Structural Heart Imaging in the VA Tricuspid Regurgitation




-Tri. Clip device • prospective, single-arm, multi-center")
 • 25%")



 Imaging • TV imaging is challenging • Three TV leaflets (anterior,")





 • 12. 5 -Fr catheter • Enlarged")


- Slides: 25
Structural Heart Imaging in the VA Tricuspid Regurgitation Mackenzie Mbai, MD Multimodal Imaging Director, Echo and Cardiac CT, Structural Heart Program-Minneapolis VAMC and Assistant Professor Of Medicine, University of Minnesota
80 yo male with mild dementia referred for evaluation of Progressive dyspnea >1 year Exam: venous distention, TR murmur, no RV lift Creat 2. 2 Transthoracic Echo: Isolated severe TR. IVC 3. 3 cm. RA is dilated RV normal function. Dilated annulus (4. 2 cm)-presumed mechanism of TR. TEE, right heart catheterization RAP 16, and coronary angiography: non obstr CAD What do you do next? Medical management, Refer to CV surgery , other options
Isolated Tricuspid Regurgitation • • Over a 10 -year period, 289 patients with isolated TR were identified. Mean age was 79. 2± 10. 6 years 70. 6% (204) were women Atrial fibrillation was present in 74. 0% (214), 24. 6% (71) had an intracardiac device 5 years after diagnosis, 51. 5% hospitalized for heart failure. Observed 5 -year mortality was 47. 8% compared with 36. 3% (P=. 005)** multivariate regression identified as associated with increased mortality • dilated inferior vena cava (≥ 2. 1 cm) without respiratory variation on echo ( HR 1. 93; P=. 02) • creatinine >1. 6 mg/d. L (HR, 1. 8; P=. 009). Fender, Nishimura et al. Mayo Clin Proc. 2019
Tricuspid clip success • Clip implant without detachment or migration • No tricuspid stenosis (gradient <3 mm. Hg) • Reduction in TR > or equal to 1 -grade Nickenig et al Triluminate EFS Circulation 2017
TRILUMINATE Feasibility Study for symptomatic tricuspid regurgitation (TR)-Tri. Clip device • prospective, single-arm, multi-center study feasibility study of 85 patients (21 sites) At 30 -days • Reduction in TR severity of at least one grade in 86. 6% of patients (p < 0. 0001) • Improvement in NYHA class I or II (84% at 30 days, compared to 22% at baseline) • Improvement in in quality-of-life scores(QOL) KCCQ score At 1 -year • NYHA class I or II (80% at 1 -year, compared to 22% at baseline) • Improvement in QOL scores by KCCQ seen at 30 d maintained at 1 -year Nickenig et al. TRILUMINATE study Euro. PCR May 2019
Severe symptomatic TR • 1. 6 million sufferers in US (<1% treated) • 25% Primary • 75% Secondary [1] • Severe tricuspid regurgitation (TR) is associated with a reduction in exercise capacity and a poor outcomes. • Patients with severe TR who undergo mitral valve surgery should undergo concomitant tricuspid valve repair (TVR) because TR does not usually resolve if only the mitral valve is repaired [1, 2] [1]. Nishimura et al JACC 2015 [2]. Takano et al. Surg Today. 2017
Concomitant Tricuspid Annuloplasty in MV Repair TMTVR and TMVR in high risk patients Kaplan-Meier estimates for freedom of heart failure hospitalization up to 18 months after TMTVR (green) and TMVR (blue) in high risk pts. Chikwe, Adams et al JACC 2015 Besler et al JACC Intver. 2018
Curio et al Interventional Cardiology Review-Radcliffe Cardiology 2019
Curio et al Interventional Cardiology Review-Radcliffe Cardiology 2019
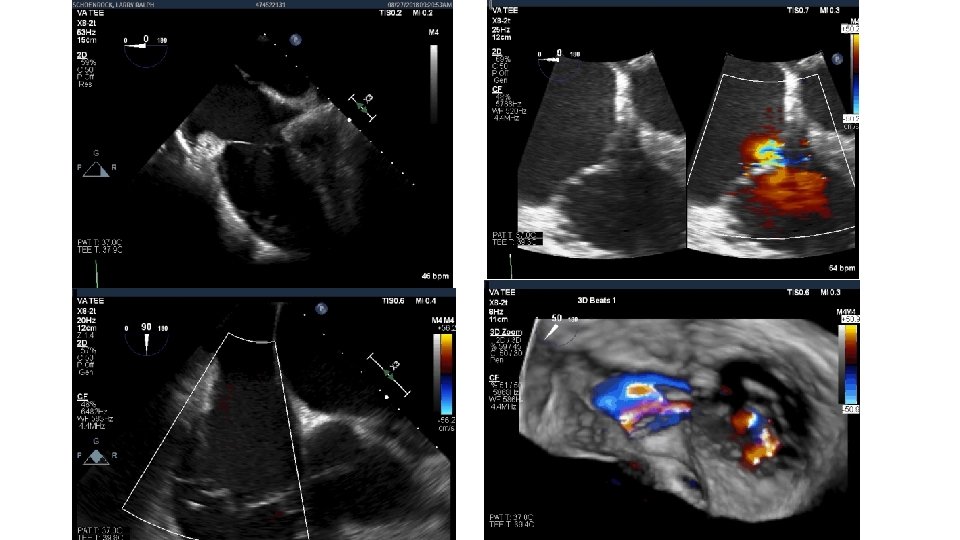
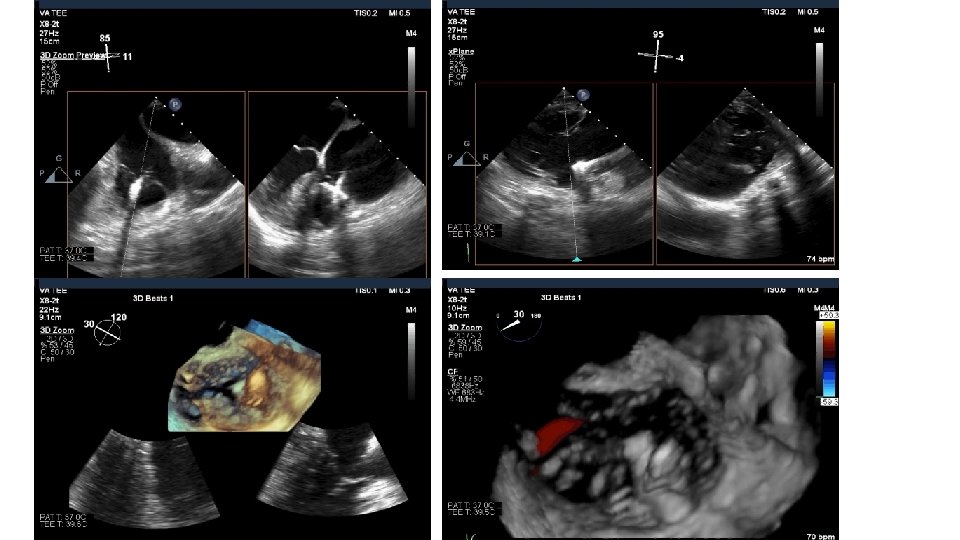
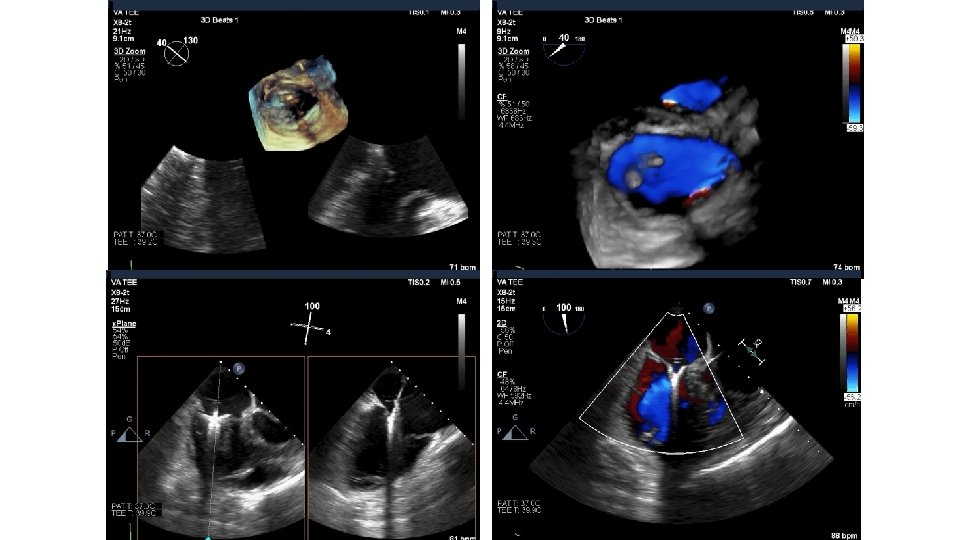
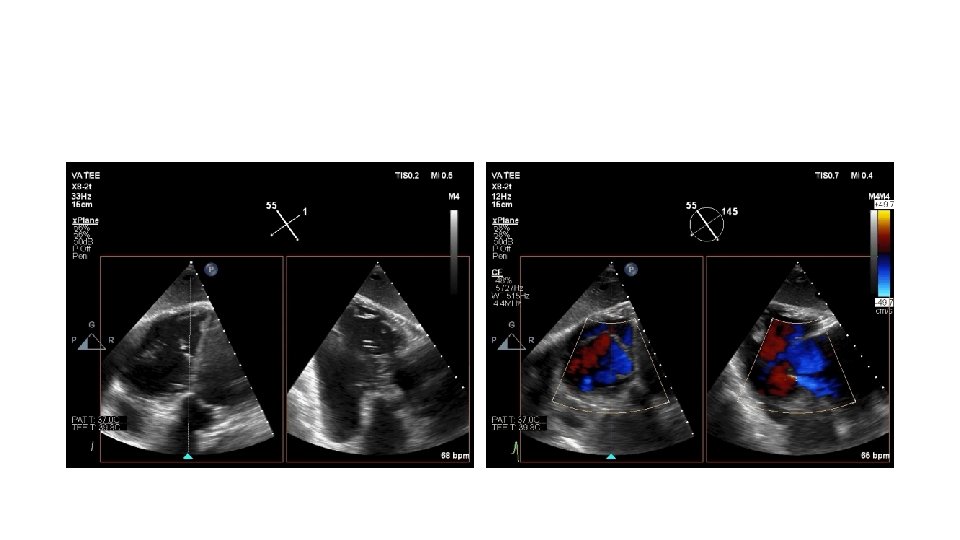
Tricuspid Valve (TV) Imaging • TV imaging is challenging • Three TV leaflets (anterior, septal and posterior) are thin and membranous Huitin et al. Archives of Cardiovascular Diseases Volume 109, Issue 1, January 2016, Pages 67 -80
• TV assessment • severity of TR • Mechanism of • mode of leaflet coaptation, • degree of tricuspid annulus enlargement and tenting • TAPSE • 3 D-TEE • Cardiac CT • cardiac MRI
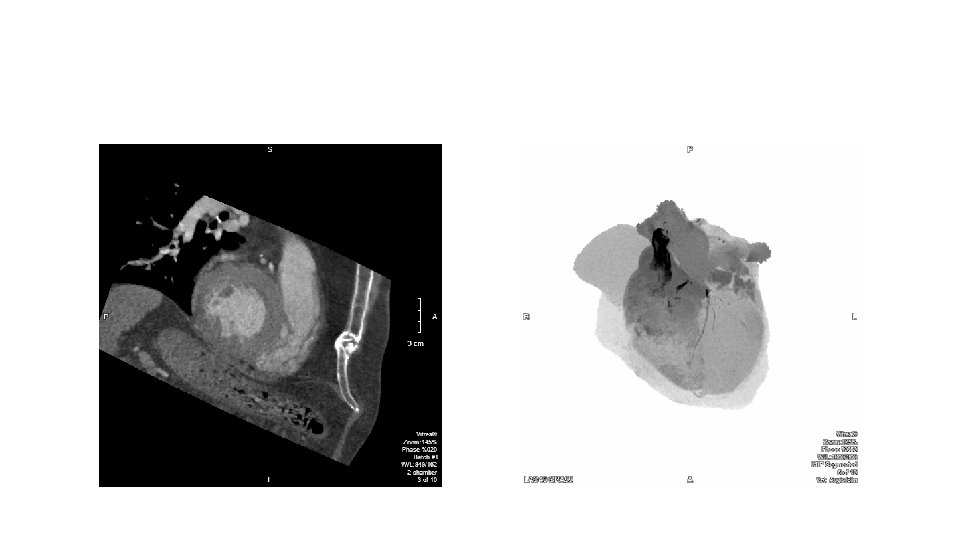
CT and MRI
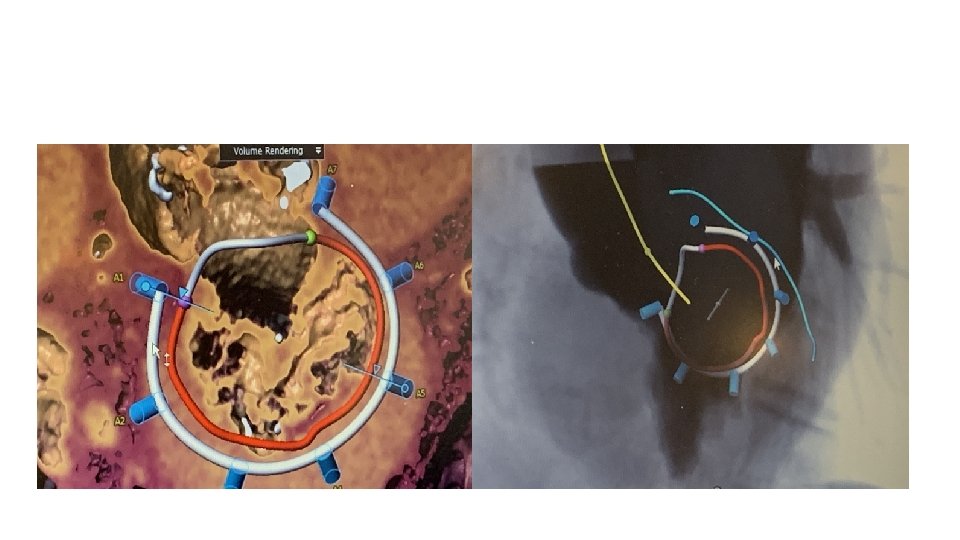
Direct annuloplasty for functional TR Schueler, Nickenig et al JACC Interventions 2017
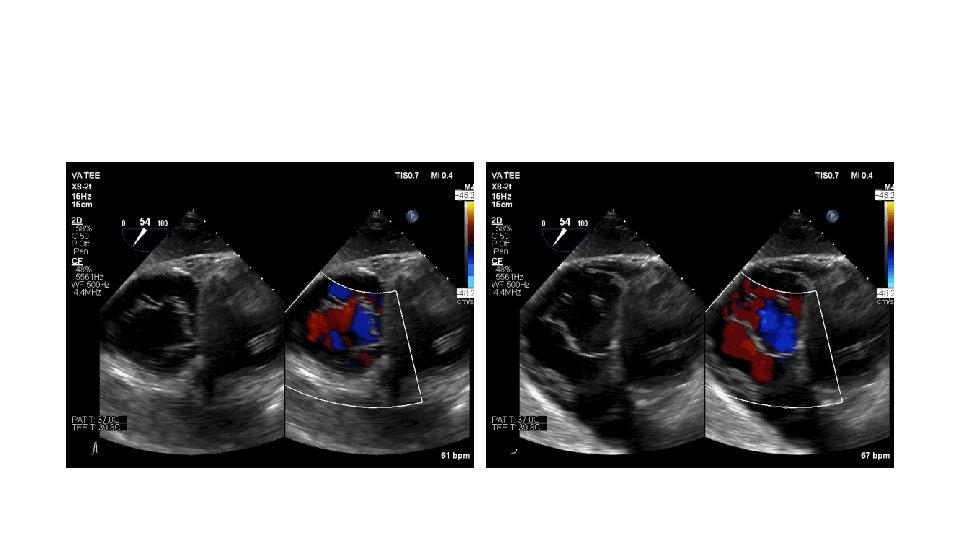
Wide angle 3 D intracardiac echocardiography (ICE) • 12. 5 -Fr catheter • Enlarged opening angle (FOV) capable of obtaining a volume of 90 x 50 deg • Depth (far field) imaging remains limited • Frame rate of 3 D/4 D limited at 16 volumes per second
3 D Wide volume ICE Ribero J. Rev Esp Cardiol. 2018
Conclusions • Symptomatic TR ? undertreated and represents large unmet need • Emerging transcatheter options for those ineligible for TV surgery • Tricuspid valve imaging is involving and evolving • Preop assessment with echo. CT and MRI are adjunctive imaging tools • Intraop: echo (TEE, ICE , TTE), fluoroscopy and fusion imaging