SubacuteChronic meningitis Reat ZARAS MD Prof Infection Dept

Subacute/Chronic meningitis Reşat ÖZARAS, MD, Prof. Infection Dept. rozaras@yahoo. com
 Subacute (1 week-1 mo. ) Chronic (> 1 mo.")
Admission Acute (1 day-1 week) Subacute (1 week-1 mo. ) Chronic (> 1 mo. )

Subacute/Chronic meningitis • Within weeks or months • Headache, fever, neck rigidity, mental changes • Focal neurological signs are more frequent • Needs specific treatment • A diagnostic challenge

A Case Study • A 48 -year-old female was admitted with headache, myalgia, nausea, vomiting, fatigue, anorexia and fever for 6 weeks • Biochemistry normal • CBC normal • C-RP: 5 Xnormal, ESR 100 mm/h

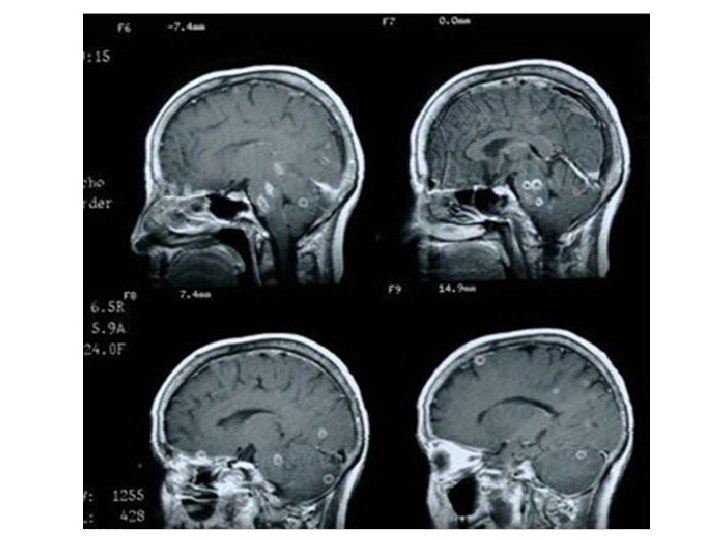
• No previous and family history – Immunosuppressive disorders/drugs – No similar signs & symptoms in the family • No focal neurological sign • Neck rigidity +/-, Kernig and Brudzinski + • MRI showed mild contrast enhancement at basal cranial meninges

CSF • • • Clear Cell count: 250 /mm 3, 80% lymphocytes Glucose 10 mg/dl (blood glucose 98) Protein 280 mg/L Gram and EZN staining: negative

• What is your diagnosis?

2 days later • CSF TB-PCR: positive

25 days later • CSF cultures Mycobacterium tuberculosis

Subacute/chronic meningitis • Infections: – TB
, immune suppression • Prodrome")
TB • May follow a slow progress • Exposure, TST/PPD(+), immune suppression • Prodrome 2 -4 weeks
 – – Fever")
• Not only menengitis, • Vasculitis, space-occupying lesion (brain tuberculoma) – – Fever Change in mental status Hemiplegia, paraplegia Ocular nerve involvement
 Cell Type Glucose(Mg/d. L) Viral 50– 1000 Lymphocytic >45 <200")
CSF Etiology WBC(/mm 3) Cell Type Glucose(Mg/d. L) Viral 50– 1000 Lymphocytic >45 <200 Bacterial 1000– 5000 Neutropilic 100– 500 TB 50– 300 Lymphocytic <45 <40 Protein(Mg/d. L) 50– 300

neuropathology. neoucom. edu

Clinical Presentation • Most common clinical findings: – Fever – Headache – Vomiting – Nuchal Rigidity

Diagnosis • CSF Examination – Usually lymphocytic pleocytosis – Elevated protein with severely depressed glucose – AFB – Culture – PCR

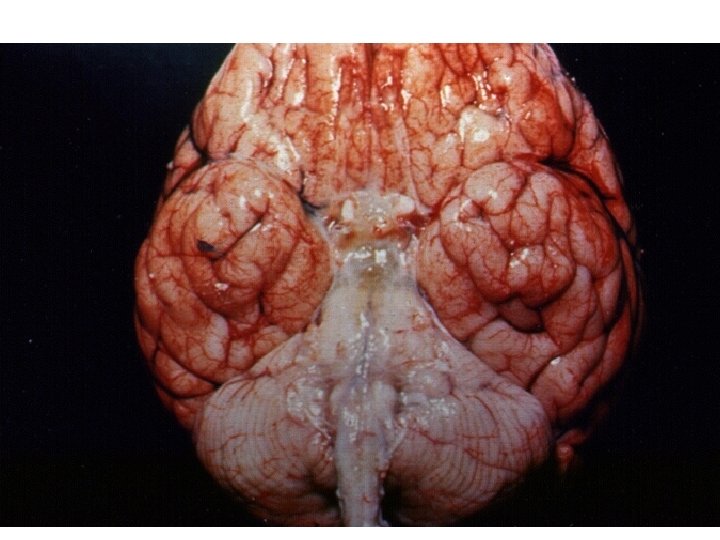
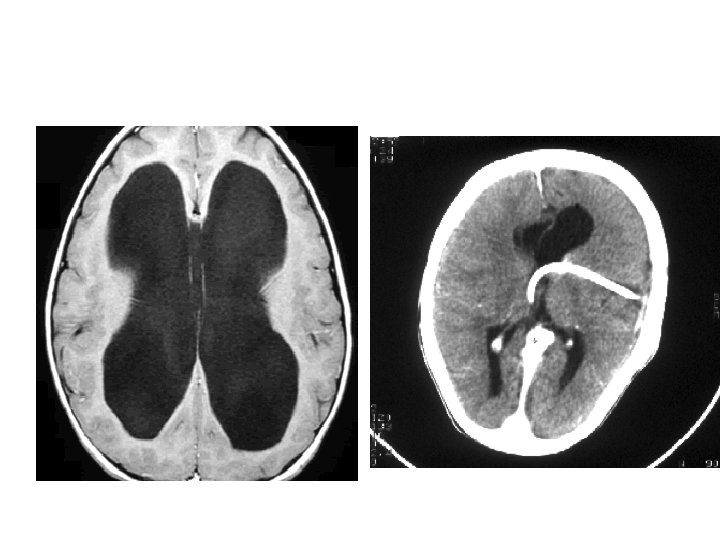
Diagnosis • Other Studies – Brain imaging – demonstrates hydrocephalus, basilar exudates and inflammation, tuberculoma, cerebral edema, cerebral infarction • CXR – Abnormal, sometimes miliary pattern

seattlechildren. org

Treatment: Antimicrobial Therapy • Start as soon as there is suspicion for TB meningitis • Same Guidelines as those for pulmonary TB – Intensive Phase: 4 drug regimen of Isoniazid, Rifampin, Pyrazinamide, and Ethambutol for 2 months – Continuation Phase: Isoniazid and Rifampin for another 7 – 10 months

Treatment: Adjunctive Therapy • Glucocorticoids Indicated with: – rapid progression from one stage to the next – CT evidence of cerebral edema – worsening clinical signs after starting anti. Tb meds – increased basilar enhancement, or moderate to advancing hydrocephalus on head CT

Outcomes • Overall Poor • Only 1/3 - 1/2 of patients demonstrate complete neurologic recovery • Up to 1/3 of patients have residual severe neurologic deficits such as hemiparesis, blindness, seizure DO

Another Case Study • A 30 -year-old male farmer was admitted with headache, newly-onset seizures, and fever for 1 month • Biochemistry normal • CBC normal • C-RP: 5 Xnormal, ESR 50 mm/h

A 30 -year-old male was admitted with headache, newly -onset seizures, and fever for 1 month… • Blood cultures were obtained • MRI: normal • Diagnosed by a serology!. . .

• Rose-Bengal test positive • Wright test positive • 2 bottles of blood culture yielded Brucella melitensis

Rx • Rifampin+Doxycycline
 – Brucellosis")
Subacute/chronic meningitis • Infections: – TB – Spirochetal diseases (syphilis, Lyme’s disease) – Brucellosis – Fungal • Cryptococcus neoformans, Aspergillus, Candida Toxoplasmosis,

Neurosyphilis • Infection of the central nervous system by Treponema pallidum • Neurosyphilis can occur at any time after initial infection.

utdol. com

• Early NS – Asymptomatic – Symptomatic – Meningovascular • Late NS – General paresis – Tabes dorsalis
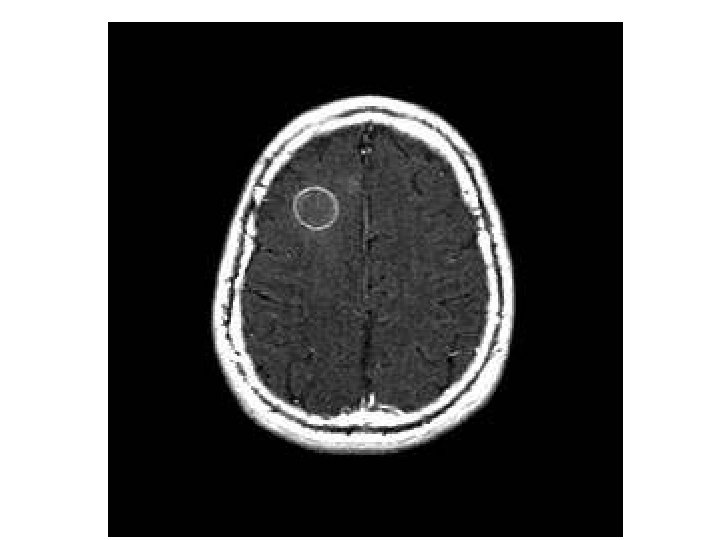
 Focal meningeal enhancement B) Significant edema in the left frontal lobe with left")
A) Focal meningeal enhancement B) Significant edema in the left frontal lobe with left posterior frontal lobe. surrounding edema. Cerebral gumma in an HIV-infected patient with recent secondary syphilis. utdol. com

Diagnosis • EIA: syphilis enzyme immunoassay • FTA-ABS: fluorescent treponemal antibody-absorbed test • TPPA: Treponema pallidum particle agglutination test

Rx • Penicillin G benzathine 2. 4 million units IM once
- Slides: 36