Subspecialty Training 2019 Alec Mc Ewan Subspecialist MFM

Subspecialty Training 2019 Alec Mc. Ewan Subspecialist MFM Acting Head of School O&G HEEM

Redrafting the subspecialty curricula • • • Short time frame Subspecialty reps on the subspecialty committee asked to do the work Previous SST Modules redrafted into Capabilities in Practice High level learning outcomes, key skills, descriptors, types of evidence, knowledge criteria Procedures No new skills/competencies to be added Generic non-technical skills to be removed Removing overlap with core Removing redundant skills/competencies Explanatory documents and examples/case studies

Gynae oncology subspecialty modules pre-2019 • • • • • Module 1: General Assessment of a Gynaecological Oncology Patient Module 2: Pre-, Peri- and Postoperative Care Objectives Module 3: Generic Surgical Skills in Gynaecological Oncology Module 4: Ovarian Cancer Module 5 Cancer of the Uterus Module 6: Cancer of the Cervix Module 7: Cancer of the Vulva Module 8: Vaginal Cancer Module 9: Medical Oncology Module 10: Clinical Oncology Module 11: Radiology Module 12: Palliative Care Module 13: Urology Module 14: Colorectal Surgery Module 15: Plastic Surgery and Wound Care Module 16: Gestational Trophoblastic Disease Module 17: Genetic Predisposition to Gynaecological Cancer

Key: Common competency framework competences Medical leadership framework competences Health inequality framework competences Module 5 Cancer of the Uterus Learning outcomes: To understand demonstrate appropriate skills and attitudes in relation to managing a patient with a diagnosis of uterine cancer: - undertake primary surgical management - understand management options to address co-morbidity - manage recurrent disease Page 25 GMC Good Medical Practice (GMP) Domains: Domain 1 : Knowledge, skills and Performance Domain 2: Safety and quality Domain 3: Communication, Partnership and Teamwork. Domain 4: Maintaining Trust Knowledge criteria Aetiological factors leading to endometrial cancer, including obesity, estrogens, genetic predisposition Histological types of endometrial cancer and prognostic implications Preoperative investigation of patients, including radiology, assessment of fitness for surgery Risk of major surgery (surgical and anaesthetic) Preoperative care of patient undergoing major surgery for gynaecological cancer Type of surgery appropriate for endometrial cancer Role of radiotherapy in the treatment of endometrial cancer Inpatient clinical trials Recruitment into clinical trials Risk factors for recurrent disease Patterns of recurrent disease Management options for recurrent disease Rare uterine tumours, e. g. sarcomas GMP Clinical competency 1, 3 Take a history and investigate patients with suspected and proven endometrial cancer Histological diagnosis of endometrial cancer Order and interpret investigations of endometrial cancer (e. g. magnetic resonance imaging) Formulate a management plan Ability to liaise with anaesthesia department To counsel patients regarding diagnosis, management and risks of treatment Perform appropriate surgery including: - Opening and closing midline laparotomy - Laparoscopic assessment of abdominal cavity - Defining ureters and gonadal vessels - Pelvic node dissection/sampling. - Para-aortic node biopsy - Panniculectomy - Salpingo-oophorectomy (bilateral) - Total hysterectomy Recognise and manage intraoperative complications Postoperative care and complications arising FIGO staging of tumour GMP Professional skills and attitudes 1, 2, 3, 4 Ability to take history and investigate appropriately Ability to recognise histological patterns of disease Ability to interpret preoperative investigations and liaise with anaesthetic department Ability to counsel patients regarding treatment options and histology Ability to select and perform appropriate surgical management of endometrial cancer according to patient’s needs Ability to undertake: - Total abdominal hysterectomy and bilateral salpingo-oophorectomy Pelvic node dissection/sampling Para-aortic node biopsy - Laparoscopy-assisted vaginal hysterectomy Ability to manage postoperative care and complications thereof Ability to define FIGO stage of tumour GMP Training support Evidence/assessment 1, 2, 3, 4 Direct supervision from senior colleagues Attendance at multidisciplinary team and pathology department Attendance at multidisciplinary team with radiologist Ward attendance Supervision in operating theatre Intensive care and highdependency unit ward rounds Multidisciplinary team attendance Clinical oncology module Joint clinic attendance Logbook Mini CEX OSATS Multidisciplinary team attendance Laparoscopic skills course Audit of complications

Module 5: Cancer of the Uterus Competence level Not required Level 1 Date Level 2 Signature Date Level 3 Signature Date Understanding of pathology of endometrial cancer Understanding of pathology of uterine sarcoma Counsel patient about surgical management Discuss medical and surgical options Follow-up of treated patient Management of recurrent disease Authorisation of signatures (to be completed by the clinical trainers) Name of clinical trainer (please print) OSATS Major Gynaecological Oncology Procedure Signature of clinical trainer Each OSATS should be successfully completed for Independent Practice on 3 occasions before the module can be signed off Date Signature

Gynae-oncology SST CIPs • CIP 1: The doctor assesses and manages patients with suspected and confirmed gynaecological cancers and those without cancer who are concerned they may develop it. • CIP 2: The doctor plans surgical care and manages problems safely along the entire surgical pathway. • CIP 3: The doctor ensures the patient undergoes a procedure of appropriate radicality for gynaecological malignancy safely, performing it independently or as the leader of a wider surgical effort. • CIP 4: The doctor assesses ovarian cancer and initiates appropriate interventions for all stages and contexts of disease. • CIP 5: The doctor assesses uterine cancer and initiates appropriate interventions for all stages and contexts of disease. • CIP 6: The doctor assesses cervical cancer and initiates appropriate interventions for all stages and contexts of disease. • CIP 7: The doctor recognises, assesses and manages patients with suspected vulval cancer. • CIP 8: The doctor is competent in the assessment of vaginal cancer, performs the practical aspects of its management and assists in the delivery of non-surgical elements of care. • CIP 9: The doctor effectively discusses the role of chemotherapy in the management of gynaecological cancers, both at presentation and in recurrent disease, within the wider multidisciplinary team. • CIP 10: The doctor works within the multidisciplinary team to assess the need for radiotherapy in all gynaecological cancers, initiates appropriate interventions and manages side effects. • CIP 11: The doctor requests and interprets the most appropriate radiological investigations and interventions for gynaecological oncology patients. • Ci. P 12: The doctor assesses and manages the holistic needs of patients with terminal gynaecological malignant disease alongside specialist palliative care services. • Ci. P 13: The doctor understands the impact of gynaecological cancers on the urinary tract and is able to identify, investigate and manage urological complications. • Ci. P 14: The doctor assesses and performs appropriate surgery on the gastrointestinal (GI) tract and manage cases perioperatively. • Ci. P 15: The doctor understands the principles and practice of plastic surgery techniques and wound care as applied to gynaecological oncology and uses these at an appropriate level. • Ci. P 16: The doctor is competent in the assessment and initial management of a patient with suspected and confirmed gestational trophoblastic disease. • Ci. P 17: The doctor diagnoses, investigates and manages patients with a possible genetic predisposition to gynaecological cancer and their families, alongside specialist genetics services.

Ci. P 5: The doctor assesses uterine cancer and initiates appropriate interventions for all stages and contexts of disease. Key Skills Descriptors Assesses uterine cancer • �Stages uterine cancer correctly. • �Counsels patients on diagnosis, surgical options, non-surgical • options, adverse effects of treatment and prognostic factors. • �Maintains good working relationships with referring units and • primary care. • �Provides appropriate surgical management and staging for uterine cancer and provides minimal access surgery where Performs correct surgery for uterine cancer indicated. • �Determines when palliative surgery is appropriate. • �Identifies patients unsuitable for surgery. • �Identifies patients suitable for fertility sparing procedures. • �Recognises and manages intraoperative complications. • �Escalates to other colleagues and specialties (e. g. plastic surgery, • colorectal). • �Communicates effectively with clinical oncology colleagues and counsels patients on the role of radiotherapy in the Manages non-surgical aspects of care management of uterine cancer. • �Counsels on clinical trial entry. • �Communicates discharge information accurately to non-cancer • centre based teams. • �Formulates appropriate follow-up schedules. • �Assesses and arranges management of physical and holistic side • effects of treatment. • �Considers all management options and determine where palliative • or best supportive care options are appropriate.

Evidence to inform the decision • �Cb. D • �Surgical log book • �Evidence of attendance • �GCP training and certificate • �OSATS: o Open/laparoscopic hysterectomy o Open/laparoscopic pelvic lymph node dissection o Open para-aortic lymph node dissection • Mini-CEX • Theatre attendance • �Observation of, assisting and discussion with trainers • �MDT meeting attendance • �Personal study • �BGCS webinars • �Appropriate post graduate surgical • courses • �GCP training • �Direct observation of trainers • �NOTSS • �Reflective practice • �TO 2 (including SO) Knowledge criteria • �The aetiology and presentation patterns of uterine cancer • �The histological types of uterine cancer including endometrial and sarcoma subtypes and the • implications this has on prognosis • �Aetiological factors leading to endometrial cancer, including obesity, estrogens, genetic • predisposition • �Histological types of endometrial cancer and prognostic implication • �Which imaging to request and how to interpret it • �How to plan safe care for patients with morbid and super morbid obesity • �How to lead multidisciplinary team discussions in planning care for uterine cancer cases • �Preoperative investigation of patients, including radiology, assessment of fitness for surgery • �Risk of major surgery (surgical and anaesthetic) • �Preoperative care of patient undergoing major surgery for gynaecological cancer • �Type of surgery appropriate for endometrial cancer • �The role of chemotherapy and radiotherapy in the treatment of uterine cancers • �The risk factors, how to determine if disease has recurred and explain to patients the • management options • �Inpatient clinical trials • �Recruitment into clinical trials • �Rare uterine tumours, e. g. sarcomas • �The physical and holistic impact of uterine cancer treatment

Subspecialty Reproductive Medicine CIPs DEVELOPING THE OBSTETRICIAN & GYNAECOLOGIST: SST-RM PROFESSIONAL IDENTITY: CLINICAL EXPERT Ci. P 1 The doctor is competent in recognising, assessing and managing endocrinological disorders. Ci. P 2 The doctor is competent in providing specialist care for women with endometriosis. Ci. P 3 The doctor has the surgical skills appropriate for a subspecialist in reproductive surgery Ci. P 4 The doctor is competent in recognising, assessing and managing fertility problems and assisted conception. Ci. P 5 The doctor is competent in recognising, assessing and managing complex early pregnancy problems.

Subspecialty Urogynaecology CIPs DEVELOPING THE OBSTETRICIAN & GYNAECOLOGIST - SST-UG PROFESSIONAL IDENTITY: CLINICAL EXPERT Ci. P 1 The doctor has the knowledge, skills and attitudes required for clinical assessment of pelvic floor dysfunction Ci. P 2 The doctor selects and performs appropriate tests and interprets the results Ci. P 3 The doctor is competent in non-surgical management of pelvic floor dysfunction Ci. P 4 The doctor is competent to undertake surgical treatment of pelvic floor disorders
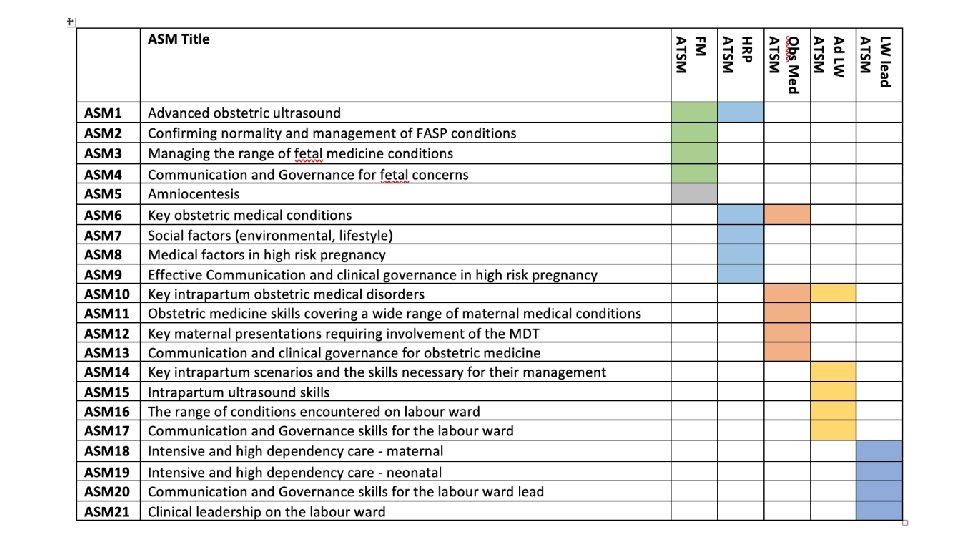
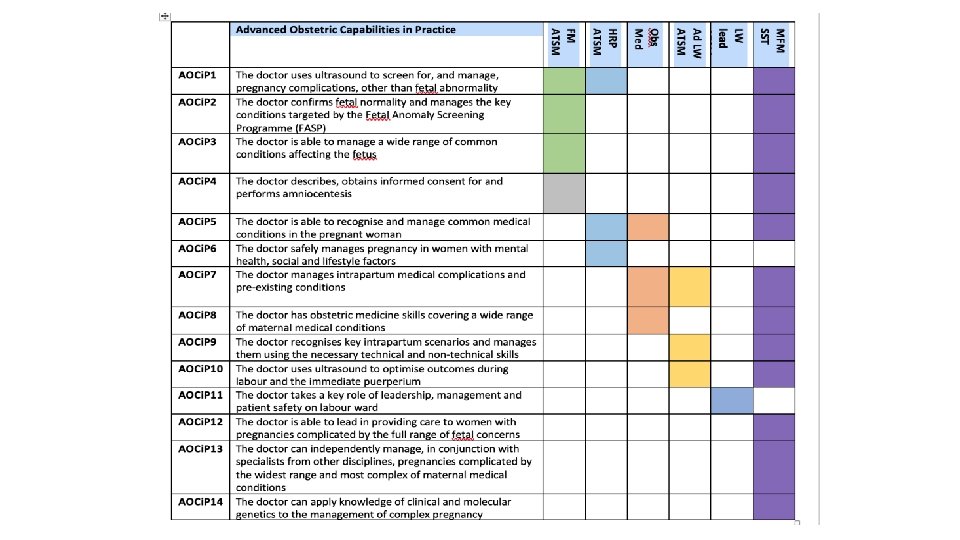
 • • • Module 1 – Maternal medicine")
Maternal and Fetal Medicine SST (pre-2019) • • • Module 1 – Maternal medicine Module 2 – Genetics Module 3 – Fetal Anomalies Module 4 – Antenatal complications Module 5 - Intrapartum care Module 6 – Infection Additional considerations • A third of the competencies in MFM SST were exactly the same as competencies in core and needed sign off by the end of ST 5 • There was a building belief that maternal medicine and fetal medicine SST should be ‘split’
 • Generic Module 1: Communication, team working and leadership skills •")
Non-technical skills (pre-2019) • Generic Module 1: Communication, team working and leadership skills • Generic Module 2: Good Medical Practice and Maintaining Trust • Generic Module 3: Teaching • Generic Module 4: Research • Generic Module 5: Clinical Governance and Risk Management • Generic Module 6: Administration and Service Management • Generic Module 7: Information use and management • Not consistently used and not referred to in the ESR or the subspecialty matrices
 • ST 6/7 trainees on the new core curriculum will be")
Non-technical skills (2019) • ST 6/7 trainees on the new core curriculum will be progressing through the generic core CIPs, and are expected to reach ST 6/7 level for these core CIPs using evidence collected during subspecialty training • ST 6/7 trainees remaining on the old core curriculum, and post CCT subspecialty trainees will be expected to show evidence of advanced progress in the following areas using evidence collected during subspecialty training: Governance and Risk management Teaching Research and Publications Leadership and Management

Assessing the progress of a subspecialty trainee • The CIPs within the subspecialty curricula are all ‘clinical’ • These should be assessed against the entrustability scale 1 -5 • Remember, it is the High Level Learning Outcome (the banner statement) which the trainee and the ES should judge against • Global judgement, not the minutiae • Procedures still need three summative OSATs • No minimal level of evidence: quality, not quantity • Do not forget the generic non-technical skills; the core CIPs 1 -8, 13, 14, OR the list mentioned earlier

Matrix of Progression • Requirements for satisfactory progress at the end of year 1, 2 and possibly 3 • Simple to make a list of what is required by the end of subspecialty training • More difficult to say what is adequate/inadequate progress at assessment points throughout the subspecialty training • Concept of ‘whole time equivalent months of training’ (WTEs) • We need some kind of guidance over what would be expected at the end of 12 months WTE clinical training (ie not including research time)
 • Review")
Transferring onto the 2019 subspecialty curriuclum • MANDATORY (after 31 st October) • Review progress through the ‘old’ modules and decide what entrustability level you feel the trainee is at with the new SST CIPs • All evidence on the old eportfolio will comes as PDF files to the trainee • This does NOT all need to be moved into the new eportfolio, but the trainee may choose to move some of their evidence • The role of the ES at this transfer point
- Slides: 18