Sugeng Rawuh Seminar Clinical Updates 2011 simposium satelit
















 changed?")


























 Lower/Upper tract infections Adult:")












- Slides: 59
Sugeng Rawuh…………. .
Seminar “Clinical Updates 2011” simposium satelit Tema : Dysuria Hari/Tanggal : Minggu, 16 Januari 2011 Tempat : Auditorium II FK UGM
Semangat !! • 100% • Tambah Pintar, Sehat, Hebat ! Bisa !! • Jam • HP
Mengesankan!!
Daftar penyakit dikelompokkan menurut sistem, organ dan tahapan usia. Berikut ini tingkat kemampuan yang diharapkan akan dicapai di akhir pendidikan. Tingkat kemampuan yang diharapkan dicapai pada akhir pendidikan dokter
Soal 1 Tingkat kemampuan 4 berarti: A. Level ini mengindikasikan overview level. Bila menghadapi pasien dengan gambaran klinik ini dan menduga penyakitnya, Dokter segera merujuk. B. Dokter mampu merujuk pasien secepatnya ke spesialis yang relevan dan mampu menindaklanjuti sesudahnya C. Dokter dapat memutuskan dan mampu menangani problem itu secara mandiri hingga tuntas. D. Dokter dapat memutuskan dan memberi terapi pendahuluan, serta merujuk ke spesialis yang relevan (bukan kasus gawat darurat). E. Dokter dapat memutuskan dan memberi terapi pendahuluan, serta merujuk ke spesialis yang relevan (kasus gawat darurat).
Soal 2 Yang termasuk Tingkat kemampuan 4 di bidang Nefrologi: A. Urinary tract infection B. Acute tubular necrosis C. Horse shoe kidney D. Uncomplicated Pyelonephritis E. Batu Ginjal
Kidney 1. Cortical adenoma 1 2. Renal cell carcinoma 3. Wilm's tumor 2 1 Nefrourologi 1. Acute renal failure 2. Chronic renal failure 3. Nephrotic syndrome 2 2 2 4. Acute glomerulonephritis 5. Chronic glomerulonephritis 3 A 7. Renal colic 3 A 6. Interstitial nephritis 3 A 1 8. Urinary stone diseases or urinary calculi without colic 3 A 9. Polycystic kidneys symptomatic 10. Urinary tract infection 2 4 11. Acute tubular necrosis 12. Horse shoe kidney 2 2 13. Uncomplicated Pyelonephritis 14. Urinary incontinence 15. Nocturnal and diurnal enuresis 16. Prostatitis 3 A 4 2 2
Soal 3. Pengelolaan Disuria: A. Dibedakan kelompok Anak dengan yang lain. B. Dibedakan kelompok Geriatri dengan yang lain. C. Dibedakan kelompok Laki laki dan perempuan. D. Terapi dibedakan kelompok ISK atas dan ISK bawah. E. Dibedakan kelompok Penyakit Penyerta.
Dysuria Yes Child, geriatric patient, adult male No Yes UA Vaginal complaints No Yes Signs or symptoms of pyelonephritis No Yes Risk factors of occult pyelonephritis No Yes Recent Hx recurrent UTI No Treat uncomplicated lower tract infection Evidence of UTI: pyuria, hematuria, nitrete positive Pelvic exam Yes Culture urine Treat recurrent lower tract infection No UA Evidence of UTI pyuria, hematuria, nitrate No Yes Culture and investigate non UTI causes of dysuria Yes Culture urine and investigate non UTI causes of dysuria Culture urine Localize site of infection Lower tract Upper tract Treat upper tract infection Figure 28. 1 Algorithm for the management of dysuria
Dysuria: Causes and associated ● ● Reiter’s syndrome ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● Weakness ● Vomiting ● Vaginal discharge Urinary urgency ● ● ● Urine stream, diminished ● ● ● Urinary frequency ● ● Urethral discharge ● ● ● Suprapublic pain Perineal pain ● Straining to void Noctruria ● ● Nausea Hermaturia ● Fever Fatingue Erythema of meatus Costovertebral angle tendernes ● ● Paraurethral gland inflammation Prostatitis (acute) Prostatitis (chronic) Pyelonephritis (acute) Urethral syndrome Urethritis Urinary obstruction Vagiritis Constipation ● Back pain ● Flank pain Cystitis (bacterial) Cystitis (chronic interstitial) Cystitis (tubercular) Cystitis (viral) Diverticulitis Anorexia Common causes Appendicitis Bladder cancer Major associated signs and symptoms Abdominal pain SIGNS & SYMPTOMS ● ● ●
L = 7, 61 P = 8, 64
Algoritme Disuria
Differential Diagnosis of Dysuria in Otherwise Healthy Women of Reproductive Age Diagnosis Frequency 1. Lower tract UTI Very common (70% of women with dysuria) Common Uncommon* Rare 2. 3. 4. 5. Vaginitis Upper tract UTI Urethritis Perineal trauma *May be more common in college health centers and reproductive health clinics UTI, urinary tract infection.
Key Elements of the History and Physical Examination for Dysuria Diagnosis Question or Maneuver Sensitivity Specificity LR+ LR- Nocturia 0. 67 0. 62 1. 8 0. 53 Dysuria 0. 80 0. 50 1. 6 0. 40 Urgency 0. 39 0. 71 1. 3 0. 86 Frequency 0. 87 0. 32 1. 3 0. 41 Offensive odor of urine 0. 20 0. 85 1. 3 0. 94 Chills and rigors 0. 32 0. 87 2. 5 0. 78 Fever 0. 44 0. 80 2. 2 0. 70 Nausea and fomiting 0. 24 0. 84 1. 5 0. 90 Flank pain 0. 48 0. 67 1. 5 0. 78 UTI Pyelonephritis UTI, urinary tract infection Data are from References 75 and 76
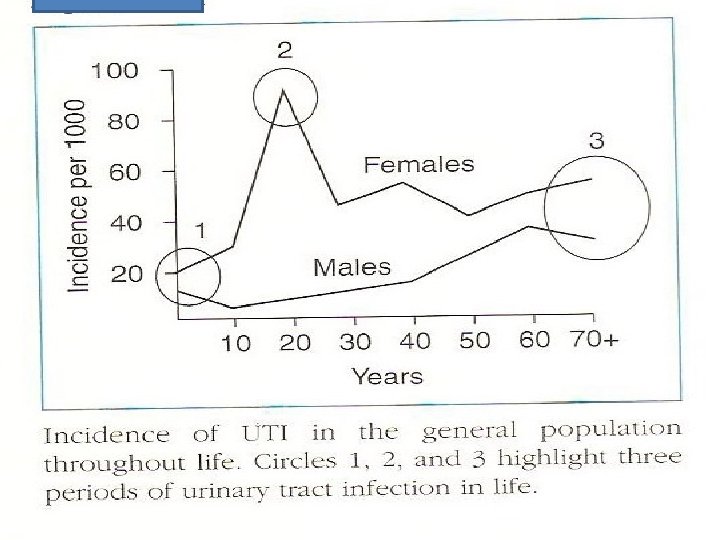
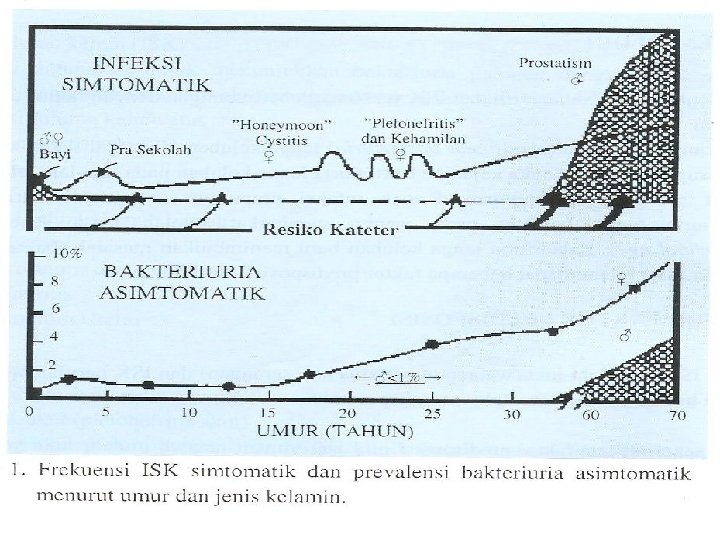
Guiding Questions UTIs 1. How has the epidemiology of urinary tract infections (UTIs) changed? 2. What are the differences between asymptomatic bacteriuria, cystitis, and pyelonephritis? 3. What distinguishes an uncomplicated UTI from a complicated UTI and how do treatments vary?
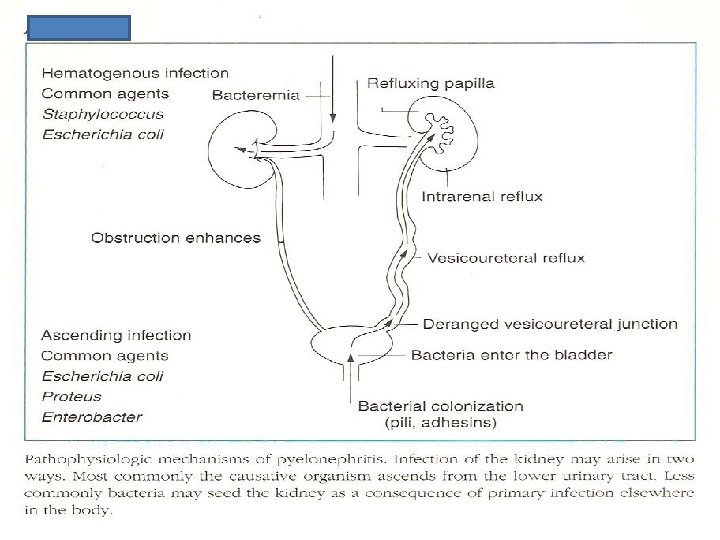
Guiding Questions UTIs 4. Are particular patient populations at increased risk for UTI and are adverse outcomes a concern? 5. What is the pathogenesis of UTI? 6. What impact does bacterial antibiotic resistance have on UTI? 7. What are two important types of complicated renal infections?
KEY POINTS Urinary Tract Infection 1. Infections in different locations within the urinary tract present with similar symptoms. 2. Fever in a patient with LM means tissue invasive infection. 3. The duration of therapy and the pathogens responsible for UTT are different in uncom plicated and complicated UIT. 4. Infection of the urinary tract with Staphylococcus aureus requires evaluation for a hematogenous source of infection.
KEY POINTS Risk Factor for and pathogenesis of UTI 1. Patient specific risk factors for UTI can be modified to decrease the incidence of infection. 2. Pathogen specific virulence factors are not the cause of antibiotic resistence.
Soal 4 Penyebab Terbanyak ISK A. B. C. D. E. coli Proteus Klebsiella, enterobacter Enterococcus Pseudomonas
Frequency of bacteria causing UTI Causative organism E. coli Proteus Klebsiella, enterobacter Enterococcus Staphylococcus Pseudomonas Other % primary infection 70 90% 2% 7. 5% 2. 5% 5% 2. 5% % early relapse 60% 15% 20% 5% % Hospital acquired 48% 10% 15% 6% 6% 15% <1%
Characteristics of Urine Tests for Primary Care Patients with Dysuria 1 Test Sensitivity Specificity LR+ LR 0. 76 0. 49 0. 90 0. 46 0. 85 0. 65 1. 4 4. 4 2. 6 0. 5 0. 6 0. 15 0. 95 0. 85 0. 91 0. 82 0. 44 0. 85 0. 99 0. 48 0. 65 0. 88 6. 3 85 1. 7 2. 3 3. 7 0. 06 0. 15 0. 19 0. 28 0. 60 Dipstick Leukocyte esterase (LE) Nitrite Either LE or nitrie Sediment Microscopy 1 bacterium/HPFb 10 bacteria/HPFb 5 WBC/HPFc 10 WBC/HPFb 5 RBC/HPFa HPF, high power field; RBC, red blood count; WBC, white blood count 1 Baeiley BL. Urinalysis predictive of urine culture results. J Fam Pract 1995; 40: 45 50. 2 Deville WL , Yzermans JC, van Duijin NP, Bezemer PD, van der Windt DA, Bouter L. M. The urine dipstick test useful to rule out infections. A meta analysis of the accuracy. BMC Urol. 2004; 4: 4.
KEY POINTS Diagnosis of Urinary Tract Infection 1. For an uncomplicated patient, a history consistent with UTI and pyuria on urinalysis establishes the diagnosis. 2. For a complicated patient, a culture and sensitivity must be performed.
Soal 4. Prinsip Pengelolaan Disuria Wanita A. B. C. D. Terapi jangka pendek Evaluasi 4 7 paska terapi Urinalisis baik, tanpa terapi antibiotika. Urinalisis jelek, kultur negatif: terapi Chlamydia E. Antibiotika sesuai Kultur, sensitivitas dan angka kuman.
WHO PRESENT WITH COMPLAINTS OF DYSURIA AND FREQUENCY Treat with short course therapy Follow up 4 7 days later Asymptomati No further intervention Both negative Observe, treat with urinary analgesia Asymptomati Urinalysis urine culture Pyuria, no bacteriuria Bacteriuria with or without Treat for Chlamydia trachomatis Treat with extended course Clinical approach to the woman with dysuria and frequency. (Modified from Tolkoff-Rubin NE, Wilson ME, Zuromskis P, et al: Singledose amoxicillin therapy of acute uncomplicated urinary tract infections in women. Antimcrob Agents Chemother 25: 626, 1984. ) Figure 15 -1.
KEY POINTS Antibiotics for the Treatment of UTI 1. Antimicrobial resistant bacteria are more common, therefore, broad spectrum empiric coverage with a quinolone is appropriate. 2. In order to avoid inducing further antibiotic resistance, once culture and sensitivity result are available, antibiotic therapy is changed to the narrowest possible spectrum.
Soal 5. “Red Flags” for a Complicated UTI A. Male gender B. Prepubertal or geriatric age C. Symptoms for more than 7 days D. An immunosuppressing condition E. An episode of acute pyelonephritis within the past year
“Red Flags” for a Complicated Infection 1. Male gender 2. Prepubertal or geriatric age 3. Symptoms for more than 7 days 4. An immunosuppressing condition 5. An episode of acute pyelonephritis within the past year Adapted from Johnson JR, Stamm WE. Diagnosis and treatment of acute urinary tract infections. Infect Dis Clin North Am 1987; (14): 773 791.
“Red Flags” for a Complicated Infection 6. Known anatomic abnormality 7. Diabetes mellitus 8. Fever 9. Flank pain or tenderness Adapted from Johnson JR, Stamm WE. Diagnosis and treatment of acute urinary tract infections. Infect Dis Clin North Am 1987; (14): 773 791.
Factors predisposing to recurrent UTI Local factors 1. Impaired bladder emptying, e. g. due to prostatic hypertrophy or neuromuscular problems 2. Bladder or renal calculi 3. Renal cysts 4. Anatomical anomaly, e. g. horseshoe kidney 5. Indwelling urinary catheter or recurrent bladder instrumentation 6. Postmenopausal vaginal atrophy
Factors predisposing to recurrent UTI Systemic factors 1. Diabetes mellitus 2. Immunosuppression 3. Pregnancy
Factors Suggesting Occult Pyelonephritis Or Complicated UTI 1. Diabetes 2. Pregnancy 3. Male patient 4. Childhood UTI 5. Elderly patient
FACTORS SUGGESTING OCCULT PYELONEPHRITIS OR COMPLICATED URINARY TRACT INFECTION 6. Indwelling catheter 7. Immunosupression 8. Urologic anatomic abnormality 9. Symptoms for >7 days 10. Recent urinary tract instrumentation or antibiotics
Criteria That Define a Complicated UTI 1. Documented fever >38°C 2. Symptoms of dysuria or urgency present for >7 days 3. Symptoms of vaginitis present (e. g. , vaginal discharge or irritation) 4. Symptoms of abdominal pain, nausea, or vomiting 5. Gross hematuria in patients >50 years Presence of immunosuppression (e. g. , current use of chemotherapy or transplant immuno suppression) 6. Diabetes mellitus
7. Known pregnancy 8. Chronic renal or urologic abnormalities other than stress incontinence (e. g. , PKD, neuro genic bladder, CKD) 9. Recent or persistent occurrence of urinary tract stones 10. Urinary catheterization or other urologic proce dure within 2 weeks 11. Discharge from hospital or nursing home within 2 weeks 12. Treatment for UTI within 2 weeks Recurrent or symptomatic UTI Abbreviations: UTI, urinary tract infection; PKD, polycystic kidney disease; CKD, chronic kidney disease. Modified from Bent, S. , Saint, S. Am J Med 113: 20 S-28 S , 2002 with permission.
Inherited or Acquired Host Susceptibility Factors for UTI GENETIC Blood group antigen Nonsecretor status Increased adhesion receptors BIOLOGIC BEHAVIORAL Congenital abnormalities Sexual intercourse Urinary obstruction Calculi Diabetes mellitus Anatomic abnormalities Residual urine Atrophic vaginitis Urinary incontinence Prior history of UTI Maternal history of UTI Childhood history of UTI Catheters/stents/ foreign bodies Condom catheters Immunologic abnormalities (HM Renal transplant Use of diaphragm Use of spermicides Antimicrobial use OTHER Decreased mental status
Inherited or Acquired Host Susceptibility Factors for UTI GENETIC 1. Blood group antigen 2. Nonsecretor status 3. Increased adhesion receptors
Inherited or Acquired Host Susceptibility Factors for UTI BIOLOGIC 1. Congenital abnormalities 2. Urinary obstruction 3. Calculi 4. Diabetes mellitus 5. Anatomic abnormalities 6. Residual urine 7. Atrophic vaginitis
Inherited or Acquired Host Susceptibility Factors for UTI BIOLOGIC 8. Urinary incontinence 9. Prior history of UTI 10. Maternal history of UTI 11. Childhood history of UTI 12. Catheters/stents/ foreign bodies 13. Condom catheters 14. Immunologic abnormalities (HM 15. Renal transplant
Inherited or Acquired Host Susceptibility Factors for UTI BEHAVIORAL Sexual intercourse Use of diaphragm Use of spermicides Antimicrobial use OTHER Decreased mental status
Evidence for Effectiveness of Recommended Therapies Intervention Strength of Recommendation* Management of uncomplicated lower tract urinary tract infection (UTI) Oral antibiotics Cranberry juice Increased fluid intake Management of uncomplicated upper tract UTI Oral antibiotics (in healthy women) No need for imaging (in healthy women) Prevention of UTI Cranberry juice Increased fluid intake Behavioral interventions *A = consistent, good quality patient oriented evidence; B = inconsistent or limited quality patient oriented evidence; C = consensus, disease oriented evidence, usal practice, expert opinion, or case series. For information about the SORT evidence rating system, see http: //www. aaf. org/afpsort. xml.
Oral Drug Therapy Tract Infection Drug Indications Dosage Trimethoprim/sulfametho Lower or upper tract Adult: double strength xazole (TMP/SMX) infections formulation bid (Septra, Bactrim, others) Child: 8 mg TMP/40 mg SMX/kg/day; divided bid Trimethoprim (Trimpex, Proloprim, others) Lower tract infections Adult: 100 mg bid Nitrofurantoin (Macrodantin, Macrobid, Furadantin) Lower tract infections Adult: 50 100 mg qid or 100 mg bid (Macrobid, others) Child: 5 7 mg/kg/day; divided qid Cephalexin (Keflex) Lower/Upper tract infections Adult: 250 500 mg qid Child: 25 50 mg/kg/day divided qid Cefixime (Suprax) Lower/Upper tract infections Adult: 400 mg daily Child: 8 mg/kg/day divided qid
Oral Drug Therapy Tract Infection Drug Indications Dosage Cefpodixime (Vantin) Lower/Upper tract infections Adult: 100 mg bid Child: 10 mg/kg/d divided bid Ciprofloxacin (Cipro) Lower tract infections Upper tract infections Adult: 250 mg bid Adult: 250 500 mg bid Levofloxacin (Levaquin) Lower tract infections Upper tract infections Adult: 250 mg qd Amoxicillin/clavulanate (Augmentin) Upper tract Adult: 875 mg bid infections (only if Child: 45 mg of amoxicillin gram positive component divided bid organism suspected) Note: Length of treatment of outpatient Lower tract infection (oral antibiotics): female adult 7 10 days, healthy geriatric female 3 days; all other geriatric patients 7 14, child older than 2 months 7 14 days. For outpatient with upper tract infection (oral antibiotics): female adult 7 14 days, male adult 14 days; geriatic patient 14 days or child 7 14 days. For hospitalized patient with upper tract infection and initial IV antibiotics (switch to oral antibiotics when stable): female adult 14 days; male agult, geriatic patient, 21 days or child 7 14 days.
KEY POINTS Pregnant Women 1. Bacteriuria and UTI have negative consequences on the outcome of pregnancy 2. All pregnant women must be treated.
KEY POINTS The Spinal Cord Injury Patient 1. Spinal cord injury patients are at high risk for UTI because of chronic indwelling catheters and loss of coordinated micturition. 2. Antimicrobial resistant organisms are common pathogens because SCI patients have multiple antibiotic exposures.
Soal 6 Kondisi ini memerlukan penanganan lebih serius: A. Pasien Diabetes B. Pasien Hipertensi C. Pasien Batu ginjal D. Pasien cangkok ginjal E. Emphysematous Pyelonephritis
KEY POINTS Diabetic Patient 1. Diabetic patients are at high risk for developing complications of UTI. 2. Antimicrobial resistant pathogens are more common in diabetic patients. 3. Diabetic are at greater risk for atypical pathogens such as fungi.
KEY POINTS Transplant Patient 1. The incidence of UTI during the first three posttransplant months is 30%. 2. Pyelonephritis in a renal transplant patient can cause acute renal failure. 3. Treatment for cystitis is extended to 7 10 days and treatment for pyelonephritis is extended to 4 weeks.
KEY POINTS Emphysematous Pyelonephritis 1. Emphysematous pyelonephritis occurs most commonly in patients with diabetes mellitus. 2. Gas forming organisms such as Escbericbia coli and Klebsiella pneumoniae are associated with this form of pyelonephritis. 3. Treatment is based on class of lesion. Antibiotics and either percutaneous drainage or nephrectomy are available therapeutic options.
KEY POINTS Xanthogranulomatous Pyelonephritis 1. Xanthogranulomatous pyelonephritis can masquerade as a renal malignancy. 2. Gram negative organisms underlie infection in XGP. 3. Computed tomography scan best demon strates the extent of disease, excludes malig nancy, and identifies the presence of renal stones. 4. The histopathology of XGP is characterized by necrotic tissue, cellular infiltration, and lipid laden macrophages (xanthoma cells). 5. Antibiotics and nephrectomy (complete or partial) are required to treat XGP.
KESIMPULAN I. Lakukan investigasi penderita Disuria, kemungkinan I S K II. Penetapan diagnosis yang sahih III. Terapi/ pencegahan disesuaikan keadaan khusus penderita
Soal 7. Kapan pasien disuria dirujuk? A. Kreatinin klirens > 60 B. Kreatinin serum >2 mg/d. L C. Laju Filtrasi Glomerulus <50 m. L/menit D. Kadar Ca x kadar PO 4 < 30 E. ISK dan atau Pielonefritis complicated
PANDUAN 1 Pasien dengan kreatinin serum >2 mg/d. L dan atau TKK (Tes Klirens Kreatinin)/LFG (Laju Filtrasi Glomerulus) <50 m. L/menit mempunyai faktor prognosis yang buruk sehingga memerlukan penanganan yang khusus dan sebaiknya dirujuk ke dokter spesialis penyakit dalam/konsultan ginjal hipertensi.
Langkah-langkah pencegahan holistik Penyakit Ginjal: G ula darah terkendali I nfeksi Saluran kencing diatasi/dihindari N o, hipertensi J auhi obat/makanan/minuman racun Ginjal A ir minum/ air putih secukupnya L anjutkan perilaku hidup SEHAT
Pantun Penutup Kapal angkutan berlayar Lebar, Minum Serbat, nikmat bersama. Kekuasaan- Kekayaan boleh dikejar, Ilmu yang bermanfaat, paling utama ! TERIMA KASIH