Superior vena cava syndrome SVCS prof L Grozdinski
 prof. L. Grozdinski assoc. prof. Ivo Petrov CITY Clinic")


















- Slides: 25
Superior vena cava syndrome (SVCS) prof. L. Grozdinski assoc. prof. Ivo Petrov CITY Clinic - Sofia dr Nikolay Iliev
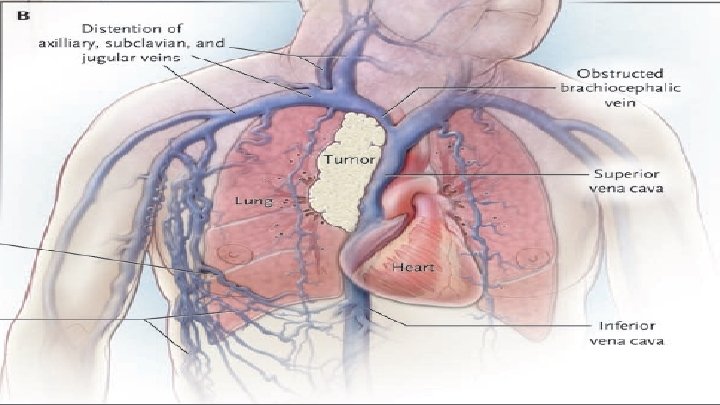
Definition q Vena cava superior syndrome is a group of symptoms caused by a disturbance of the blood flow in it, due to a stenosis or thrombosis q First described by William Hunter in 1757 in a patient with syphilistic aneurism of ascending aorta
Epidemiology q Approximately 15 000 new cases per year only in USA
Etiologic Factors: 90% malignant conditions ; q~50% - non–small-cell lung cancer; q~25% - small-cell lung cancer; q~10%- lymphoma; q - 35% - thrombosis – implantation of intravascular devices - catheters and pacemakers. q
Signs and symptoms q q Facial edema Distended neck veins Distended chest veins Dyspnea 60 - 100% 27 - 86% 38 - 70% 25 - 75%
Clinical diagnosis In most cases, symptoms are progressive over several weeks; q In some cases – symptoms may improve as collateral circulation develops; q The severity of the symptoms is important in determining the urgency of intervention q
Management q Most data regarding management are from case series; randomized trials are scarce q Management is guided by: severity of the symptoms underlying malignant conditions anticipated response to treatment q q q
Radioterapy q Complete relief of the symptoms of obstruction of the superior vena cava in 78% of q patients with small-cell lung cancer and 63% of those with non–small-cell lung cancer. BUT: q q Requires a tissue diagnosis Objective criterias of the change in vena caval obstruction are not paralleled criterias of symptomatic improvement based on patients’ reports. Completely relief of vena caval obstruction as measured on serial venograms was noted in 31% of the patients and partial relief in 23% of the patients. Development of collateral circulation may contribute to improvement of symptoms
Systemic Chemotherapy q q Complete relief of symptoms in approximately 80% of patients with non-Hodgkin’s lymphoma or small-cell lung cancer and in 40% of those with non–small-cell lung cancer BUT: review of 2 randomized studies and 44 observational studies concluded that patients with lung cancer have no clinically significant difference in the rate of relief from the superior vena cava syndrome whether chemotherapy, radiotherapy, or chemotherapy with radiotherapy was used
Surgery q q Sternotomy or thoracotomy with extensive resection and reconstruction of the superior vena cava Operative mortality - ~ 5%; patency rates - of 80% to 90% 10% reocclusion BUT: some patients with severe SVCS cannot undergo mediastinoscopy/anesthetize because of their inability to maintain a supine position;
Placement of an Intravascular Stent q q The stent can be placed before a tissue diagnosis is available Useful procedure for patients with severe symptoms such as respiratory distress that require urgent intervention Strongly considered for patients with mesothelioma, which tends not to respond well to chemotherapy or radiation More prompt relief of symptoms than in radiation or chemotherapy - cyanosis is usually relieved within hours, and edema resolves within 48 to 72 hours in most series (response rate - 75 to 100%)
Placement of an Intravascular Stent q q q Technical success rate – 95 -100% Complications of stent placement 3 -7% - infection, pulmonary embolus, stent migration, hematoma at the insertion site, bleeding, perforation, recurrent laryngeal palsy Late complications - bleeding (1% to 14% of patients) and death (1% to 2% of patients) due to anticoagulation
Placement of an Intravascular Stent q q q Rate of relapse - 11%. However 78% of these relapses were successfully managed by repeated intravascular intervention Patients with brain metastasis may undergo stent placement because of the potential of the superior vena cava syndrome to exacerbate cerebral edema. In these cases at least a temporary anticoagulation is needed which is associated with cerebral hemorrhage However there are no absolute contraindication
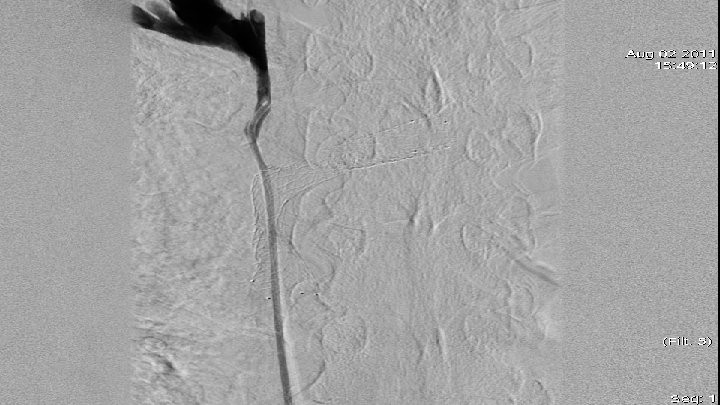
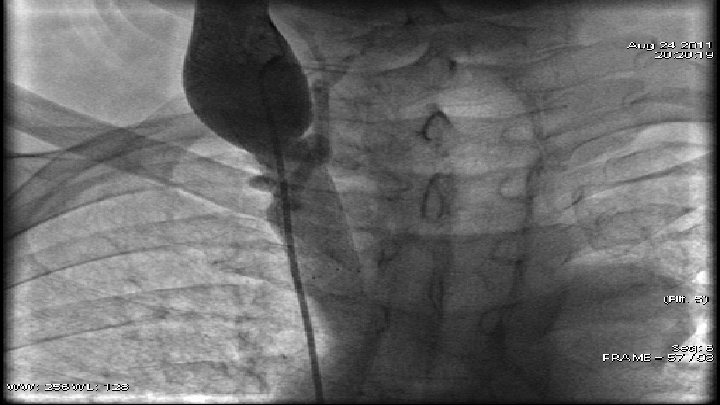
Case 1 q q q 66 y old patient May 2010 – small cell lung cancer was diagnosed April 2011 – venography - high grade stenosis of v. brachiocephalica billateral, PTA and stent implantation of v. brachiocephalica sinstra and baloon angioplasty of v. brachiocephalica dextra July 2011 – CT scan data for restenosis of v. brachiocephalica dextra August 2011 – venography - 90% restenosis of v. brachiocephalica dextra – after predilalatation was implanted stent.
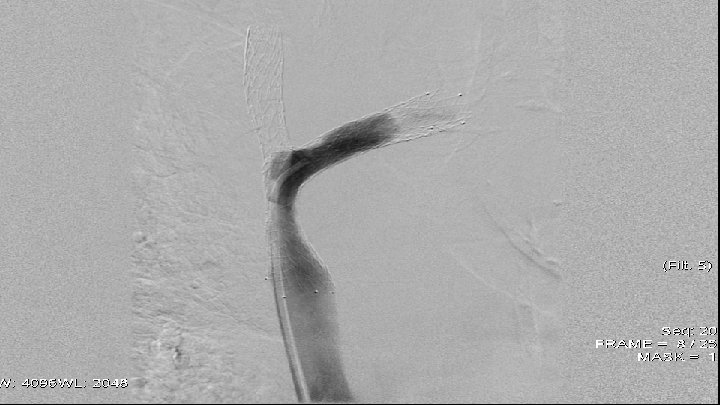
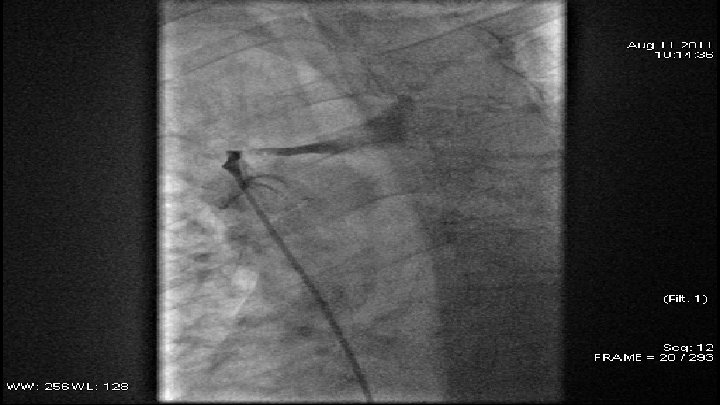
Case 2 q 59 y. o. patient q June 2011 - diagnosed with small-cell lung cancer q August 2011 - angiographic data of subtotal occlusion of VCS. q. PTA – baloon dilatation and stent implantation
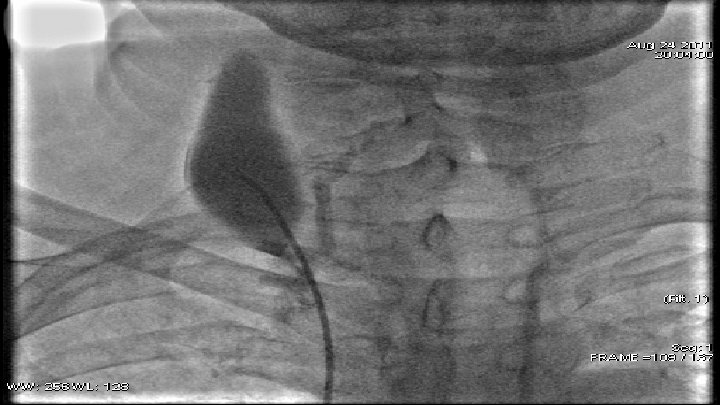
Case 3 q 66 y old patient q 2000 г. - non-Hodgkin lymphoma was diagnosed. q Later thrombosis of the right subclavian vein q March 2011 г. - СТ data – partial thrombosis of truncus brachiocephalicus q August 2011 г. - venography – subtotal occlusion of v. braciocephalica sin. and occlusion of v. braciocephalica dex. q After balloon predialatation - v. braciocephalica sin. was implanted stent
Conclusions q q In patients with life-threatening symptoms or signs of obstruction of the superior vena cava, the placement of an intravascular stent can provide rapid relief of the symptoms Outcomes and complications of PTA compared with chemotherapy/radiotherapy (associated with risks of excessive toxic effect) are in favor of PTA Stent placement does not reduce the likelihood of cure of the underlying malignant condition and should not compromise the choice of appropriate therapy There are not routine imaging and anticoagulation protocols. Expert’s consensus on definition of clinical and imaging follow up algorithms is needed