Subkingdom Protozoa Phylum Phylum Sarcomastigophor Ciliophora Balantidium Subphylum

Subkingdom: Protozoa Phylum: Phylum : Sarcomastigophor Ciliophora Balantidium ØSubphylum: Sarcodina Amoebas: Entamoeba histolytica Phylum : Apicomplexa • Cryptosporidium • Isospora belli • Plasmodium • Toxoplasma Ø Subphylum: Mastigophora= Flagellates: Giardia lamblia, Trichomonas Leishmania , Trypanosoma

Subphylum: Mastiophora Flagellates protozoa üProtozoa with one or more thread like extension of ectoplasm known as flagella. ü Flagellum, contains an axial structure (axoneme), arising from parabasl body, associated with kinetoplast.
 Lumen – dwelling flagellates: Giardia lamblia, Dientamoeba fragilis, Chilomastix mesnili,")
Subphylum: Mastiophora (Flagellates protozoa) Lumen – dwelling flagellates: Giardia lamblia, Dientamoeba fragilis, Chilomastix mesnili, Trichomonas hominis, Trichomonas tenax Trichomonas vaginalis Flagellate of blood and tissues: (hemoflagellates) 1. Trypanosoma 2. leishmania. Intestinal (oral), (urogenital)
 with world wide distribution. Its life cycle")
Chilomastix mesnili Is a non-pathogenic flagellate (commensal) with world wide distribution. Its life cycle is similar to that of Giardia lamblia. Its trophozoites and cysts found commonly in colon.

Dientamoeba fragilis q. Despite its name, Dientamoeba fragilis is not an ameba but a flagellate. q. This protozoan parasite produces trophozoites only; cysts have not been identified. q. This protozoan commensal in colon and May occasionally produce infection. Infection may be either symptomatic or asymptomatic.
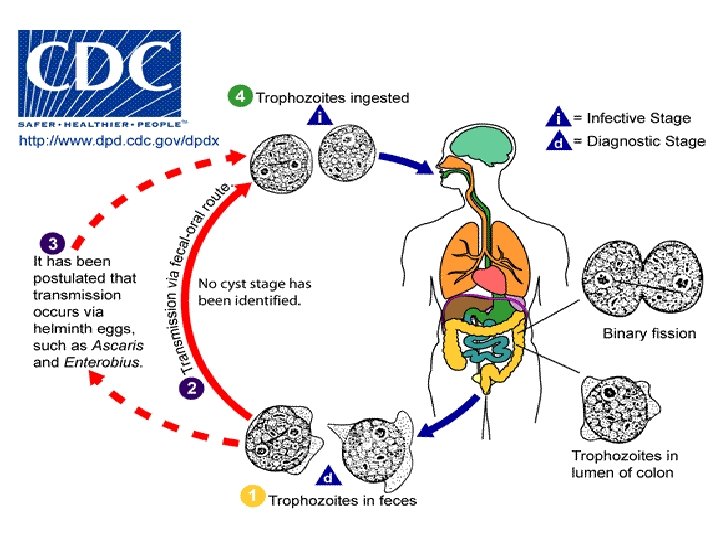

Pathogenesis: Symptoms that have been associated with infection include diarrhea, abdominal pain, anorexia, nausea, vomiting, fatigue, and weight loss. Diagnosis: detection of trophozoites in stool exam. Treatment: Paromomycin, tetracycline or metronidazole.
: (Giardiasis)")
Giardia lamblia (G. intestinalis): (Giardiasis)

q Is a protozoan flagellates q Exists in two morphological forms: 1. a motile vegetative stage, the trophozoite, 2. a cyst stage. q Both of which are seen in small intestine. q This intestinal psrasite common in wild animals (beaver fever)

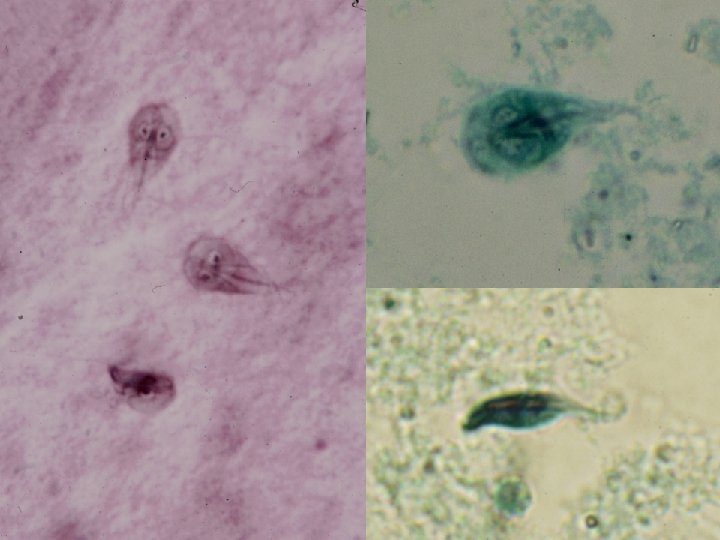
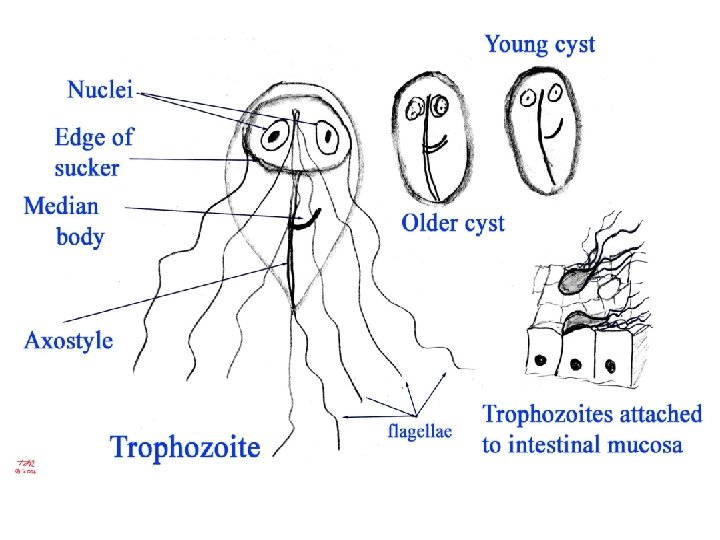
Trophozoites § Pyreform shape § Anterior end broad, posterior end narrow and tapering. §Their dorsal side is convex § 12 -15 x 5 -10 x 2 -4 m § 2 nuclei • large karyosome, no peripheral chromatin
 evident • bilateral symmetry §Pair of claw-shaped median bodies §Adhesive disk")
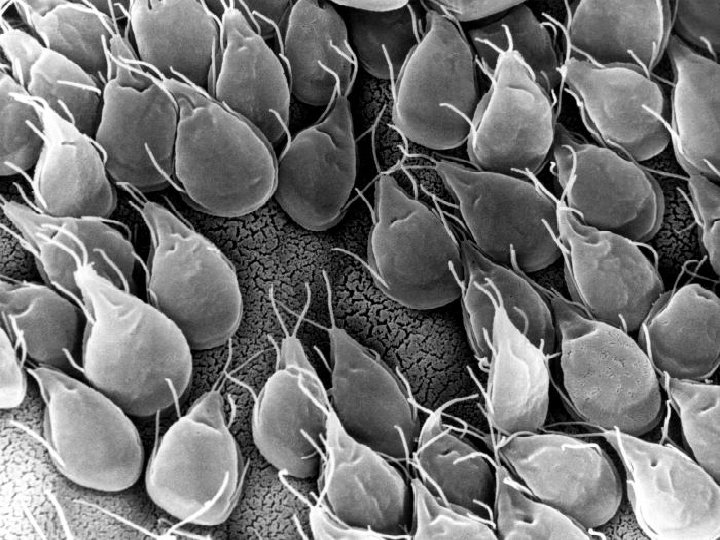
Trophozoites §Fibrils (axonemes) evident • bilateral symmetry §Pair of claw-shaped median bodies §Adhesive disk (not always evident) § 4 pair flagella • motility likened to falling leaf § inhabit the small intestine mucosa

large sucking disk on the anterior ventral side, which serves as the parasite’s method of attachment to the mucosa of the host.

Adhesive Disk = ventral sucking Disk and Attachment

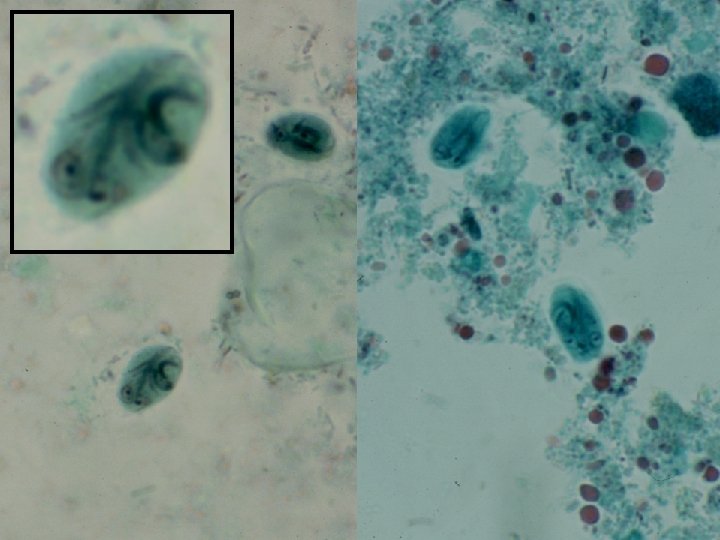
Cysts • Oval shape 11 -14 x 6 -10 m • 4 nuclei at anterior end • large karyosome, no peripheral chromatin • Fibrils (axonemes) evident • Flagella retracted before encystations into stiff curved pairs of parallel fibrils. • Claw-shaped median bodies • Does not destroyed by chlorination of water. • Can survive several months in cold water.

Pavement membrane

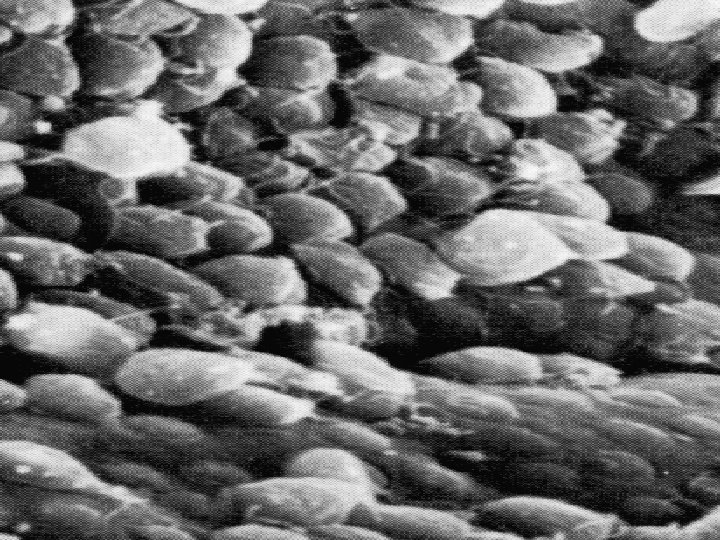
Pathogenesis: • The spectrum varies from asymptomatic carriage to severe diarrhea and malabsorption. • In humans, infection is symptomatic only about 50 %of infected persons. • The trophozoites do not invade tissues, but form pavement-like sheath covering mucosa.

• Therefore the colonization of the gut results in inflammation and villous atrophy, functional derangement of epithelium, reducing the gut's absorptive capability, reduced brush border enzymes and malabsorption.

Villus atrophy and crypt hyperplasia Normal small intestine mucosa

Acute giardiasis v. Develops after an incubation period of 1 to 14 days. v. Symptoms include: • Sudden explosive watery, foulsmelling diarrhea. • The stools are generally describes as loose, bulky, frothy, and/or greasy with no blood or mucous.

• These symptoms accompanied by nausea, colicky epigastric pain, upper gastro-intestinal uneasiness, bloating, flatulence, vomiting, and/or prolonged belching, loss of appetite & weight. • The acute stage usually resolves spontaneously in 3 -4 days.

• Occasionally an acute infection will persists leading to malabsorption, steatorrhea (excessive loss of fat in the feces), debility (loss of strength) and weight loss. • Uptake of bile salts by Giardia inhibits the digestion of fats by pancreatic lipase = steatorrhea

Chronic giardiasis • Characterized by recurrent brief episodes of gastro-intestinal symptoms. • Recurrent diarrhea and malabsorption (particularly of fat and carbohydrates) and debilitation may occur. • Anorexia accompanied by marked weight loss is sometimes associated With chronic infections.

Post-Giardia Lactose Intolerance v. Some patients may present with a lactose intolerance during active Giardia infections which can persist after parasite clearance. v. This clinical manifestation is due to the parasite-induced lactase deficiency and is most common in ethnic groups with a predisposition for lactase deficiency.

v. Lactase is an enzyme that breaks down lactose, a sugar found in milk, to monosaccharides which can be absorbed. v. This lactose intolerance syndrome should be considered in persons who still present mushy stools and excessive gas following treatment, but have no detectable parasites.

Epidemiology: ØCyst infective when passed with feces. ØThe disease transmitted by: § Feco-oral rout. § Direct person to person contact. § Ingestion of contaminated food or water. §Waterborne outbreaks due to contamination of municipal water supplies.

• The infection occurs more frequent in children, in institutions and in large families. • All ages are affected. Infants and young children have an increased susceptibility to giardiasis. • The age-specific prevalence of giardiasis is highest in childhood and adolescence and begins to decline thereafter.

Diagnosis: ØSymptoms, history, epidemiology are used in diagnosis. Giardia caused dysentery is distinct from other dysenteries due to lack of mucus and blood in the stool, lack of increased PMN leukocytes in the stool and lack of high fever. ØStool examination to identifying of cysts or trophozoites in the feces. ØCysts and trophs in the duodenum can be identified microscopically after content has been obtained using a string device (Enterotest).
. The Enterotest consists of a gelatin capsule containing")
The Enterotest (also called 'string test'). The Enterotest consists of a gelatin capsule containing a nylon string of the appropriate length. The free end of the string is taped to the patient's face and the capsule is swallowed. After four hours to overnight the string is retrieved and the bile-stained mucus on the distal portion of the string is scraped off and examined by both wet mount and permanent staining. A small intestinal biopsy, preferably from multiple duodenal and jejunal sites, may also reveal trophozoites attached to the intestinal epithelium.

Treatment: metronidazole and tinidazole. Control: • improve personal hygiene and public sanitation. • Adequate water purification methods.

Trichomonas spp.

ØFlagellated protozoa of the intestinal and urogenital tract, Øpresent in trophozoites stage only (no cyst stage). ØThey are rounded anteriorly and pointed posteriorly. ØThe axostyle arises near the median anterior pole and protroduce from posterior end.

ØFive flagella emerge from a basal body at the anterior pole, Øfour freely extend forwards and Ø one extends backwards, forming the outer edge of the undulating membrane. ØSmall cytostome present in one side of the anterior end; ØSpherical nucleus also present near the anterior pole.

TRICHOMONADS
. a flagellate, is the most important pathogenic")
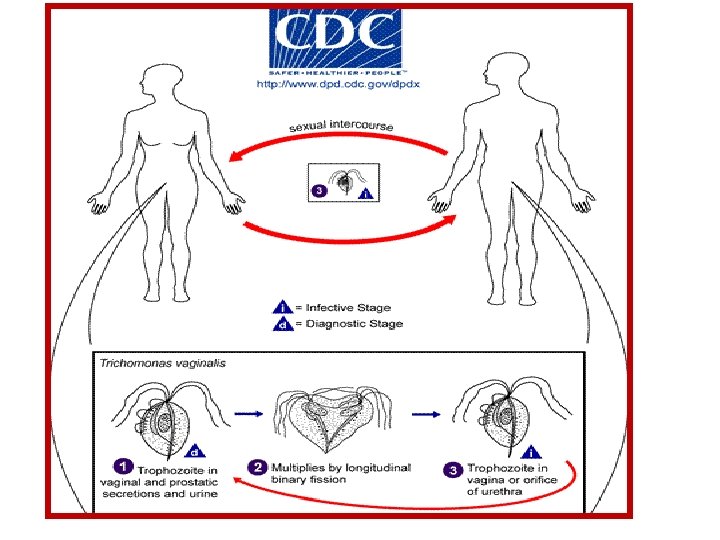
Trichomonas vaginalis (trichomoniasis vaginalis or trichomonas vaginitis). a flagellate, is the most important pathogenic protozoan of human’s venereal disease (i. e. sexual transmitted infections STIs)

Trophozoite: • Pear shaped protozoan • about 10– 20 µm long and 2– 14 µm wide. • The undulating membrane, extending only about half the distance to the posterior end.

Trophozoite: • Jerky non directional motility. • Larger than T. hominis. • Axostyle protrudes well beyond posterior end. • Transmission is by sexual intercourse.

Proportion of asymptomatic trichomoniasis symptomatic 73% 77% asymptomatic Women Men

Pathogenesis: v. Trichomonas vaginalis, despite its name, infects both men and women. v. The incubation period is 5 to 28 days. v. Trichomonas vaginalis infection in women is frequently symptomatic, which includes: ØVaginitis with a purulent frothy discharge (yellowish or greenish) is the main symptom Øvulva and cervical lesions (strawberry cervix)

Frothy discharge and strawberry cervix are classic findings on exam

• itching, burning or pain in the vagina and musty vaginal odor • Abdominal pain, • Dysuria (painful urination) followed by urinating more than usual • Dyspareunia (pain or discomfort during sexual intercourse). • Elevated vaginal p. H, amines

Clinical presentation in men • Urethritis, epididymitis, and prostatitis can occur. • Symptoms include thin, whitish urethral discharge, dysuria (though commonly asymptomatic) • T. vaginalis can be isolated from men with chronic prostatitis

DIAGNOSIS • demonstration of parasite microscopically in: • Vaginal or urethral discharge • urine sediment • Pap Smears are sometimes used to confirm diagnosis

Diagnosis ØThe Papanicolaou test (also called Pap smear, Pap test, cervical smear, or smear test) is a screening test used to detect potentially pre-cancerous and cancerous processes in the endocervical canal of the female reproductive system.

ØThe cells are collected from the outer opening of the cervix of the uterus and the endocervix examined under a microscope to look for abnormalities. ØThe test aims to detect potentially precancerous changes (called cervical intraepithelial neoplasia (CIN) or cervical dysplasia), which are usually caused by sexually transmitted human papillomaviruses.
 and abnormalities in the endocervix")
ØThe test may also detect infections (such as trichomoniasis) and abnormalities in the endocervix and endometrium.
 Control: • Personal hygiene. • Treating of infected persons. •")
TREATMENT • metronidazole (Flagyl) Control: • Personal hygiene. • Treating of infected persons. • Avoiding of coitus with infected partner.
- Slides: 52