Subcutaneous Mycoses These are caused by fungi that

Subcutaneous Mycoses

These are caused by fungi that grow in soil and on vegetation and are introduced into subcutaneous tissue through trauma.

Subcutaneous Mycoses 1. Mycetoma 2. Chromoblastomycosis 3. Phaeohyphomycosis 4. Sporotrichosis 5. Lobomycosis 6. Rhinosporidiosis
 • Post-traumatic chronic infection of subcutaneous tissue. • Characterized by draining")
MYCETOMA (Maduromycosis=Madura foot) • Post-traumatic chronic infection of subcutaneous tissue. • Characterized by draining sinuses, granules and tumefaction. • Caused by a number of different fungi and actinomycetes. • First case seen in Madura region of India.

Distribution • World-wide • Most common in bare-footed populations living in tropical or subtropical regions

• Source of infection: soil • Mode of infection : trauma • Infection is acquired following trauma to the skin by plant materials from trees, shrubs or vegetation debris. • More seen in rural areas (in farmers, walking bare-foot in agricultural land or city parks).

• Feet are the most common site for infection and account for at least two-thirds of cases. • Other sites include the lower legs, hands, head, neck, chest, shoulder and arms.
 • Actinomyces (Actinomycetoma)")
Causative agents • Saprophytic fungi (Eumycetoma) • Actinomyces (Actinomycetoma)

Eumycetoma • • • Madurella mycetomatis Pseudallescheria boydii Acremonium Exophiala jeanselmei Leptosphaeria
: Feet, lower extremities, hands Findings: Abscess formation, draining sinuses containing granules")
Clinical findings Site(s): Feet, lower extremities, hands Findings: Abscess formation, draining sinuses containing granules Deformities Dissemination: Muscles and bones

• Most cases start out as a small hard painless nodule which over time ulcerate to discharge a viscous, purulent fluid containing grains. • Spread to surrounding area. • Spares nerve and tendons.

361







Diagnosis • Clinical findings : – Triad- tumefaction, multiple discharging sinuses, granules. • Characteristics of the granules

Laboratory diagnosis: Clinical specimen: • Tissue biopsy or excised sinus • Serosanguinous fluid containing the granules Methods: 1. Macroscopic examination of the granule • 0. 5 – 2 mm diameter • Bacterial- white granule (rarely red) • Eumycetoma- black or white

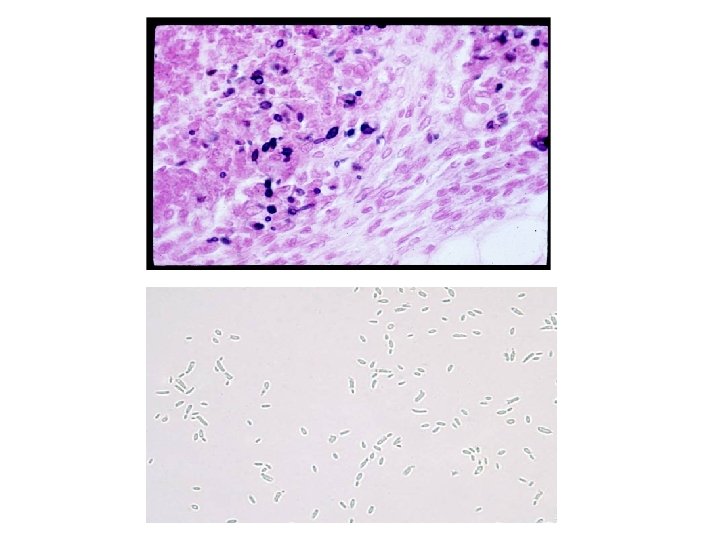
2. Direct Microscopy • Serosanguinous fluid containing the granules examined using either 10% KOH and Parker ink or calcofluor white mounts. • Tissue sections stained using H&E, PAS digest, and Grocott's methenamine silver (GMS).

Tissue section showing blacked grained eumycotic mycetoma caused by Madurella mycetomatis

367

3. Culture Media used: SDA

Pseudallescheria boydii

M. mycetomatis 369

Treatment: Combining miconazole and surgery may prove useful in effectively treating the disease.

Sporotrichosis • Primarily a chronic mycotic infection of the cutaneous or subcutaneous tissues and adjacent lymphatics characterized by nodular lesions which may suppurate and ulcerate. • Infections are caused by the traumatic implantation of the fungus into the skin, or very rarely, by inhalation into the lungs. • First case presented with the clinical picture of sporotrichosis was recorded by Schenck in 1898 from Johns Hopkins Hospital.

• Etiologic agent - Sporothrix schenckii ØThis fungus is a dimorphic fungus. ØAt room 25 degree, it grows as a mold producing branching septate hyphae + conidia & in tissues or at 37 degree, it grows as small budding yeast cells. Ø This fungus lives on plants, grass, trees and rose thorns.

Ø…. . Rose gardener’s disease Sporothrix schenkii infects the body by; Traumatic inoculation Lymphocutaneous sporotrichosis Fixed cutaneous sporotrichosis Rarely, inhalation Pulmonar y lesion

• Fungus enters through scratches from thorns or splinters, cuts while handling potting soil, sphagnum moss, or grass • Distribution: World-wide particularly tropical and temperate regions. • In India, it is prevalent in sub-Himalayan areas.

Ø The conidia or hyphal fragments are introduced into the skin by traumatic inoculation usually by rose thorns. Pathogenesis Ø So, this disease is an occupational risk to gardeners and agricultural workers.

Clinical types • • • Lymphocutaneous sporotrichosis Fixed cutaneous sporotrichosis Mucocutaneous sporotrichosis Disseminated sporotrichosis Pulmonary sporotrichosis

• The first sign of disease is the appearance of a small, hard, nontender subcutaneous nodule. • As the disease progresses – involves adjacent lymphatics. Nodulo-ulcerative secondary lesions • Lymphocutaneous sporotrichoisis - 75% of all cases.

• Secondary spread to articular surfaces, bone and muscle is not infrequent, and the infection may also occasionally involve the central nervous system, lungs or genitourinary tract. • Granulomatous raection + pyogenic.

Ø The initial lesion is a granulomatous nodule that will ulcerate and become necrotic. Ø Multiple subcutaneous nodules occur along the lymphatic vessels.

Ø In endemic areas such as Mexico, South Africa and Japan, population has some immunity to sporothrix so they develop fixed cutaneous sporotrichosis in which the patient has only single non lymphatic nodule which is limited and non progressive.

433

434



437

Lab -diagnosis Specimen: • Biopsy • Exudate from the lesion

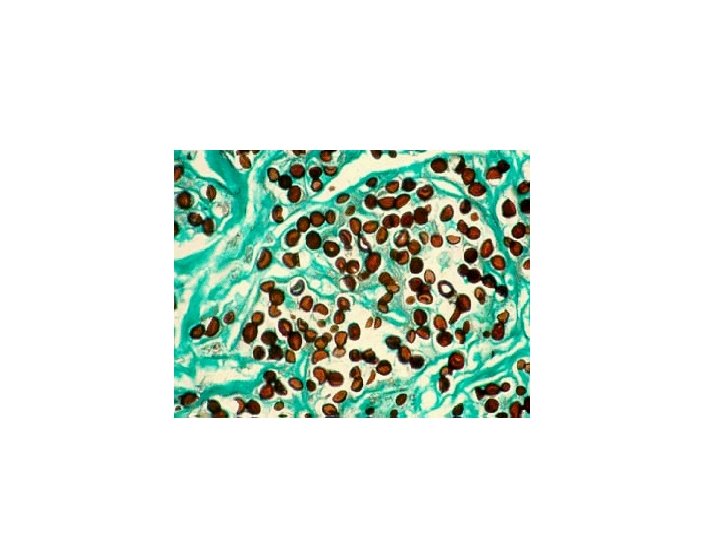
Methods Labo. Lab-ratry diagnosis q Direct microscopic examination: ü Yeasts are seen in tissue sections stained with Gomori methenamine silver which stain cells black or periodic acid Schiff which stain cells red. ü Yeast cells are round, fusiform or cigar shaped (1 -3 X 3 -10 µm).
.")
Budding yeast often irregularly-shaped to broadly elliptical (cigar bodies).

438

441

Another structure termed asteriod body is often seen especially in endemic areas. In H&E sections, asteriod body is a central basophilic yeast cell surrounded by eosinophilic radiating extensions which are Ag/Ab complexes

• Fungus is diphasic, and will convert from a filamentous phase to a yeast phase when grown at a higher temperature (37°C). • Filamentous phase is hyaline, and produces delicate conidiophores and conidia.

q Culture: ü It is the most reliable method of diagnosis of sporotrichosis. ü Culture is done on SDA with antibiotics at 25 degree (colonies are black and shiny then become wrinkled and fuzzy with age).


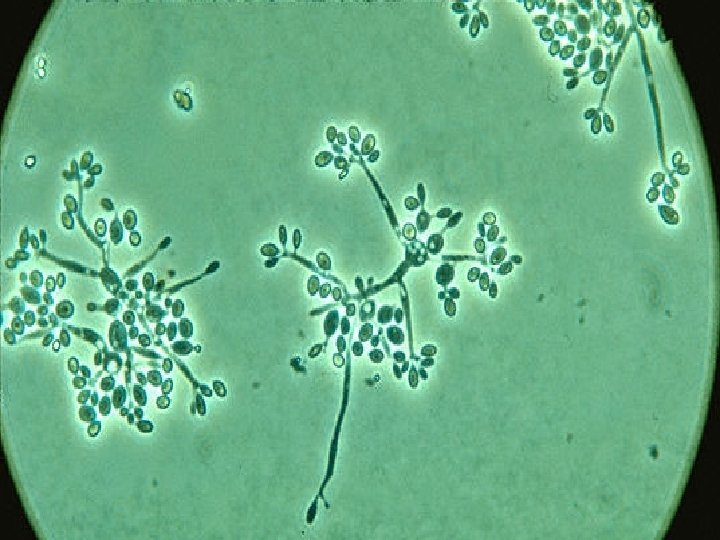
ü Under the microscope: hyphae are seen bearing clusters of oval conidia (2 – 4 µm) at the tip of slender conidiophore resembling daisy. -- Flower like pattern ü If the plate is incubated at 37 degree, it will convert to a yeast culture. q Serology: latex agglutination test.

440

Treatment • Oral potassium iodide in milk. • Itraconazole. • Amphotericin B in systemic infections.

Lobomycosis or Lobo disease • Caused by Loboa loboi (yeast-like organism that has never been cultured) • Disease is chronic, localized, subepidermal infection characterized by the presence of keloidal, verrucoid, nodular lesions • • Frst describe in patient known as Jorge Lobo Found in humans and dolphins. Chains of yeast cells form in tissue Common in Amazon natives

Phaeohyphomycosis • Characterized by the presence of brown pigmented fungal elements caused by a number of different fungal species • The fungi are usually pigmented dark brown to hyaline • In rare instances infections may become invasive systemic (invading various organs) and/or cerebral. • Distribution: World-wide

Cutaneous phaeohyphomycosis of the forearm caused by Exophiala jeanselmei. Cutaneous phaeohyphomycosis of the face caused by Wangiella dermatitidis.

Aetiological Agents: Various dematiaceous hyphomycetes ; • Cladophialophora bantiana • Curvularia sp. • Wangiella dermatitidis • Bipolaris sp. • Alternaria sp. • Exophiala jeanselmei.

Exophiala moniliae Wangiella dermatitidis

Cladophialophora bantiana Bipolaris australiensis Cladosporium cladosporioides Aureobasidium pullulans

• In diagnosis, materials from cysts, nodules, abscesses and other infected tissues may be examined under the microscope directly with 10% KOH. The fungi are usually pigmented dark brown to hyaline. • Treatment usually involves surgical excision of fungus and treatment with antifungal drugs (amphotericin B, 5 -fluorocytosine, ketoconazole, or another imidazole).

Chromoblastomycosis chromomycosis or verrucous dermatitis • Slowly progressive granulomatous infection, characterized by the formation of verrucoid (rough), warty, cutaneous nodules, which may be raised 1 -3 cm above the skin surface. The roughened, irregular, pedunculated vegetations often resembles the florets of cauliflower. • Found primarily in the tropics or subtropics

Aetiological Agents: • Fonsecaea pedrosoi • Phialophora verrucosa (identical to Cladophora americana which causes bluing of lumber) • These fungi are collectively dematiaceous fungi, because their conidia or hyphae are darkcolored, either gray or black.

• Soil-inhabiting fungi • Common in tropics or subtropics • Fungi found growing on plant debris, wood, soil. • Susceptibility enhanced by going barefoot or wearing sandals • Found almost exclusively in laborers • Enters hand or feet after trauma

Chromoblastomycosis

• Red or violet color on skin may resemble a ringworm lesion • Develops into a verrucous lesion • Pruritus (itchiness) and papules may develop • Fungus gets under the skin (produces bumps) • Bumps may block lymphatic system and cause elephantiasis

• Sometimes bacterial infection may enter and cause a secondary infection • Rarely this fungus spreads to other areas of the subcutaneous tissue. • Potentially may spread to brain (lifethreatening in that case)

Laboratory diagnosis • Microscopy • Culture Specimen: Biopsy tissue – Hematoxylin stain - look for fungal cells scattered among skin cells – Colonies of fungi are dark or blackish

– Two species implicated in this mycosis - each may produce several spore types • Fonsecaea pedrosoi - Cladosporium type and Rhinocladiella type of conidiation • Phialalophora verrucosa - Phialophora type (flowers in the vase conidiation)

Fonsecaea spp.

Phialophora spp.

• Treatment – Usually not fatal or necessarily painful – No really good cure – Surgical excision, electrodesiccation, or cryosurgery are useful in early stages of disease – Thiabendazole - shows promise (given orally and on skin mixed with dimethyl sulfoxide [DMSO] - to deliver drug) - experimental drug – Itraconazole shows promise in clinical trials.

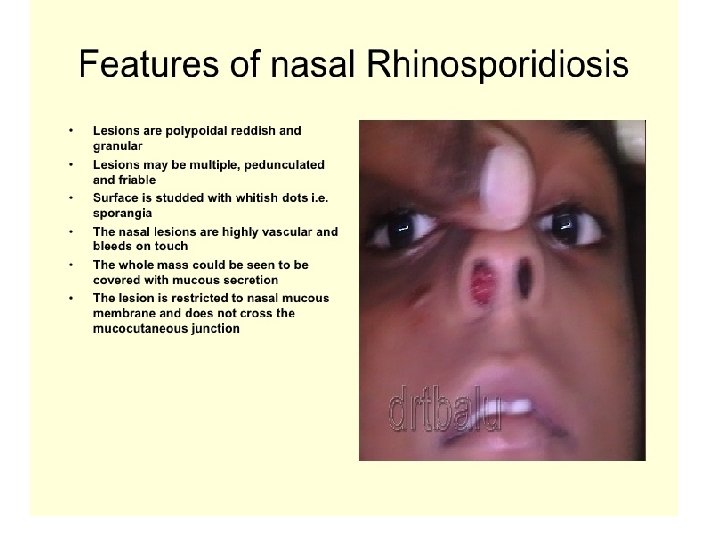
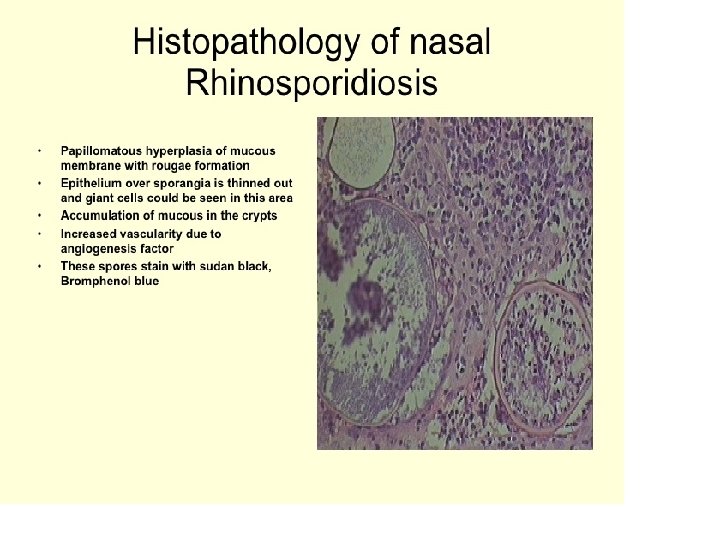
Rhinosporidiosis • A chronic granulomatous disease characterised by the production of large polyps, tumours, papillomas, or wart-like lesions. • It is an infection of the mucocutaneous tissue. • The nose is the most commonly affected site caused by Rhinosporidium seeberi

• Causative agent: Rhinosporidium seeberi yet unisolated and unclassified fungus. • Common in India, Ceylon, the Middle East • Males account for 70 -90% of cases • Eye infections seem to be more common in women • Nasal, ocular, and other mucocutaneous regions may show signs of disease manifested as polyps and tumors

• In tissue, the fungus produces spherules that possess a thick wall; endospores are contained within.

431

Treatment: Surgery Dapsone
- Slides: 82