Substance Use 101 SUBSTANCE USE 101 PRESENTED BY

Substance Use 101 SUBSTANCE USE 101 PRESENTED BY ADAM TROSPER PROGRAM COORDINATOR, ADULT SUBSTANCE USE TREATMENT AND RECOVERY SERVICES DBHDID

Agenda �Definition of Addiction �Risk Factors and Characteristics �Treatment Options of Substance Use Disorders �Additional Things to Know

SUD is a Complex Illness …with biological, sociological and psychological components
 Definition of Addiction �“ the harmful or hazardous use")
4 World Health Organization’s (WHO) Definition of Addiction �“ the harmful or hazardous use of psychoactive substances--- a cluster of behavioral, cognitive, and physiologic phenomena that typically include: �A strong desire to take the drug �Difficulties in controlling its use �Persisting in its use despite harmful consequences, �A higher priority given to drug use than to other activities
 Definition of Addiction is a primary, chronic disease")
American Society of Addiction Medicine (ASAM) Definition of Addiction is a primary, chronic disease of brain reward, motivation, memory and related circuitry. Addiction is characterized by: Inability to consistently abstain (Capacity for rational thought is overwhelmed by drug seeking drive) Impairment in behavioral control (Users seek the drug with such intensity that basic human drives for food and safety are overpowered) Craving- “Reward” circuitry in the brain becomes hard wired (neurobiological aspects) Diminished recognition of significant problems with one’s behaviors and interpersonal relationships Dysfunctional emotional response Like other chronic diseases, addiction often involves cycles of relapse and remission. Without treatment or engagement in recovery activities, addiction is progressive and can result in disability or premature death.

Addiction is a Brain Disease Prolonged Use Changes the Brain n “Healthy” Brain “Cocaine Addict” Brain In Fundamental and Lasting Ways
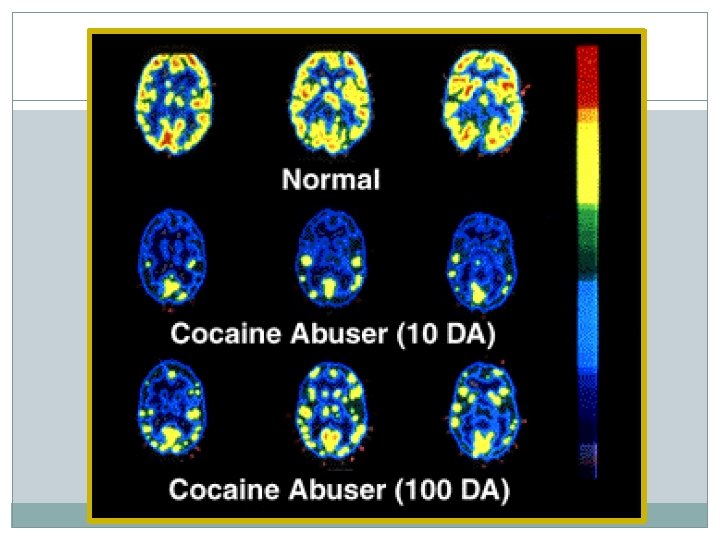

How Drugs Work § Interact with neurochemistry ð Results: - Feel Good – Euphoria/reward - Feel Better – Reduce negative feelings

�All drugs of abuse directly or indirectly target the brain’s reward system by flooding the circuit with dopamine �Dopamine is neurotransmitter present in regions of the brain that regulate movement, emotion, cognition, motivation and feelings of pleasure �Drugs release more dopamine than eating or sex

Brain Reward Pathways

Activation of Reward

Dopamine Spells REWARD Release Recycle Activate
 �Learning Disorders")
SUD Risk Factors �Genetics �Young Age of Onset �Childhood Trauma (violent, sexual) �Learning Disorders (ADD/ADHD) �Mental Illness Depression Bipolar Disorder Psychosis

Critical Period of Brain Development ØThe Brain is not structurally complete at birth. 2 Ø The period after birth is a critical period ØSynaptic connections, where experiences permanently alter brain structure and function myelination, and glial and circulatory support systems all develop after birth 15

Early Experiences can Alter Brain Structure Healthy Brain Deprivation “The Two Year Window” 16

Adversity Impacts Brain Development Ø Permanently alters brain structure and function Ø Lack of stimulation results in pruning away of circuits Ø Lack of social-emotional hardwiring provides weak foundation for later cognitive abilities Ø Repetitive setting off a stress-survival response results in enlargement of the amygdala, smaller hippocampus, and smaller brain Ø Effects last for a lifetime, affecting health as an adult. Institute of Medicine, 2000

18

The Adverse Childhood Experiences When you were growing up, during your first 18 years of life, did you experience: Did you live with anyone who was depressed, mentally ill, or suicidal? • Physical abuse Did you ever see your mother hit, slapped, kicked, punched, or beat up? • Emotional abuse • Sexual abuse • Domestic violence (mother treated violently) • Substance abuse in home • Mental illness in parent • Lost parent due to separation or divorce • Household member in jail Did a parent or adult in the home ever swear at you, insult you, or put you down? [never, once, more than once, don’t know, refused to answer]
 Score Number of individual adverse childhood experiences were summed…… ACE")
Adverse Childhood Experiences (ACE) Score Number of individual adverse childhood experiences were summed…… ACE score Prevalence 0 1 2 3 4 5 6 7 or more 36. 4% 26. 2% 15. 8% 9. 5% 6. 0% 3. 5% 1. 6% 0. 9% 64% reported experiencing one or more 37% reported experiencing two or more One ACE 87% chance of having more than one 20

ACEs Influence Multiple Outcomes Smoking Alcoholism Promiscuity Relationship Problems High perceived stress Married to an Alcoholic Difficulty in job performance Poor Self. Rated Health Hallucinations High Perceived Depression General Health and Obesity Sleep Risk of HIV Disturbances Social Functioning Risk Factors for Mental Common Diseases Health Memory Disturbances Poor Perceived ACEs Illicit Drugs Anxiety Health Panic Reactions IV Drugs Prevalent Sexual Multiple Somatic Health Poor Anger Diseases Symptoms Control Cancer Liver Disease Teen Paternity Fetal Death Skeletal Teen Unintended Chronic Lung Fractures Disease Pregnancy Sexually Early Age of Sexual Dissatisfaction Ischemic Heart Disease Transmitted First Diseases Intercourse
 40 Ace")
ACE Score and Teen Sexual Behaviors 45 Percent with Health Problem (%) 40 Ace Score 0 1 2 3 4 or more 35 30 25 20 15 10 5 0 Intercourse by 15 Teen Pregnancy Teen Paternity Hillis S et al, 2001 22

Relationship Between ACE Score and Early Initiation of Smoking Cigarettes 25 Regular smoking by age 14 Percent (%) 20 15 10 5 0 0 1 2 ACE Score 3 4 >=5 Anda et al. , 1999, JAMA

The ACE Score Alcohol Use and Abuse Percent with alcoho related problem 40 35 30 0 1 2 3 4 or more 25 20 15 10 5 0 Alcoholic Married an Alcoholic Dube SR et al, Adictive Behavior, 2002

Relationship Between Number of ACEs and the Age at Initiation of Illicit Drugs 16 15 -18 Years 14 Percent (%) 12 10 8 6 4 2 0 0 1 2 ACE Score 3 4 ≥ 5 Dube et al. , 2003, Pediatrics

ACE Score and Intravenous Drug Use % Have Injected Drugs 3, 5 3 2, 5 2 1, 5 1 0, 5 0 0 1 2 ACE Score 3 4 or more N = 8, 022 p 0. 001 Dube, 2003, Pediatrics

ACE Score and Chronic Depression as Adult % With a Lifetime History of Depression 70 60 Women – Lighter color Men – Darker color 50 40 30 20 10 0 0 1 2 ACE Score 3 >=4 N = 8, 022 p 0. 001 Dube, 2003, Pediatrics

Relationship Between the ACE Score and Attempting Suicide During Adolescence 16 Attempted suicide < = 18 years 14 Percent (%) 12 10 8 6 4 2 0 0 1 2 3 4 ACE Score 5 6 >=7 Dube et al. , JAMA, 2001

ADVERSE CHILDHOOD EXPERIENCES AND ADULT DISEASE: 54% of depression 58% of suicide attempts 39% of ever smoking 26% of current smoking 65% of alcoholism 50% of drug abuse 78% of IV drug abuse 48% of promiscuity (>50 partners) are attributable to ACE’s. Dr. V. Felitti. 2011

The ACE Study is evidence that…. ADVERSE CHILDHOOD EXPERIENCES are the most basic and long lasting cause of : health risk behaviors, mental illness, Including SUD social malfunction, disease, disability, death, and healthcare costs Dr. V. Felitti. 2011

Seeking to Cope n n n The risk factors/behaviors underlying these adult diseases are actually effective coping devices. What is viewed as a problem by the health care provider is actually a solution to bad experiences for the patient. Dismissing these coping devices as “bad habits” or “self destructive behavior” misses their source of origin. 31

Substance Use and Mental Health Disorders �Managing mental illness is difficult if the client is: USING SUBSTANCES ABUSING SUBSTANCES DEPENDENT ON SUBSTANCES And vice versa

Parallels Between Mental Health Disorders and Substance Abuse � Both are bio-psychosocial illnesses � Both create shame and guilt � Both are stigmatized by society � Both are primary � Both are progressive � Both are chronic � Both are no fault illnesses � People can and do recover from both

Who has Co-occurring mental health and substance use disorders? Dual Diagnosis? �Over 50% of people suffering from schizophrenia, bipolar disorder and other severe mood disorders have a substance use disorder at some time in their life. �About one third of people with anxiety and depressive disorders have a substance use disorder at some time in their life. Mary F. Brunette/Dartmounth 2003

Common Characteristics of Persons Suffering from SUD � Unemployment � Multiple criminal justice contacts � Difficulty coping with stress or anger � Highly influenced by social peer group � Difficulty handling high-risk relapse situations

Common Characteristics… �Emotional and psychological immaturity �Difficulty relating to family �Difficulty sustaining long-term relationship �Educational and vocational deficits

Cognitive Deficits �Memory problems – short-term loss �Impaired abstraction �Perseveration using failed problem-solving strategies �Loss of impulse control �Similar performance to those with brain damage

38 Women Differ From Men: Drug Use · Initiation of drug use · How she obtains her drugs · Where she uses her drugs · How she recovers from drug use Untreated addiction places a woman and her fetus at risk for multiple adverse consequences

39 Drug Injection and Relationships • Women − are less likely to inject drugs than men, although they begin injecting sooner − injecting drugs for the first time are more likely to be introduced to injecting by a sexual partner − are more likely to be involved with a sexual partner who also injects − are more likely to inject with and borrow needles and equipment from their partner, spouse, or boyfriend. − are also likely to begin injecting with groups that are predominantly female Although women may initiate injection through their relationships with injection-drug-using individuals, they are also likely to initiate injection on their own Bryant & Treloar, 2007; Frajzyngier et al. , 2007

40 The Family We Grow Up In Matters ● Drug use disorders co-occur in families ● Major risk factors for drug initiation and substance use disorders among women include chaotic, argumentative, blame-oriented, and violent households Credit: https: //pixabay. com/en/shame-criticism-child-judged-799095/

41 Women’s Partners Matter • Drug-dependent women are more likely than drug-dependent men drugs to have partners who use drugs • Some women continue using alcohol and illicit drugs to have an activity in common with their partners or to maintain the relationships • Although alcohol and marijuana use often begins with peer pressure during adolescence, women are likely to be introduced to cocaine and heroin by men Credit: https: //pixabay. com/en/sunset-kiss-couple-love-romance-691995/

42 Telescoping ● The amount of time between initial use and the development of physiological problems is shorter for women than men ● The amount of time between initial use and the severity of the problems that develop from use of alcohol and drugs is shorter for women than men Greenfield, 1996; Mucha et al. , 2006; Peters et al. , 2003; Credit: http: //pixabay. com/en/spyglass-binoculars-view-lenses-158156/

43 Women and Other Co-Occurring Mental Disorders ● Depression is estimated to co-occur in adults with opioid use disorder at somewhere between 15% and 30% ● Women are more likely than men to have co-occurring drug use and mental disorders ● Women are more likely to have multiple co-morbidity (three or more psychiatric diagnoses, in addition to substance use disorder) than are men ● Research on co-occurring disorders suggests that women who use drugs may be using them to self-medicate distressing affect ● Anxiety disorders and major depressive disorders are the most common cooccurring diagnoses ● Eating disorders and Post-Traumatic Stress Disorder (PTSD), a common reaction following exposure to violence and trauma, also often co-occur in women with drug use disorders Agrawal et al. , 2005; Kessler et al. , 1997; Zilberman et al. 2003

Substance Use Disorder Treatment WHAT IT IS AND HOW IT WORKS

Matching Treatment to Individual’s Needs · No one, single treatment is appropriate for all individuals · Effective treatment attends to multiple needs of the individual, not just his/her drug use · Treatment must address physical, intellectual, social, vocational, environmental, emotional, financial and spiritual problems

Components of Treatment �Assessment �Enhancing motivation �Determining level of care �Treatment planning �Service provision �Progress monitoring and reassessment �Follow-up �Discharge

Determining Level of Care �SUD Professional may use ASAM criteria or other tool �Based on assessment of Medical problems Level of severity of the disorder � Degree of compulsive use � Length of time person has had the illness � Level of use, route of administration � Ability to maintain abstinence on own or with support Co-occurring mental illness History of treatment attempts

ASAM Criteria

The Continuum is Critical

Treatment for Substance Use Disorders/ Continuum of Care �Withdrawal Management �MAT—Medication Assisted Treatment �Inpatient �Residential �Transitional (Long term Residential)/Half-way Houses /Recovery Houses �IOP/Day and Evening �Outpatient �Aftercare and relapse prevention �(Case management) Treatment Resources: http: //dbhdid. ky. gov/Provider. Directory. aspx Treatment Line: 502. 287. 0632

Moving from one level of care to another �Re-occurrence of symptoms is common – don’t be surprised or disappointed! Just be supportive. �Higher severity may require long-term treatment and life-long follow-up �One person may move from one level of care to another, depending on need and response to treatment �Client may need extra support during transition between levels of care
 is a set of interventions aimed at managing acute intoxication and")
Withdrawal Management (detoxification) is a set of interventions aimed at managing acute intoxication and withdrawal. It denotes a clearing of toxins from the body of the patient who is acutely intoxicated and/or dependent on substances of abuse.
 �Medication Assisted Treatment (MAT) is the use of pharmacological medications,")
Medication Assisted Treatment (MAT) �Medication Assisted Treatment (MAT) is the use of pharmacological medications, in combination with counseling and behavioral therapies, to provide a ‘whole patient' approach to the treatment of substance use disorders.

Medication Assisted Treatment Medications are an important element of treatment for many patients, especially when combined with counseling and other behavioral therapies. Alcohol: Opiates: Nicotine: Stimulants: Naltrexone, Disulfiram, Acamprosate, Odansetron Naltrexone, Methadone, Buprenorphine, Vivitrol Nicotine replacement (gum, patches, spray), bupropion [None to date: Research is being conducted but nothing is approved by the FDA]

Inpatient Treatment �For patients with co-occurring physical condition and/or mental illness �Some take Medicaid, some insurance, some self-pay �Length of stay depends on medical necessity �Medical model: Care provided by doctors, nurses, social workers �Education and therapy groups similar to residential treatment

Residential Programs �Residential services includes adult, adolescent, gender specific. �Length of stay based on the individual needs of the client �Care provided by substance abuse professionals, medical professionals and others �Programs are highly structured, including drug and alcohol education, family education, group therapy, individual counseling, support group meetings and discharge planning �Psychiatric interventions if needed �Aftercare services

Outpatient Services �Individual �Group �Family �Intensive Outpatient Programs �Peer Support Services �Case Management Services

Case Management Functions �Engagement �Assessment �Planning, goal setting and implementation �Linkage, Monitoring and advocacy �Disengagement

Case Management Principles �Offers the client a single point of contact with the health and social services systems �Is client-driven and driven by client need �Involves advocacy �Community-based �Pragmatic �Anticipatory �Flexible �Culturally sensitive

Barriers to Treatment and Recovery �Continuum of care may be fragmented, making available services or transition from one level of care to another difficult. �Responsibility for navigating the complex system of care often falls on the client �“Helping” may be viewed as “enabling” to some substance abuse professionals �Program hours or lengths of stay may interfere with child care, employment, housing and other environmental and psychosocial factors

Other Models of Services PREGNANCY CASE MANAGEMENT, RECOVERY MODELS, FAITH BASED INITIATIVES, SMVF AND PILOT PROJECTS.


MAT-PDOA Grant • Medication Assisted Treatment – Prescription Drug • • • and Opioid Abuse Award amount: 1 million dollars per year Length: 3 years Goal: Expand treatment capacity for pregnant and parenting women with opioid use disorder with focus on access to MAT and sustainability Two sites: Bluegrass. org and Cumberland River Behavioral Health Projected to serve 450 clients

Strategy – Future of SUD treatment �Create a new system of care for pregnant and parenting women that is recovery oriented Comprehensive/integrated services Long term, client-centered treatment Evidence based, access to MAT (HBFF COR-12) Multidimensional assessment according to ASAM criteria and placement in the continuum Addresses service deficits and provides wrap around services Cabinet for Health and Family Services
 Behavioral Health Initiative The overall goal of")
Service Members, Veterans and their Families (SMVF) Behavioral Health Initiative The overall goal of the SMVF Behavioral Health Initiative is to strengthen the statewide behavioral health care systems and services for SMVF through ongoing collaboration at the Federal, State and Local levels. SMVF Priorities: 1. 2. 3. 4. Increase access to appropriate and effective behavioral health services for the SMVF population. Maximize quality of services and efficiently allocate resources. Sustain a stable and healthy environment focused on awareness, education, employment and justice. Capture data to support decision-making. Kentucky SMVF Clinical Provider Designation: DBHDID is developing this special designation in order to meet the needs of clinical providers working with the SMVF population in Kentucky. Providers will participate in: Operation Immersion, web-based educational sessions, in-depth behavioral health training including suicide prevention and intervention, and substance use disorders.

This innovative four day training event engages behavioral health and healthcare providers in exploring issues unique to SMVF. DBHDID and the Kentucky Army National Guard have teamed up to present this training. The focus of this program is to allow professionals who work with the military population a chance to experience “Basic Training” and some of the challenges faced by our military today. Providers will also have an opportunity to use virtual reality training simulators that are exclusively used by Service Members to train and prepare for combat. The target population for this training will be behavioral health professionals who treat SMVF, healthcare providers and college students in the respective areas of study. One participant said: “When I left Operation Immersion I truly believe I left a different person than when I came. I understand it was only four days, but it has been one of the most beneficial trainings in my career, I feel it will truly help me in the future. ”

Representatives from federal, military, state and professional organizations across Kentucky unite to host the annual Operation Headed Home (OHH) Conference. This state-wide conference address the needs of SMVF, caregivers, behavioral and medical health professionals with information, resources, and support regarding Traumatic Brain Injury (TBI), Post. Traumatic Stress Disorder (PTSD) and Suicide Prevention. “It is my hope that other states will follow suit with Kentucky and provide the well-deserved and much needed support that Kentucky offers its National Guardsmen. ” Benjamin C. Freakley retired United States Army Lieutenant General
 for")
Drug Courts �Diversion from jail/prison �Non-violent drug-related offenses �Case management and support (leverage) for abstinence from drugs/alcohol �Some provide counseling, most make referrals

OXFORD HOUSE PROGRAM �A democratically run, self-supporting, safe, and drug free living environment for recovering addicts Sharing recovery helps to assure a safe living environment �Can be started by obtaining a Group Home Loan-the funds help pay the first and last month’s rent, deposits for utilities, and items to furnish the homethe members then have two years to repay the loan Must maintain a job, attend weekly support meetings, pay their own portions of expenses, and maintain recovery.

Recovery Kentucky �“In January of 2005, Governor Ernie Fletcher unveiled Recovery Kentucky, an initiative to help Kentuckians recover from substance abuse, which often leads to chronic homelessness. The initiative will create at least ten housing recovery centers across the state” (www. kyhousing. org) � 15 Recovery Centers serving both males and females �The Healing Place in Louisville and the Hope Center in Lexington

Recovery Kentucky �Must meet definition of “homeless” � 1/3 will be referred from corrections �Peer support and peer staff �Recovery Dynamics (12 Step Based) �System of consequences and strong confrontation �Daily living skills training; job responsibilities (on site) and vocational rehabilitation; medical services

Faith Based Programs �May be faith based and licensed treatment providers (check on our website) �May be faith based and unlicensed but with rigorous standards �May not have rigorous standards or other forms of accountability

Faith Based Programs �Variety of programs: Residential Transitional or half-way houses Support services (food, clothing, etc. ) Faith based self-help groups (Celebrate Recovery) Recovery oriented church services Mentoring programs

Self Help § Complements and extends treatment efforts § Most commonly used models include 12 -Step (AA, NA) and Smart Recovery § Most treatment programs encourage self-help participation during/after treatment

Things to know TREATMENT INFORMATION

How Long Should Treatment Last ? Depends on the individual’s needs.

Treatment Effectiveness � Individuals suffering from addiction who participate in drug treatment can: Decrease drug use Decrease criminal activity Increase employment Improve their social and intrapersonal functioning Improve their physical health

But…For How Long? �One Year After Treatment Drug selling fell by nearly 80% Illegal activity decreased by 60% Arrests down by more than 60% Trading sex for money or drugs down by nearly 60% Illicit drug use decreased by 50% Homelessness dropped by 43% and receipt of welfare by 11% Employment increased by 20%

Public Health �Drug treatment is disease prevention �HIV and/or hepatitis infection in injecting drug users

Coercion Treatment does not need to be voluntary to be effective. Court-Ordered Probation Family Pressure Employer Sanctions Medical Consequences

What Is Casey’s Law? An involuntary treatment act in Kentucky for those who suffer from the disease of addiction.

Casey’s Law What does this law provide? This act provides a means of intervening with someone who is unable to recognize his or her need for treatment due to their impairment. What is this law for? This law allows parents, relatives and/or friends to petition the court for treatment on behalf of the person who is substance abuse impaired.

What’s the first step? �The first step is to obtain the petition: From the local District Court Clerk’s Office Or on our website : www. caseyslaw. org

Compounding Issues in Recovery �Socio-economic �Treatment �Single parent �Co-dependency �Ethnic �Employment �Matriarch/ �Domestic violence Patriarch �Gender �Religion �Living situation �Extended family

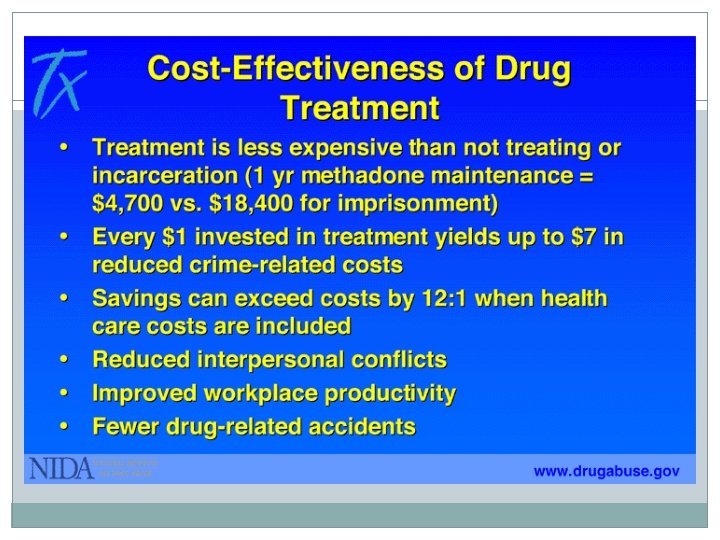
Facts of SUD Treatment �Addiction is a brain disease �Chronic, progressive disorders require multiple strategies and multiple episodes of intervention �Treatment works in the long run �Treatment is cost-effective

Thank You Adam Trosper Program Coordinator Kentucky Division of Behavioral Health Phone: 502. 782. 6230 Email: adam. trosper@ky. gov

Take Home Message
- Slides: 89