Strongyloides stercoralis Anguillula stercoralis Bavay 1876 Geographic distribution


Strongyloides stercoralis Anguillula stercoralis Bavay 1876

Geographic distribution • • • Worldwide • Warm, humid environments • Poor sanitation highest prevalence • Soil contaminated 1% of world population In tropical region Asian, Africa, South America Man maintain infection up to 36 years

Transmission • Direct contact with soil containing Location • Adult female worms are embedded in the mucosa of the duodenum and jejunum

MORPHOLOGY


Entamoeba coli Larva II 2 -3 mm

Free-living female Strongyloides stercoralis 30 µm 1 mm

Parasitic female Strongyloides stercoralis Head Tail Eggs • Small, transparent 60 µm • 2 -2. 2 mm, tail pointed • Cylindrical oesophagus • Paired uteri, 10 -20 eggs

Narrow: snake-like ♀

The existence of parasitic♂ • • Debated over many years Shorter, broader than ♀ Don’t have penetrating power Don’t invade the intestinal wall Free-living ♂ • Smaller than free-living ♀ • 0. 7 -1 mm, tail pointed, curving ventrally • 2 copulatory spicules, with a gubernaculum

• Thin shelled and indistinguishable from Hookworm eggs • Rarely seen because they embryonate and hatch in the s. intestine • 50 -58 µm • Transparent • Ovoid Larva ~250 µm in length

Life cycle – Very complex – Parthenogenic females in layers of intestinal tissue (sometimes lungs, gall bladder, pancreas) and produce partially embryonated eggs
 Dog")
autoinfection Primate Rhabditiform in intestines mature to filariform (rare) Dog
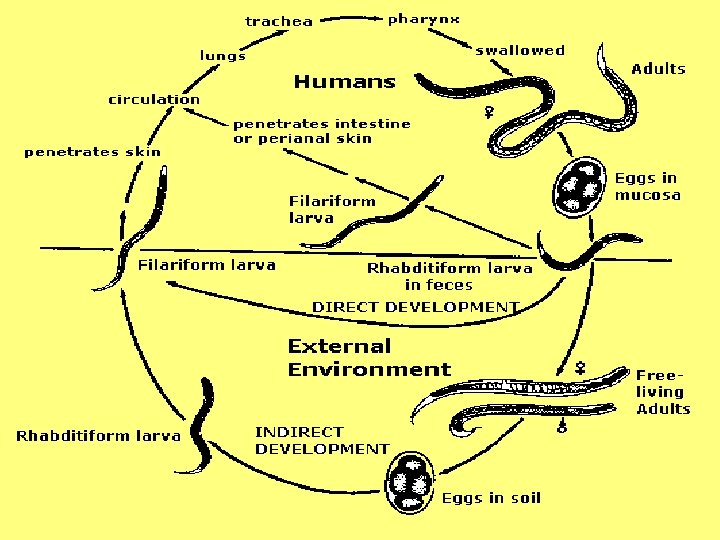


Auto. Inf Larvae smaller than external Inf L

Strongyloidiasis Cochin-China diarrhoea

Invasion stage • • Intense itching at site of entry- creeping eruption papular erythematous rash Hives Urticaria
 • • Asymptomatic Damage to lung tissue Cough, wheezing , transient")
Migratory stage (Pulmonary) • • Asymptomatic Damage to lung tissue Cough, wheezing , transient pulmonary infiltrates Pneumonitis, chest pain, allergies • Eeosinophilia that may be quite high

Pneumonia

Pulmonary haemorrhage due to migrating

Intestinal phase • Frequently asymptomatic • Heavy infections - pain, vomiting, diarrhea • Death is often result of imbalance of fluid and electrolyte levels • Epigastric pain, abdominal cramps • Malabsorption, weight loss • Perianal itching • Peripheral Eosinophilia

Loeffler's syndrome • The combination of transient pulmonary infiltrates and eosinophilia

Acute strongyloidiasis ØProtein losing enteropathy Ø Hypokalaemia Ø Paralytic ileus Ø More common in children Ø Serology usually negative

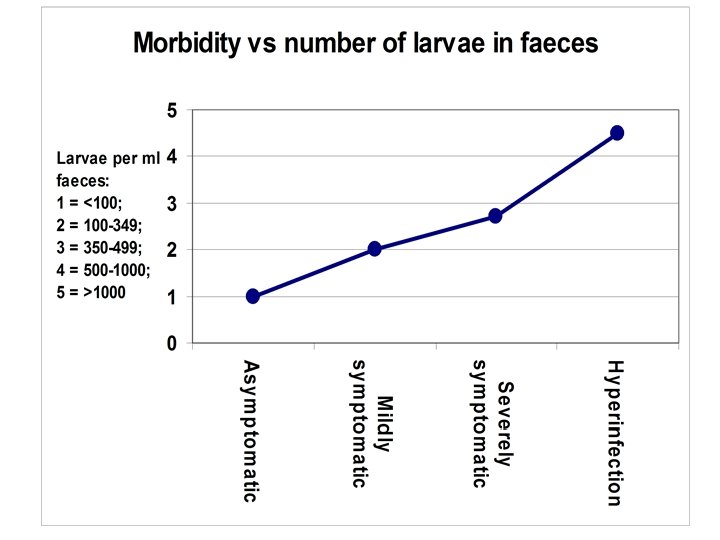
Hyperinfection Syndrom • >80% mortality • Rhabditiform larvae change to filariform in host (large scale) drugs, immune suppression • Large numbers of larvae transform into infective stages • • • Invade the intestine induce cell death Severe diarrhea and bloody diarrhea About 90% of cases are immunodeficient Meningitis Eosinophilia generally absent

Disseminated strongyloidiasis • Migrating larvae produce symptoms in other organs, liver, heart, kidneys, or central nervous system • Bacterial infection is common (50%) – pneumonia – septicaemia – meningitis • Gut signs

Gastrointestinal pathology

Strongyloides stercoralis in situ S. s

Larva of Strongyloides stercoralis in skin

Strongyloides tunnels through the mucosa of the small intestine



 2. “String” test Observe worms in")
Diagnosis: 1. Microscopic examination of feces (x 6) 2. “String” test Observe worms in stool Second stage larva

Acute strongyloidiasis • Diagnose by finding larvae in faeces • ELISA detecting genus specific Ig. G

Drug of choice: Ivermectin Thiabendazole d s e s i rea is m a h o pr ic for t om dem ed c o n n y un in e ree rap m e c Im nts e th tie ld b for a p ou be sh

Prevention and Control: • Sanitary disposal of human feces • Wear shoes/gloves when in contaminated soil • Proper sanitation • Hand washing Low Tech High Tech *Dog is a common reservoir host. Cannot control spread of dog feces which may contain infective larvae

Once infected with S. stercoralis always infected. . unless properly treated
- Slides: 41