients • “Preventable” hyperoxia occurred in 83% of patients • Old age, emergency surgery and OLV a/w increased O 2 exposure • Use of volume control ventilation and PEEP a/w decreased O 2 exposure Suzuki et al. 2018

• Cross-sectional study looking at Fi. O 2 practices during 1500 general anesthetics • FIO 2 <30% for 1% of patients • “Preventable” hyperoxia occurred in 83% of patients • Old age, emergency surgery and OLV a/w increased O 2 exposure • Use of volume control ventilation and PEEP a/w decreased O 2 exposure Suzuki et al. 2018

• Patients undergoing OLV at more likely to have negative effects of hyperoxia Suzuki et al. 2018

• Prospective RCT of 1386 patients undergoing laparotomy randomized to receive Fi. O 2 of 80% or 30% • Included same Fi. O 2 for 2 hours postoperatively • Increased long-term mortality for 80% group (23. 2% vs. 18. 3%) • Statistically significant for cancer patients (but not in noncancer patients) Meyhoff et al. 2012

• Retrospective review of 74, 000 anesthetics to evaluate outcomes of patients divided into one of 5 groups based on Fi. O 2 • High Fi. O 2 found to be a/w major postoperative respiratory complications • High Fi. O 2 also a/w higher 30 -day mortality • Dose-dependent Staehr-Rye et al. 2017

OXYGEN GUIDELINES FROM BTS “As discussed in sections 4– 6 of this guideline, there is no evidence of benefit from above normal oxygen saturation in most clinical situations and there is evidence that excessive concentrations of oxygen can have adverse effects, even in some patients who are not at risk of hypercapneic respiratory failure. A target oxygen saturation range of 94– 98% will achieve normal or nearnormal oxygen saturation for most patients who are not at risk of hypercapneic respiratory failure. Furthermore, the suggested lower limit of 94% allows a wide margin of error in the oximeter measurement, thus minimizing the risk of any patient being allowed to desaturate below 90% due to inaccurate oximetry. ”

TO THIS POINT, HOPEFULLY I’VE CONVINCED YOU THAT…. • Increasing the Fi. O 2 isn’t the only way to increase oxygen tissue delivery • In fact, it’s not even the best way (remember DO ) 2 • There is little benefit to increasing oxygen saturation above 90% (remember Hb-O dissociation curve) 2 • Aiming for the right side of the Hb-O 2 dissociation curve isn’t necessary • Oxygen free radicals are bad…. worse than we might already suspect (remember ) • Higher levels of oxygen lead to higher levels of oxygen free radicals • The benefits of hyperoxia are limited • Patients under/following anesthesia don’t need more oxygen (and maybe they need less)

TO THIS POINT, HOPEFULLY I’VE CONVINCED YOU THAT…. • Hyperoxia actually reduces blood flow (remember increased SVR) • It likely increases mortality in CVA and TBI • Hyperoxia is particularly damaging to infants and elderly patients • ED patients requiring intubation with hyperoxia did WORSE than those with hypoxia! • COPD patients should never receive supratherapeutic FIO 2 • Causes airway inflammation • Abolishes hypoxic ventilatory drive • High Fi. O 2 masks alveolar hypoventilation (remember alveolar gas equation)

SO WHAT DO WE DO? ? ?

AVOID EXCESSIVE OXYGEN FOR: Infants/Neonates Traumatic brain injury Cerebral vascular accident Those intubated in the ED Eldery COPD People who dislike broccoli People who dislike oxygen free radicals
 “The")
“Contemporary medicine’s culture of oxygen assumes oxygen is always safe. ” (Kopp 2014) “The traditional approach to oxygen has been to prioritize the avoidance of hypoxemia while being tolerant of hyperoxemia. ” (Carvalho 2017)

AIMING FOR CULTURE SHIFT • “Too much oxygen may be as harmful as not enough” (Carvalho 2017) • “As with too little oxygen, too much is consequential” (Kopp 2014)

CULTURE SHIFT CONTINUED… • Maybe we should start to view oxygen as we do radiation… LOLA • Lowest Oxygen Level Acceptable standard (LOLA)

CAN WE MEASURE HOW MUCH OXYGEN IS ENOUGH? ? ? SVO 2

Habre 2014

Habre 2014

Questions?
 The pulmonary physician in critical care 2:")
REFERENCES • Leach RM, Treacher DF (2002) The pulmonary physician in critical care 2: oxygen delivery and consumption in the critically ill. Thorax 57: 170– 177 • Carvalho M, Soares M, Machado HS. Paradigms of Oxygen Therapy in Critically Ill Patients. J Intensive & Crit Care 2017, 3: 1. • W. Habre, F. Peták; Perioperative use of oxygen: variabilities across age. Br J Anaesth 2014; 113 (suppl_2): ii 26 -ii 36. doi: 10. 1093/bja/aeu 380 • Kopp VJ. Oxygen: Achieving a Rational Balance in Anesthetic Care. Anesthesiology News Guide to Airway Management 2014 • J. J. Pandit; Volatile anesthetics and the hypoxic ventilatory response: effects, clinical implications, and future research. Semin. Anesth. Perioperat. Med. Pain, 26 (2007), pp. 49 -57 • C. L. Reynolds, S. Zhang, A. K. Shrestha, R. Barrios, B. Shivanna. Phenotypic assessment of pulmonary hypertension using highresolution echocardiography is feasible in neonatal mice with experimental bronchopulmonary dysplasia and pulmonary hypertension: a step toward preventing chronic obstructive pulmonary disease. Int. J. Chronic Obstr. Pulm. Dis. , 11 (2016), pp. 1597– 1605 • Rincon F, Kang J, Maltenfort M, et al. Association between hyperoxia and mortality after stroke: a multicenter cohort study. Crit Care Med 2014; 42: 387– 96 • Page D, Ablordeppey E, Wessman BT, et al. Emergency department hyperoxia is associated with increased mortality in mechanically ventilated patients: a cohort study. Critical Care. 2018; 22: 9. doi: 10. 1186/s 13054 -017 -1926 -4.
- Slides: 69