Substance Use Disorders 101 Robert Ochsner MD Overview

Substance Use Disorders 101 Robert Ochsner, MD

Overview Definition Identification/Stats Inheritance/Contributing factors Epigenetics Risk Factors Effects on the Brain Treatment Approach

Addiction: The Great Masquerader IT CAN LOOK LIKE ANYTHING Affective Anxiety Disorders Personality Psychotic Organic Disorders and Neurological Disorders

The Latest News Headlines on Drug Abuse CDC Report Finds Overdose Deaths Rose 21 Percent in 2016 Nov. 3, 2017 Breaking Down the Uptick in Adolescent Overdoses Nov. 3, 2017 Donald Trump Officially Declares Opioid Crisis a Public Health Emergency Oct. 26, 2017 What Is the Opioid Crisis? 5 Facts on the Addiction Epidemic Oct. 26, 2017 Opioid Crisis Spurs Change at Medical Schools Oct. 19, 2017 How to Break Unhealthy Habits During Pregnancy Oct. 5, 2017 Parents: Get Inside Your Adolescent’s Brain to Prevent Addiction Sept. 28, 2017 CVS to Enforce New Limits on Opioid Prescriptions Sept. 22, 2017 Mc. Caskill Releases First Findings from Opioids Investigation Sept. 6, 2017

Take Action Against Addiction

As pill mills fade away, heroin fills the void There are signs that heroin is returning as a cheap alternative to prescription pills, the by-product of Florida’s successful crackdown on pill mills. Read more here: http: //www. miamiherald. com/living/article 1951397. html#storylink=cpy
")
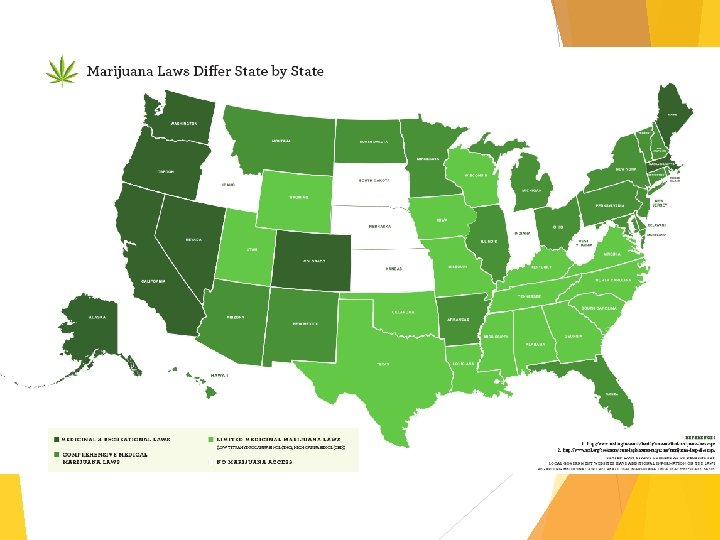
23 states have Medical Marijuana Laws (2015)

ASAM Definition 2014 Addiction is a primary, chronic disease of brain reward, motivation, memory and related circuitry. Dysfunction in these circuits leads to characteristic biological, psychological, social and spiritual manifestations. This is reflected in an individual pathologically pursuing reward and/or relief by substance use and other behaviors.

ASAM Definition 2014 Addiction is characterized by inability to consistently abstain, impairment in behavioral control, craving, diminished recognition of significant problems with one’s behaviors and interpersonal relationships, and a dysfunctional emotional response. Like other chronic diseases, addiction often involves cycles of relapse and remission. Without treatment or engagement in recovery activities, addiction is progressive and can result in disability or premature DEATH.

DSM-5 Definition: Substance Use Disorders 1. Using larger amounts or over a longer period of time than intended. 2. Persistent desire or unsuccessful efforts to cut down or control 3. Great deal of time spent in obtaining, using, and recovering from 4. Craving or a strong desire or urge to use 5. Recurrent use resulting in failure to fulfill major role obligations 6. Continued use despite persistent or recurrent social or interpersonal problems caused or exacerbated by use 7. Important social, occupational, or recreational activities are given up or reduced because of use 8. Recurrent use in physically hazardous situations 9. Continued use despite knowledge of having a persistent or recurrent physical or psychological problems that is caused or exacerbated by use. 10. Tolerance defined by need for increased amounts to achieve desired effect or markedly diminished effect with continued use of the same amount 11. Withdrawal either withdrawal symptoms, or continued use to relieve or avoid withdrawal

DSM-5 Definition: Substance Use Disorder Mild: Presence of 2 -3 symptoms Moderate: Presence of 4 -5 symptoms Severe: Presence of 6 or more symptoms

non e ALC mod erat e non-use Continuum Model OH OL & DRU GC ON SUM sub stan PTI tial ON hea vy misuse abuse addiction re e v se e non mild L O H O C L A us S o i M r E e L s B O PR G RU D &

Illicit drug use in America has been increasing, 22. 5 million Americans aged 12 or older (8. 7% of the population) in 2011, up from 8. 3 % in 2002. US Dept. of Health and Human Services, National Institutes of Health, Nationwide Trends, Dec 2012

Top Drugs among 8 th and 12 th Graders, Past Year Use

Source of Prescription Narcotics among Past Year Non-medical Users, 12 Grade

Stimulantsdata from 2014 University of Michigan Past year non-medical use of the stimulant Adderall remained relatively steady at 6. 8 percent for high school seniors.

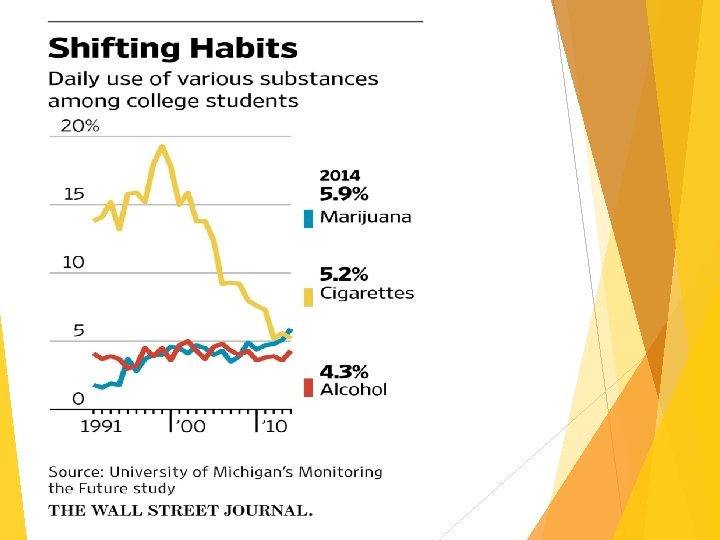
Drug Use Among College Students Data from 2014 University of Michigan

Are adolescents more susceptible to alcohol than adults? Most certainly YES 1. Reduced sensitivity to intoxication 2. Increased sensitivity to social disinhibitions 3. Greater adverse effects to cognitive functioning

What’s the big deal about kids drinking anyways? ? ? Have you ever seen a group of drunk teenagers? Demeaning behaviors Risk taking behaviors Accidents Teenage brain effects before 18 yrs old

Alcohol and Teenagers: Date Rape – one to two-thirds of teen sexual assaults involve alcohol 18% of Females/ 39% Males say it is acceptable for a boy to force sex if the girl is stoned or drunk 40% of children who start drinking before age 15 will become alcoholics In television 9 out of 10 drinkers are portrayed as having no effects or only positive outcomes from their alcohol consumption

Age of Onset & Risk

Two Powerful Questions

Inheritance - Genes

Developmental Issues and Epigenetics

Prenatal Drug Exposure

Epigenetics - Methylation

What is the Field of Epigenetics? Changes in gene expression that occur by a mechanism other than change to the DNA sequence. Gene-regulatory information that is not expressed in DNA sequences by transmitted from one generation (of cells or organisms) to the next. Epigenetics means “above” or “on top of genetics”.

What Does Epigenetics Mean?

Epigenetic Modulation

What Contributes to the Development of Substance Use Disorders/ Addiction? Genes/ genetic variation Account for about 40 -50 % of having a substance use problem is genetic. Alcohol liking or disliking is linked— alcohol and aldehyde dehydrogenase Males are twice as likely as females to have alcohol or drug addiction Environment Family's beliefs and attitudes – Exposure to Parental SUDs Peer group that encourages drug use Adverse Childhood Events Trauma, mental health, physical health, household dysfunction Age of Onset Earlier the age of onset of use…

What Contributes to the Development of Substance Use Disorders/ Addiction? Adverse Childhood Events Trauma, Mental health, Physical Health, Household Dysfunction 5 or more childhood events are 7 -10 times more likely to report illicit drug use and addiction Individuals seeking treatment for alcohol use disorders show a high prevalence of childhood adversity and PTSD Age of Onset Earlier the age of onset of use… 40 % if onset 14 y. o. or younger 10% if onset is 20 years and older

Risk Factors for Alcohol and Drug Use Psychiatric Depression, loneliness, hopelessness Anxiety Low self-esteem Genetic Inherited predisposition to alcohol or drug dependence Alcoholic parent - 3 to 6 times higher Adult children of alcoholics have abnormal brain cortisol reactions to stress Drugs induce changes in genes (cocaine, FOS B) Low tolerance for stress Other mental health disorders Feelings of desperation Feelings of loss of control over one’s life Feelings of resentment Behavioral Aggressive behavior in childhood Conduct disorder; antisocial personality disorder Avoidance of responsibilities Impulsivity and risk-taking Environment Alienation and rebelliousness; reckless behavior Male gender School-based academic or behavioral problems; school drop-out Inner city or rural residence combined with low Involvement with criminal justice system or illegal activities socioeconomic status; lack of employment Poor interpersonal relationships Opportunities Social Family Use of drugs and alcohol by parents, siblings, spouse Family dysfunction (e. g. , inconsistent discipline, poor parenting skills, lack of positive family rituals and routine) Family trauma (e. g. , death, divorce) Age of first use Alcohol- and drug-using peers Low perception of harm Social or cultural norms approving use Expectations about positive effects of drugs and alcohol Availability of or accessibility to alcohol and drugs

REG FLAGS Physical or sexual abuse Marked change in physical health Parental substance abuse Deteriorating performance in school or job Parental incarceration Dysfunctional family relationships Peer involvement with drugs or alcohol or with serious crime Smoking tobacco Dramatic change in personality, dress, or friends Involvement in serious delinquency or Crimes HIV high-risk activities (e. g. , injection drug use or sex with injection drug user) Serious psychological problems (e. g. , suicidal ideation or severe depression)
 Neocortex (modern man) 1. Survival")
NEOCORTEX LIMBIC SYSTEM REPTILIAN COMPLEX Limbic and Reptilian (beast) Neocortex (modern man) 1. Survival 1. Reasoning and learning 2. Emotions 2. Consciousness 3. Autonomic functions 3. Motor and sensory 4. Reward and appetite 4. Memory 5. Reliable and rigid 5. Language 6. Only able to execute yes 6. Abstract thought 7. Always on 7. Flexible and plastic 8. Able to execute both yes and no 9. Both on and off

Circuits Involved In Drug Abuse and Addiction Inhibitory/ Control PFC – prefrontal cortex ACG – anterior cingulate gyrus; Motivation/ Drive OFC – orbitofrontal cortex SCC – subcallosal cortex Reward/ Saliency NAc – nucleus accumbens VP – ventral pallidum; Memory/ Learning Hipp – hippocampus; Amyg – amygdala All of these brain regions must be considered in developing strategies to effectively treat addiction

Natural Rewards and Dopamine Levels Adapted from: Di. Chiara et at, Neuroscience, 1999 Adapted from Fiorino and Phillips, J Neuroscience, 1997

Normal Pleasure Response nucleus accumbens YUM!! VTR substantia nigra Increased Dopamine Release locus coeruleus Pleasure/Motivation Response

Brain Reward Pathway substantia nigra locus ceruleus Psychoactive Addictive Drugs Act on this Pathway

Brain Reward Pathway Wow!!! substantia nigra locus ceruleus Drug Dopamine surge!!!

Brain Reward Pathway Wow!!! substantia nigra locus ceruleus Drug Dopamine surge!!! Dopamine, Serotonin, Norepinephrine…

Reward Pathway Drugs act on the Brain Reward Pathway The “Wow!!!” is a big reason people take drugs but other things also happen…

Reward Pathway Areas Emotional & behavioral learning Control of body movement Early learning and memory processing Attention states and automatic function

Continued Drug Use Wow!!! substantia nigra locus ceruleus A “molecular switch” is thrown in the brain • Sensitization, Craving and Relapse • Loss of control over drug use • Compulsive drug seeking behavior
 Hijacked!! Euphoric memories Profound changes in neurons and brain circuits Impaired")
Neocortex (modern man) Hijacked!! Euphoric memories Profound changes in neurons and brain circuits Impaired cognitive function Reptilian (beast) DRUG ADDICTION HIJACKED BRAIN Euphoric memories Profound changes in neurons and brain circuits Impaired cognitive function Adaptations in habit or nonconscious memory systems Susceptibility to powerful emotional and environmental cues

The hijacked brain is trapped in a circle of A. B. C. D. E. F. G. Dishonesty Denial Rationalizations Justification Minimization Cravings Guilt and Shame LOSS of CONTROL over taking a substance

Limbic and Reptilian 1. 2. 3. 4. 5. 6. 7. Survival Emotions Autonomic functions Reward and appetite Reliable and rigid Only able to execute yes Always on Neocortex (modern man) 1. 2. 3. 4. 5. 6. 7. 8. 9. Reasoning and learning Consciousness Motor and sensory Memory Language Abstract thought Flexible and plastic Able to execute both yes and no Both on and off Aberrant Dysfunctional Addiction Self –The Disease 1. 2. 3. 4. 5. 6. 7. 8. 9. Survival, distorted definition of survival Hyper-reward, hyper-appetite Manipulates Emotions Autonomic functions Hyper-rigid, hyper-reliable Can access selective memories Selectively accesses motor and sensory, for continued hyper-rewards Unable to say no Always on

Once born, the addiction self, is extremely durable and can affect a person after many years of abstinence, can be present for an entire lifetime. Eric Sprague

Effects of Drugs on Dopamine Levels Adapted from: Di. Chiara and Imperato, Proceedings of the National Academy of Sciences USA, 1988, courtesy of Nora. D Volkow, MD

Effects of Amphetamines on Dopamine Levels Adapted from: Di. Chiara and Imperato, Proceedings of the National Academy of Sciences USA, 1988, courtesy of Nora. D Volkow, MD

Long-term drug exposure impairs brain functioning 1. Release 2 to 10 times more dopamine than natural rewards (eating, sex and social activities) 2. Powerful reward strongly motivates people to take drugs again and again. 3. The brain adjusts - producing less dopamine and reducing the number of receptors that can receive signals 4. The ability to experience ANY pleasure is reduced.

Incentive Salience— Wants/ Cravings Incentive salience is a type of motivation created in the brain because it has developed an association between a certain stimuli and reward. “I want and I want it now!!” In the case of addiction this stimuli will be whatever drug the individual is using. Incentive salience is a far greater incentive than merely liking something.

Incentive Salience – Wants/ Cravings Previously neutral stimuli are assigned incentive salience. Smelling cigarette smoke can trigger a craving for nicotine Drug paraphernalia now trigger drug craving. Driving in or near a neighborhood where drugs were purchased triggers craving Thus, if a person's addiction subsides and the individual subsequently encounters one of these secondary reinforcers, a craving for that drug may reappear.

Prolonged drug use changes the brain in fundamental and long-lasting ways And evidence shows that these changes are both functional and structural.

Dopamine D 2 Receptors are Lower in Addiction Cocaine DADA DA D 2 Receptor Availability DA Meth Alcohol Heroin DA DA DA Reward Circuits Non-Drug Abuser DADA DA DA Reward Circuits Control Addicted Drug Abuser

Safe Limits ALCOHOL Men: no more than 2 day, 14 week or 4 drink tolerance Women and Men/Women over the age of 65: no more than 1 day, 7 week or 3 drink tolerance Illicit Drugs: NO safe limit for use All Tobacco products: NO safe limit for use Prescription Drug misuse/abuse: NO safe limit for use

What is a “Standard Drink”
 /nicotine dependence Or")
What should be treated first? Alcohol/ stimulant / substance abuse (detoxification) /nicotine dependence Or de r o f T Eating Disorder—(weight restoration/ stop behaviors) rea tm en t f or Mood Disorders A du lts Anxiety Disorders (Trauma) ADHD Modified from: Stahl, SM. Essential Psychopharmacology. Cambridge, UK: Cambridge University Press 2013.

Many of my patients just want a pill…. . Sorry, there are no magic pills.

Treatment Setting Medical Detoxification and Stabilization/Inpatient hospitalization Dual-diagnosis hospital inpatient Free-standing Rehabilitation or Residential Partial Hospitalization Temporary recovery or halfway homes Intensive outpatient Outpatient DUI/DWAI/DUID programs

Multiple Therapeutic Approach Neuro-Cognitive Behavioral Therapy Contingency Management Motivational Enhancement Therapy Family Therapy (especially for youth) Individual and Group Psycho Therapy Recreational Therapy Music Therapy Equine Therapy Disease Education Classes Spiritual Therapy Nutritional Therapy 12 Step based programs
 Depot Naltrexone (Vivitrol) Acamprosate (Campral)")
Medications for Recovery from Substances Alcohol: Naltrexone (Re. Via) Depot Naltrexone (Vivitrol) Acamprosate (Campral) Disulfiram (Antabuse) Opiates: Naltrexone(Re. Via) Depot Naltrexone (Vivitrol) Buprenorphine (Subutex) Buprenorphine + Naloxone (Suboxone) Methadone Nicotine: Varenicline (Chantix) Buproprion (Wellbutrin/Zyban) Nicotine-gum, patch, lozenge, inhaler

SUD Treatment – The ARS Approach 1. Stabilization 2. Inspiration 3. Motivation 4. Education 5. Application 6. Innovation 7. Continuation

Stabilization = Detoxification and Initiating Treatment 1. Management of acute withdrawal 2. Craving Stabilization 3. Cessation of drug use 4. Continuing treatment at the appropriate level of care

Stabilization -Detoxification Sedative taper Suboxone Craving Control Naltrexone Suboxone CBT -Pain Control NSAIDS Membrane Stabilizers SNRI’s TCA’s Muscle relaxants Suboxone CBT Psychiatric Care Antidepressants Safe Anxiolytics Mood Stabilizers Antipsychotics Safe insomnia medications CBT

Inspiration Belief Change

Motivation A Confrontational Process – we must confront the barriers to change Develop a nurturing rapport with clients. Induct clients to the partnership of the treatment process. Explore what clients expect and determine discrepancies. Prepare clients so that they know there may be some embarrassing, emotionally awkward, and uncomfortable moments Investigate and resolve barriers to treatment. Increase congruence between intrinsic and extrinsic motivation. Examine and interpret noncompliant behavior in the context of ambivalence and the disease and refocus on the treatment partnership Demonstrate continuing personal concern

Education A Teaching and Discovery Process 1. Disease 2. Themselves 3. Provide them a full tool box (coping skills, MAT, etc) that they fully understand 4. Family

Application A process of engagement and practice Recovery Requires ACTION Knowledge alone is not enough Group therapy Therapeutic community Family therapy Psycho Drama Yoga Meditation Mindfulness therapy

Innovation Individualized treatment Find something that works or create new programs Internet Smart phone Apps Research

Continuation Community Recovery Transition programs to IOP care Sober Living Aftercare programs Alumni Groups Virtual therapy with Apps Long term goals and long term follow-up

Summary Addiction is a chronic DISEASE Substance use is on the rise Addiction is incredibly complex with multiple influencing factors Addiction has significant effects on the brain Treatment is a lifelong process
- Slides: 76