STRATEGY FOR ACCESSIBLE AFFORDABLE AND QUALITY HEALTHCARE IN

STRATEGY FOR ACCESSIBLE, AFFORDABLE AND QUALITY HEALTHCARE IN KENYA 11 th Feb 2010

Presentation Outline Introduction: background and process Health Sector priorities and objectives Ongoing Reforms and rationale Process of developing the strategy Goals and core values of the proposed strategy on affordable healthcare Proposed changes What it means to the sector and country Implementation framework

Vision • Vision of the Health Sector: • A nation free from preventable diseases and ill health • An efficient, integrated, high quality and affordable health care system • In line with Vision 2030: “Kenya will restructure the health delivery system and also shift the emphasis to “promotive” care in order to lower the nations’ disease burden. ”
;")
Specific Objectives • • • According the National Health Sector Strategic Plan (2005 -10); the Health Ministries Strategic Plans (200812) and Vision 2030, the key objectives can be summarized as follows: Increase equitable access to health services Improve quality and responsiveness of services Improve efficiency and effectiveness of service delivery Enhance the regulatory capacity Foster partnerships in the delivery of services Improve the financing of the sector

Comprehensive Reforms - Ongoing Strategic human resource management: equity in distribution and motivation of staff Upgrading/modernising and expanding of the health infrastructure and equipment – in terms of number, rehabilitation and upgrading The transformation of management practices in the health facilities – decentralisation, leadership, use of ICT and effective referral system Promotion of community participation and ownership through the community strategy Strengthening the collaboration between the public and private sector - centres of excellence and medical tourism

Comprehensive Reforms Cont. Efficiency and accountability in procurement and the supply chain – including restocking, planning and strengthening KEMSA operations Institutional strengthening – policy, regulation and standards as well as treatment modalities Transformation of the healthcare financing system: Ensure equitable allocation of resources to reduce disparities in health status Increase cost-effectiveness and efficiency of resource allocation and use Move from oop, taxes and user fees to Social health protection

Why the focus on above priorities? • Only about 40% of Kenyans live within 4 kms of a functioning facility, mostly in rural areas; 70% access in urban areas • About 52% of all health facilities are operated and managed by the Ministries of Health Public and related institutions – indicating vital role in sector • Public health facilities are overcrowded, while there is still some underutilized capacity in private and FBOs facilities (exact figures not known) – issue of cost of care and quality

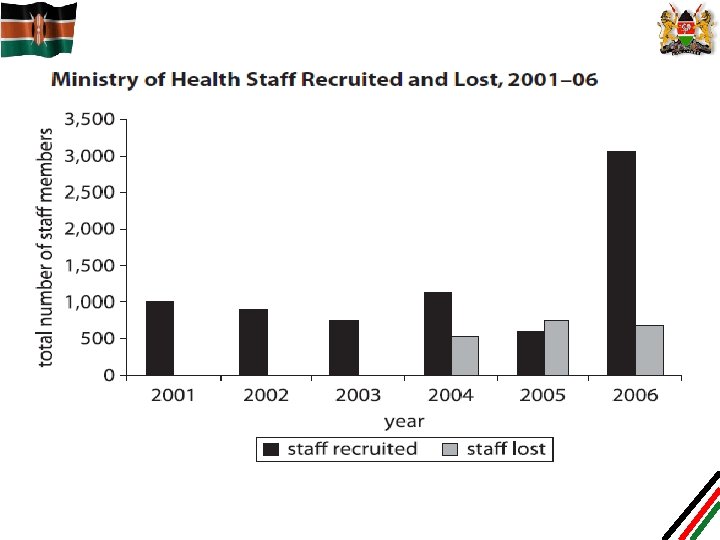
Why the focus on above priorities? Cont. • Continued shortage of health workers has been associated with poor health indicators: – Shortage due to freeze of employment since 1990 s – Out of 72, 234 proposed establishment for health staff, only 33, 317 are in place (38, 91 vacant) – L 2 & L 3 alone will require more 24, 800 nurses once new facilities are completed in the next 3 years – Out of 5, 926 doctors, only 2000 are public sector – Out of 41, 679 nurses, only 17, 347 are in public sector – Mal-distribution of health workers – urban vs rural – Challenge of retention due to resignation, desertion, termination and death

Why the focus on above priorities? Cont. • High burden of disease, including HIV/AIDS, Malaria, TB • Whereas the policy and the plans emphasize preventive, demand for curative services continue to increase • Households bear the highest cost of care – direct costs, taxes and premiums

Why the focus on above priorities? Cont. • About 40% of sick Kenyans do not seek care when sick due to cost • About 1 million people go into poverty due to some illness in the family • Removal of user fees in primary health facilities led to shortages in health commodities due to lack of compensation for loss of revenue

Process of Developing a new Strategy A multi-stakeholder Task Force established by the Minister for Health in 2006/07 to: 1) Develop a long-term financing healthcare strategy; 2) Propose a time bound action plan for implementation A number of studies undertaken to inform the process Study tours to other countries to inform and learn from their experiences A Health Financing Working Group was reconstituted in February 2009 to steer the process The draft strategy and the presentation is a product

Proposed Health Financing REFORMS

The ultimate objective of any healthcare financing system… “effective access to affordable healthcare services of adequate quality and financial protection in case of sickness” (International Labor organization)

Aim of the strategy Contribute to national welfare, economic growth and increased productivity through the establishment of a health financing system to provide the highest attainable standard of health for all Kenyans. In line with the foundations of Kenya's nationhood built on the values of human dignity, social justice and equal access to resources and opportunities.

Goals of the strategy • Create a system which guarantees access to quality healthcare • Protect all Kenyans from health related financial shocks; • Promote efficiency in the provision of health services • Improve the effectiveness and efficiency of revenue collection and risk pooling • Improve governance and transparency in order to optimize the use of the available resources • Improve aid effectiveness in the health sector • Ensure sustainability of the health system

Core Values of Strategy The strategy should strive to ensure the fulfilment of the following values: Solidarity: The better off , the younger and healthier will support the poor, old and the sick. Responsibility: The system at all times put the people first, ensure quality, efficiency and cost-effectiveness as well as giving people choice and allowing competition within a regulated environment Equity: That ALL Kenyans will access to services according to needs and not according to their ability Transparency: That purchasers, providers and users will have access to information regarding the operations of the system

Supportive Reforms • Ministries of health to focus more on critical oversight – policy, regulation and standards • Greater decentralization of public health facilities – as being done through Health Sector Services Fund and Hospital Management Services Fund – Decentralisation will improve efficiency and accountability • Strengthen the Referral System • Restructuring and strengthening of NHIF into a National Health Services Trust – focusing on governance, efficiency, coverage for the poor and expansion to the informal sector. • Institutional audit of NHIF already initiated • Strong quality assurance and accreditation system – establish a Health Benefits Authority

Specific Changes Proposed • Remove user fees from primary facilities – govt policy • Pay public health facilities through output-based (for Hospitals) and capitation (Dispensaries and H/Centres) • Increase informal sector membership in SH Insurance • Channel donor funds through out-based and pool mechanisms • Give tax incentives to employers to co-pay for social health insurance of their employees • Promote private insurance and other risk pooling plans trough legislation • Promote community and other pre-payment schemes through appropriate legislation • Undertake studies on revenue collection and pooling
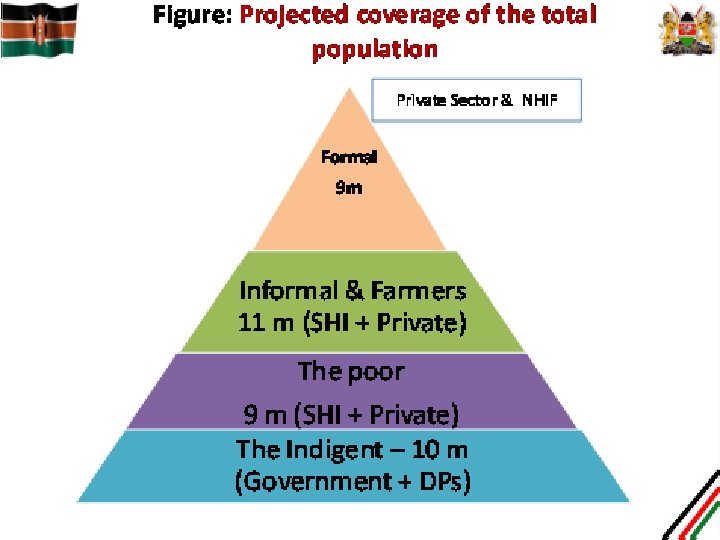

Development Partners Ministries of Health Benefits Board Projects * Insurance subsidy would be low formal workers, higher for informal workers/farmers (with possible subsidy for CBHI). Compensate providers for lost revenue for waivers/exemptions Access and Equity Funding to purchase services for national programs Subsidies* Formal Sector Informal workers and farmers “the poor ” National Health Services Trust /NHIF Contributions Private Insurance Risk Pool Negotiate Organize Identify Representative Groups (e. g. , KWFT) or CHF (at community level) Ministry of Gender & Youth (or MOH) User Fees. Private Insurance, Community Based Health Insurance Premiums paid on behalf of beneficiaries Payments for services under contract (uniform tariff – case based for hospitals, capitation/P 4 P mix for primary care Autonomized Public providers FBO/NGO/NFP Providers Private providers Figure: Social Healthcare Insurance System (with Significant Tax Financing)

What it means to the Sector • Increased access to primary care services through removal of user fees and compensation • Increased utilization of Primary care services as more poor people will be able to receive healthcare from Go. K, FBO and private facilities • Protection of financial resources for primary care • More resources for preventive and health promotion and curative services – and better services, drugs, etc • Reduction in number of preventable deaths

What it means to the sector Cont • Efficient mobilization of health resources from the households and the informal sector • Protection of the poor from impact of unplanned health expenditures • Predictable financing of the sector • Households have choice on where to pre-pay for healthcare and where to seek care • Better functioning referral system • Hospitals can specialize and provide advanced care

What it means for the Country/Sector • Efficient use of health infrastructure - reduction of idle capacity and over-crowding • Balanced growth of private sector and gradual reduction of government involvement in curative care • Universal coverage for all Kenyans and early attainment of MDGs • Increased individual productivity and growth of GDP • Health savings will increase • Increased foreign earnings as a result of medical tourism

Implementation Framework Build on existing institutions and experience Build on the lessons from the past, e. g. 2004 Bill Pilot test some of the approaches Refine mechanism for identifying the poor Have a strong communication strategy on the draft strategy – for inclusiveness • Focus first on the poor and vulnerable • Create linkages with other reforms in the sector and the Government • • •

NESC is requested to Advise Government to • Embrace the principles of universal coverage using social health insurance – in line with Vision 2030 • Introduce social health insurance by building on the structures and systems of the NHIF while bringing the poor into the system • Introduce legislation for the Health Benefits Authority Act to guide and regulate the health insurance and health risk pooling in the country
 • Create an environment for")
NESC is requested to Advise Government to (Cont. ) • Create an environment for other risk pooling plans and private insurance to provide SHI alongside the State run system • Set up the Equity Fund through which funds for the poor will be channeled • Remove all forms of user fees in public primary level health facilities and primary level faith based providers – either directly or through Social health insurance • Adopt the proposals in this draft strategy

Thank you for your Attention
- Slides: 28