Strengthening Facility Based New Born Care Madhya Pradesh

Strengthening Facility Based New Born Care Madhya Pradesh Experience
 UNICEF Type your title in this FOOTER")
Infant Mortality rate in India (SRS 2008) UNICEF Type your title in this FOOTER area and in CAPS

Half of Child Deaths occur in the Neonatal Period When do neonates die? Day deaths 1 st day 20% By 3 rd day 25% By 7 th day 37% By 28 th day 50%

Half of Child Deaths occur in the Neonatal Period If we have to achieve MDG 4 we need to address Neonatal Mortality

Care of Sick Neonate: Government Sector • Specialized Care Non Existent…… • Sick New Born clustered in General wards. • Equipments primitive. • Staff untrained for New Born Care. • Some services available at District level, Non existent beyond.

Care of Sick Neonate: Private Sector • Very few beds • Unaffordable for parents • Health Insurance for Neonates not developed

We also need to reach to places where they are referred…. WHY ? ? • Increasing load of New Born due to success of JSY • 15% needs special care. • Increased referral of Sick Newborn from Community under IMNCI. • Failure to do so would shift the mortality burden from Community to Hospitals.

The Need “Augmenting Essential Newborn Care at facility level”

Strengthen Facility based Newborn Care Components : • Establishing Sick New Born care Units at District and Block Level. • Triage or three tiered system of primary (Level I) at Block level, Secondary (Level II) at District level and Tertiary (Level III) care at Medical College level with inter linkages. • 24 hours safe delivery and Essential New born care facilities at PHCs. • Non government , private sector effective utilization for newborn care

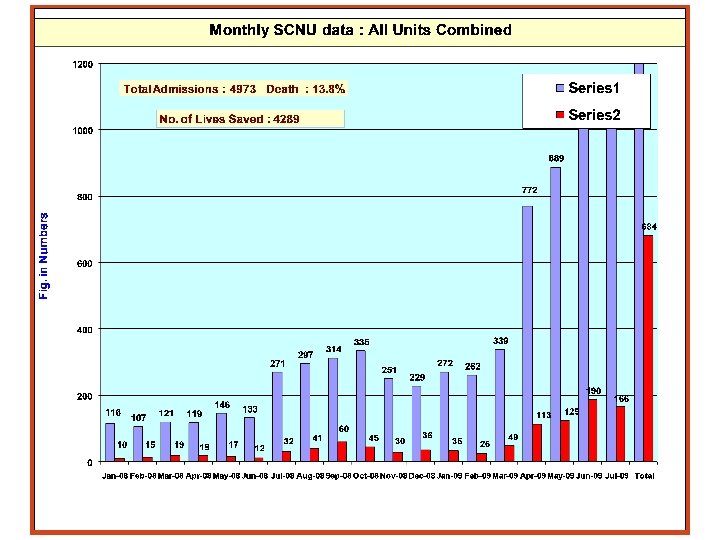
Sick New Born Care Unit - Guna • Needed to address increasing load of newborns due to doubling of delivery load and increased referral under IMNCI. • 20 bedded level II Unit started at District Hospital, Guna. • 4 Pediatricians & 12 Staff nurses • First of it’s kind in Government set up in Central India.

Sick New Born Care Unit - Guna • Joint effort of GOMP and UNICEF under NRHM. • Establishment cost Rs. 40 lakh and Operational cost Rs. 15 lakh per year • Services free of charge for Patient. Cost to Govt. Rs. 4000 per New Born saved

Scaling -up n n 20 bedded level II Unit at 13 more District Hospitals. UNICEF technical partner for designing, Quality monitoring and training of staff. This year we are planning 15 more SNCU. Two SNCU through PPP mode.

Way forward… • SNCU for 15 district Hospitals will be established under NRHM in year 2009 -10. • By end of year 2009 -10, 28 SNCU will be established • 22 more districts need level 2 SNCU for which proposal is submitted. • When scaled up to entire State would save 63, 000 New Born each year, thus decreasing IMR by nearly 30%

Status of Special Care New Born Units Under Construction MR N B HD Near Functional GL R Functional DTA S OP S VP NMC GUN TK M AK N R WA C TP G MDS R TM SJP DHR IDR DMH B PL UJ N DWS BRW K ND B HP S DH K TN NS P MDL S NI C DW B TL UMR DDR HS B HR D KRG S TN S DL JBP RSN S HE JBA SA VDS RJG PAN BLG ANP
/ Unit Cost 1 Civil")
Establishment cost of SNCU S. No, Work Cost (in lacs)/ Unit Cost 1 Civil Work 25 2 Equipments 20 3 Manpower 29. 28 4 Recurring Cost (Oxygen, Maintenance, Electricity etc. 15. 00 Total 89. 28

Thank You
- Slides: 18