Strokes Hemorrhagic stroke Stroke is acute disorders of







")





 Renewal (up")










")






 Epistatus Uremic coma Diabetic coma Traumatic hemorrhage Brain")



 – aneurysm rupture.")












- Slides: 56
Strokes. Hemorrhagic stroke
Stroke is acute disorders of cerebral circulation, rapidly developing clinical signs of focal (at times global) disturbance of cerebral function, lasting more than 24 hours or leading to death with no apparent cause other then that of vascular origin
Hemorrhagic stroke Intracerebral (when the hemorrhage is into the substance or parenchyma of the brain ) Membrane – – subarachnoid (when the bleeding originates in the subarachnoid spaces surrounding the brain) epidural and subdural Combined – – subarachnoid – parenchymatose– subarachnoid parenchymatose–ventricular
The most common causes of hemorrhage are: Hypertension Symptomatic arterial hypertension (at kidney diseases, systemic vessel processes) Inborn arterial and arterio – venous malformations Blood diseases (leucosis, polycythemia) Cerebral atherosclerosis Intoxications, such as uremia, sepsis
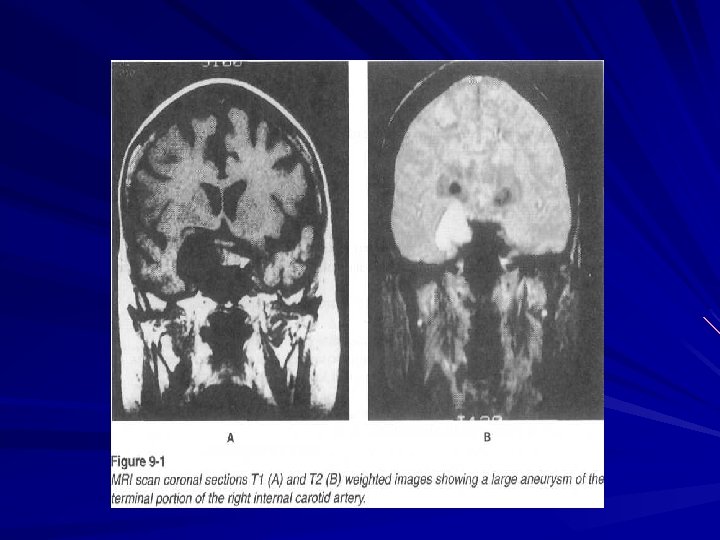
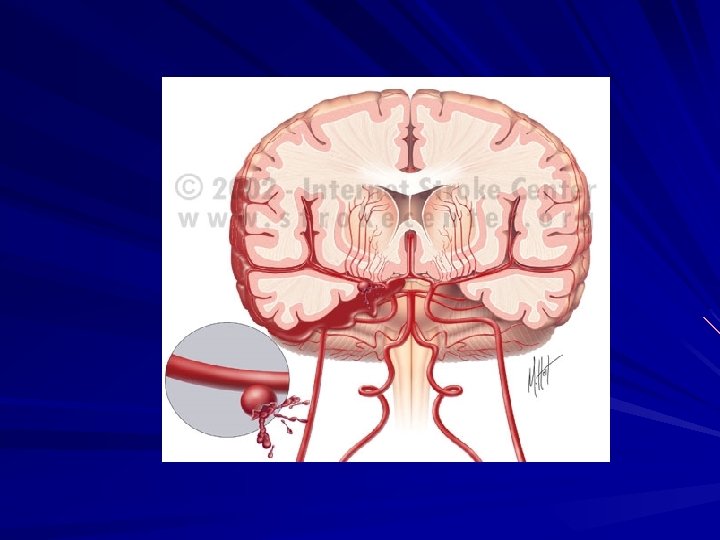
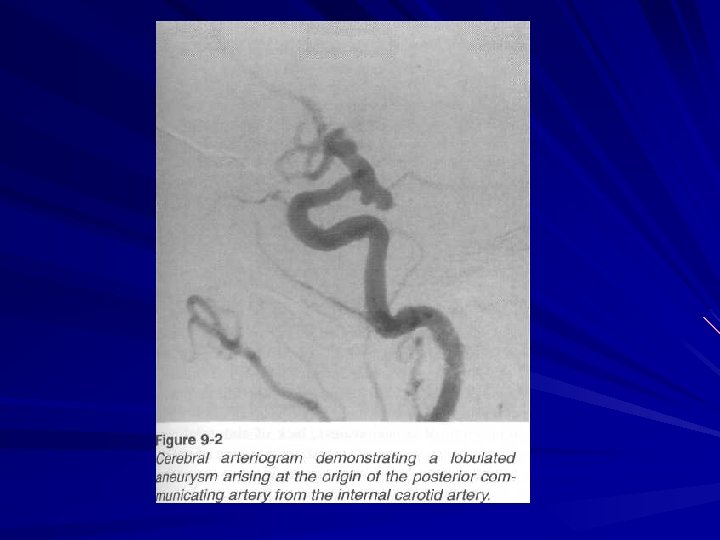
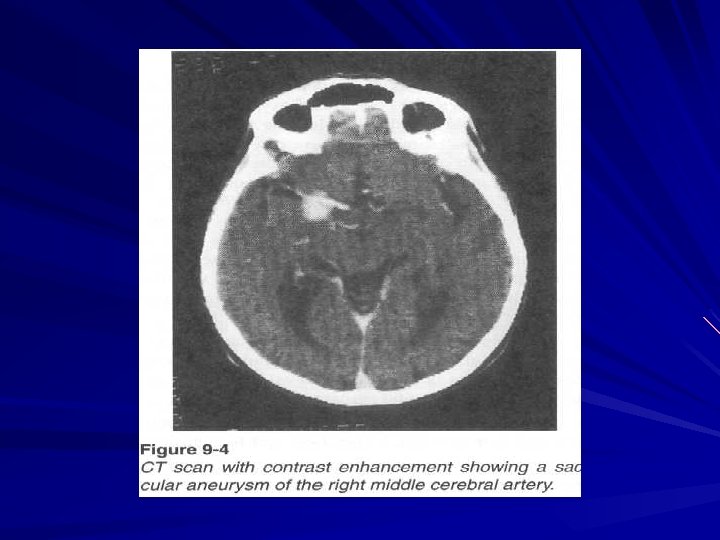
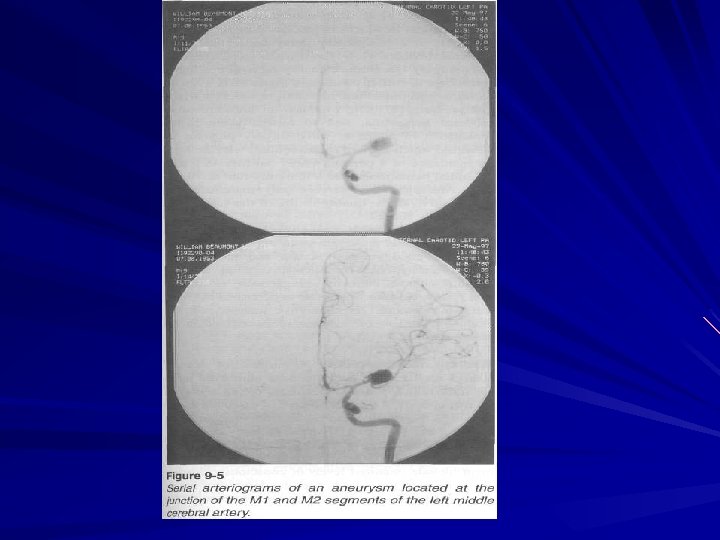
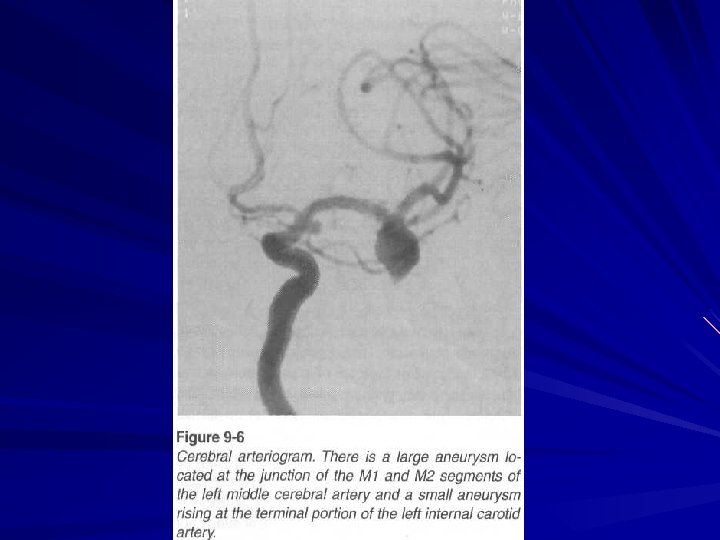
Aneurysm
Aneurysm
According to the localization there are : Lateral hemorrhage (they are located laterally compared with the internal capsule)
Medial hemorrhage (they are located medially compared with the internal capsule)
Combined hemorrhages (they take the whole region of basal nuclei: subcortical nuclei, thalamus, internal capsule)
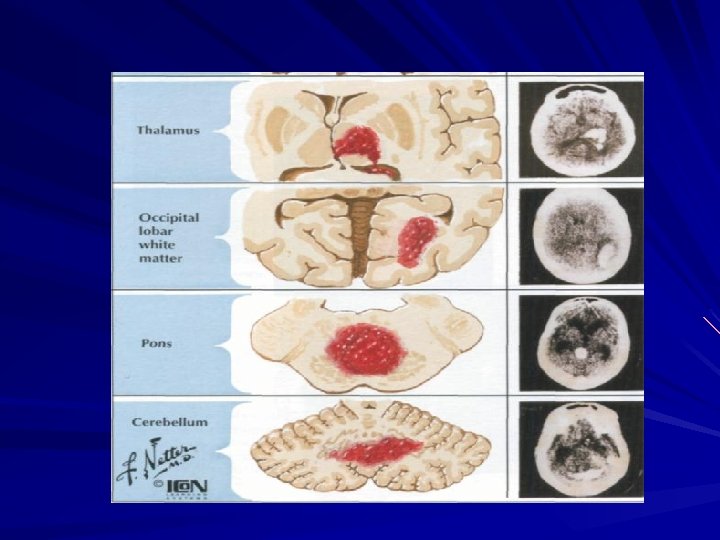
Brain stem hemorrhages Cerebellar hemorrhages
In hemisphere
In ventricules
Pathomorphology Per rexis Per diapedesis
The main periods of stroke Acute (up to 3 – 4 months) Renewal (up to 1 year) Residual
Stages of acute period Precursors Apoplectic stroke Focal signs
General cerebral symptoms - severe headache nausea vomiting seizures consciousness disorders sopor stupor semicoma
Coma is characterized by deep consciousness disorder, disturbance of breathing and heart activity. The patient doesn’t respond to stimuli.
Coma response to stimuli is absent eyes are closed, mouth is opened face is red, lips are cyanotic, skin is cold, neck vessels are pulsing there is breathing disturbance pulse is strained and slow blood pressure is increased temperature increases in 24 hours patient is lying on his back all muscles are relaxed pupils are changed (there can be anizokoria, cross – eyes, sometimes gaze paresis can be observed) mouth angle is a little bit lower
On the opposite side hemiplegia is often observed: the arm is falling down like bine there is hypotonia of muscles reflexes are low Babinski sign is often observed too
Large hemisphere hemorrhage meningeal signs vomiting and dysphagia retention of urine or involuntary urination in case of cortex irritation epileptic attacks
Sign of paralysis in right side
Sign of central paralysis
Secondary brain stem syndrome progressive breathing disorders disturbance of heart activity consciousness disorders disturbance of eye movements changes of muscle tonus (hormetonia) autonomic disorders (sweating, tachycardia, hyperthermia)
Brain stem hemorrhage tetraparesis alternating syndromes eye movements disorders Nystagmus gorge disorders cerebellar syndromes.
Pons hemorrhage ptosis gaze paresis increased muscular tone (hormetonia)
Cerebellar hemorrhage Dizziness Severe headache in occipital lobe Vomiting Eye movements disorders Ptosis Gervig – Mazhandi syndrome, Parino syndrome Cerebellar symptoms - nystagmus, dysartria, hypotonia, ataxia Paresis of extremities is not common
Complication of intracerebral hemorrhage is rupture into the ventricle system. This is usually associated with: worsening of patient’s state Hyperthermia breathing disorders hormetonia manifests as changes of muscle tone in extremities, when hypotonia is changed into hypertonia in a few seconds or minutes.
Diagnostics In blood usually leucocytosis, related lymphopenia, hyperglycemia (up to 8 – 10 mmole per liter) In liquor high pressure during lubar puncture a great number of erythrocytes are found On eye fundus – retinal hemorrhages, hypertonic angioretinopathy and Salus symptoms are observed At echoencephaloscopy there is dislocation of middle structures on 6 – 7 sm to the healthy side At angiography - aneurysm, dislocation of blood vessels, to find out zone “without vessels“ CT and MRI find out hyperdensive focuses.
In liquor high pressure during lubar puncture a great number of erythrocytes are found 1. normal 2. subarachnoid hemorrhage 3. intracerebral hemorrhage 4. xantochromia
On eye fundus – retinal hemorrhages, hypertonic angioretinopathy and Salus symptoms are observed 1 -2 embolism of retinal vessels 3 – hypertensive encephalopathy 4 – subarachnoid hemorrhage
At echoencephaloscopy there is dislocation of middle structures on 6 – 7 sm to the healthy side
Differential diagnosis Infarction of brain (thrombembolic) Epistatus Uremic coma Diabetic coma Traumatic hemorrhage Brain tumor with inside hemorrhage
Subdural haematoma
Subdural haematoma
MRI. Intracerebral hemorrhig
Subarachnoid hemorrhage Aetiologic factors: Aneurysmatic ( 50 – 62 % ) – aneurysm rupture. Hypertensive ( at hypertension ) Atherosclerotic ( 15 % ) Traumatic ( 5 – 6 % ) Infectious – toxic ( 8. 5 % ) Blastomatose ( at tumors ) Pathohemic ( at blood diseases ) Cryptogenic ( 4 – 4. 8 % )
Clinical features Severe headache or feeling of hot liquid flowing in the brain (pain is local in the region of occipital lobe). Later pains in neck, back appear, sometimes they irradiate in legs. Simultaneously with headache vomiting and nausea occur. there are other general cerebral symptoms: short loss of consciousness, psychomotor excitement, seizures.
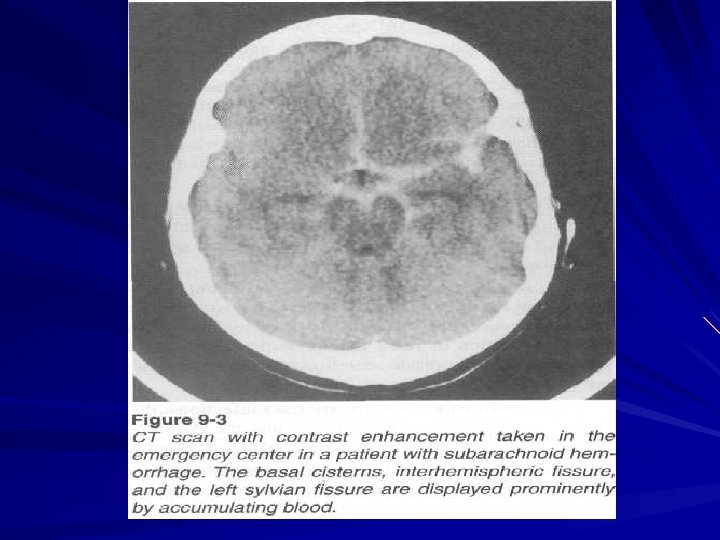
Subarachnoid hemorrhig
Subarachnoid hemorrhig
Clinical features Meningeal syndrome rigidity of occipital muscles symptoms of Kernig, Brudzinsky general hyperesthesia. Significant focal neurologic symptoms are not common. Only in case of basal hemorrhage CNs suffer (that is the reason of ptosis, cross – eye, dyplopia, paresis of mimic muscles). That’s why lesion of CNs is typical for basal aneurysm rupture.
Kernig’s sign
Complications Brain edema Recurrent SH Occlusive hydrocephalia Brain infarction
Diagnosis Stroke – like development with general cerebral and meningeal symptoms and absence of significant focal neurologic deficit The presence of blood in liquor (bleeding liquor during first day and yellow liquor on 3 rd – 5 th day) Retinal hemorrhages are on eye fundus
Differential diagnosis Meningitis Acute food toxic infection Infectious diseases
Strokes treatment Nondifferential treatment includes: Prevention and treatment of pulmonary insufficiency Liquidation of heart – vascular disorders Brain edema treatment Normalization of water – electrolytes balance and acid – alkali balance Osmosis correction Improving of brain metabolism Liquidation of hyperthermia and other autonomic disorders
Brain edema treatment Diuretics Corticosteroids Albumini Ganglioblockers 20 % mannit Manitoli Glycerini Lazix Diakarbi
Differential treatment of hemorrhage The main directions of treatment are: – To lower increased blood pressure – To liquidate brain edema and lower intracranial pressure – To increase coagulative properties of blood and decrease penetrance of vessels’ wall – To prevent and treat cerebral vessels spasm – To normalize vital and autonomic functions and prevent complications – To treat hypoxia and brain metabolism disorders