Structural Heart Valve Intervention Sunday February 21 2010

Structural Heart & Valve Intervention - Sunday, February 21, 2010 Percutaneous Edge-to-Edge Evalve Mitral Valve Repair for Functional MR James Hermiller, MD, FACC, FSCAI St Vincent Hospital, Indianapoli, IN

DISCLOSURES James Hermiller, MD • Consulting Fees – Abbott Vascular, Boston Scientific Corporation, St. Jude Medical

Background • Of the over 250, 000 patients in the United States developing significant mitral regurgitation (MR) each year, up to 60% have functional MR • Functional mitral regurgitation results from ventricular remodeling with apical/posterior displacement of one or both papillary muscles, tethering the chordae, which in combination with LV dysfunction causes mal-coaptation of the leaflets

EVEREST I & II Enrollment as of September 15, 2009 Enrollment Population n EVEREST I Feasibility (completed) Registry patients 55 23 Patients from Phase I and EVEREST II Roll-in roll-in from Phase II with FMR Randomized n=279 Randomized Clip (100% enrolled) Randomized Surgery 60 184 95 EVEREST II 46 Patients from. High. HRR with FMR Risk Registry (100% enrolled) EVEREST II REALISM Registry patients Continued Access Registry (enrolling) (non HRR and HRR) Total enrolled 78 135 591

Methods: Anatomic Eligibility • Ischemic or non-ischemic etiology – Absence of degenerative valve disease on TEE • Sufficient leaflet tissue available for mechanical coaptation – > 2 mm “vertical” leaflet tissue available • Absence of severe LV dysfunction – Excluding LVID-s > 55 mm or EF <25% (HRR: >60 mm; <20%)
 Improved 17% (2/12) No")
EVEREST Preliminary FMR Cohort: NYHA Class- APS Patients 75% (9/12) Improved 17% (2/12) No Change 8% (1/12) Worsened w/o MR > 1+

EVEREST Preliminary FMR Cohort Reverse LV Remodeling p = 0. 006 p < 0. 04 p < 0. 03 p = 0. 12 Diastolic Systolic

EVEREST Preliminary FMR Cohort: Freedom From Death and MV Surgery Kaplan-Meier, APS Patients -- N = 19 100% Probability of Event Free Clinical Success 100% 95% 84% 80% 84% 84% 84% 78% 60% 40% (19) (18) (12) (8) (5) (n = reached endpoint) (0) (0) (4) (9) (12) (n = patients At Risk) 20% Freedom From Death and MV Surgery 0% 0 6 12 18 Time (months) 24 30 36 42

EVEREST Preliminary FMR Cohort: Freedom From MR > 2+ Kaplan-Meier, Probability of Event Free Clinical Success 100% 84% 80% 79% 79% 60% 40% (19) (18) (16) (12) (8) (5) (n = reached endpoint) (0) (0) (2) (7) (9) (n = patients At Risk) 20% Freedom from MR > 2+ 0% 0 6 12 18 24 Time (months) 30 36 42

EVEREST II HRR: Study Algorithm KEY INCLUSION CRITERIA • Predicted procedural mortality risk >12% (STS calculated or Surgeon estimated based on pre-specified comorbidities) • Symptomatic 3+ or 4+ MR • Degenerative or Functional KEY EXCLUSION CRITERIA • EF ≤ 20% and/or LVESD >60 mm • MVA <4 cm 2 • Leaflet anatomy unsuitable for Mitra. Clip device 78 Enrolled FMR N=46 (59%) DMR/Mixed N=32 (41%)
 Mitra. Clip therapy results in sustained MR reduction 18%")
HRR FMR: Mitral Regurgitation (ITT) Mitra. Clip therapy results in sustained MR reduction 18% 26% Moderate-Severe or Severe MR (Grade 3+/4+) 97% 82% 74% Mild-Moderate MR (Grade 1+/2+) 52% of patients had MR grade < 2 at 12 months 3% n=34, Matched Data

HRR and FMR: LV Volume Mitra. Clip therapy results in reverse LV remodeling P<0. 0001 n=34 12 month Matched data P=0. 0002 192 153 Diastolic LVEDV Baseline LVEDV 12 Months 103 87 Systolic LVESV Baseline LVESV 12 Months
 Non-randomized 55 EVEREST II (Pivotal)")
Mitra. Clip Experience Study Population n EVEREST I (Feasibility) Non-randomized 55 EVEREST II (Pivotal) Pre-randomization 60 EVEREST II (Pivotal) Non-randomized patients (High Risk Registry) 78 EVEREST II (Pivotal) Randomized patients (2: 1 Clip to Surgery) REALISM (Continued Access) Patients 255 EUROPE Commercial Patients 442 Total *Data as of 2/5/2010. Source: Queue emails, EU Case Observation Reports, US REALISM Case Observation Reports. 279 184 Clip 95 Surgery 1, 074 +95 surgery

Worldwide Experience Comparison* Europe* REALISM* Patient Treated 442 244 Hospitals/Sites 31 35 Etiology: FMR/DMR/Mixed (%) 68%/25%/7% 60%/33%/6% Average Device Time (hr) 1: 52 Clip Implant Rate (%) 95% 1 Clip/2 Clip/3 Clip/4 Clip (%) 70%/29%/1%/<1% 64%/36% Site Reported MR Reduction (%) 98% 100% Clip Embolization (%) 0% 0% *Data as of 2/5/2010. Source: Queue emails, EU Case Observation Reports, US REALISM Case Observation Reports.

Case Example • 78 year old woman status post 4 V CABG 10 years prior to admission • FC IV CHF - refractory symptoms • LHC revealed widely patent grafts

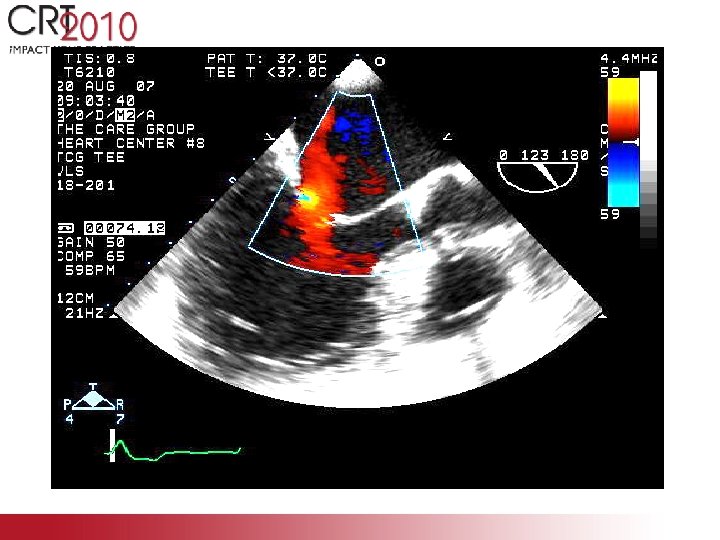
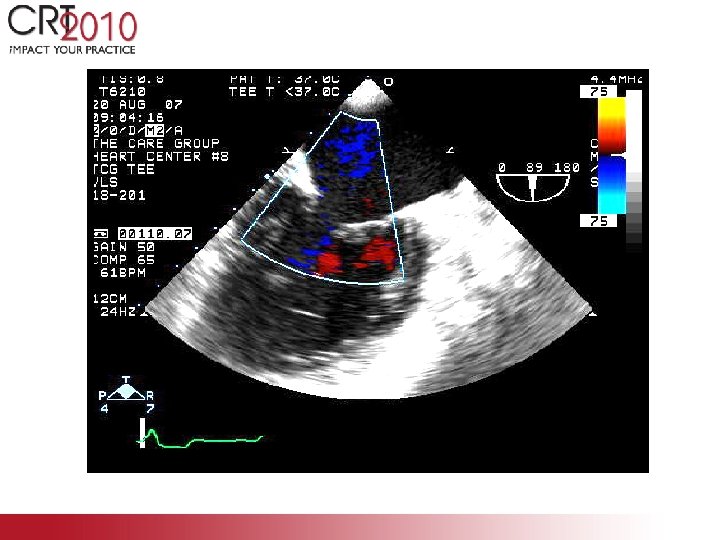

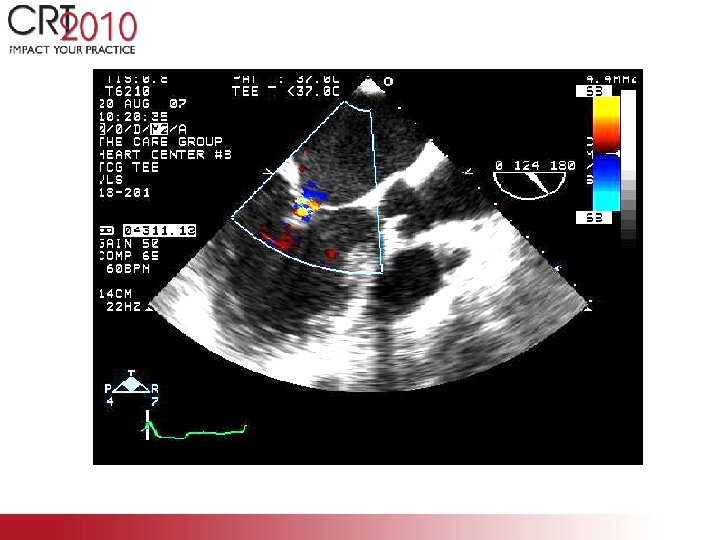
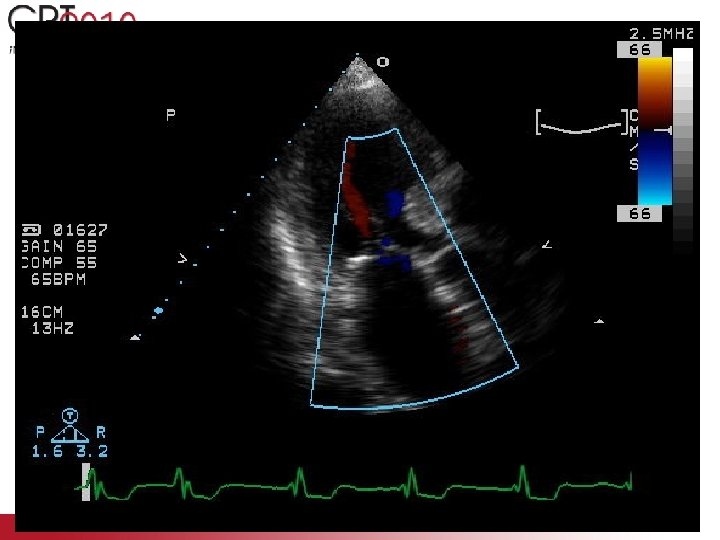

Case Example: Functional MR • 2. 5 years later – FCI I- II mild DOE • No recurrent hospitalizations for CHF • No MACE • LVEF increased from 25 to 40%; LVIDs – decreased from 5. 7 to 5. 0 cm

Technical Issues With FMR • Because of tethering of the leaflet tips, too much height (room above the annulus) rather than too little height is most frequent problem • Posterior leaflet retraction may require separate grasping of the anterior and posterior leaflets • Often patients have had prior open heart surgery and are elderly – thick atrial septum which may require balloon dilatation for successful guiding catheter delivery to left atrium

Conclusion These preliminary data suggest that patients with severe functional MR benefit significantly from the Mitra. Clip therapy with substantial improvements in functional class, MR reduction and ventricular volume/dimension metrics
- Slides: 24