Strategies for Heart Failure Prevention Stuart J Smith


 • Prevalence in")










 • Not recommended")
 • Community Based Studies – Prevalence of")



 Design • International multicentre trial •")





 to usual therapy in stable cardiovascular")



- Slides: 31
Strategies for Heart Failure Prevention Stuart J Smith MD Heart Failure Program St Mary’s Regional Cardiac Centre
Outline • • Know your enemy Epidemiology of Heart Failure – the Basics Pathophysiology / Stages of Heart Failure Implications for Prevention – Prevention of HF in CHD – Prevention of HF in asymptomatic LV dysfunction – Prevention of HF targeting BP
Epidemiology of Heart Failure AHA Heart & Stroke Statistical Update (2009) • Prevalence in US : 5. 7 million , males > females • Race adjusted prevalence – Caucasian : 3. 1 % male , 1. 8% for women – Blacks : 4. 2 % male , 4. 2% for women • Incidence in US – 670, 000 new cases /year with 1 % / year after 65 • Leading cause of hospitalization for age ≥ 65 – 1. 1 million in 2006 vs 0. 4 million in 1980 • Total US cost for HF ( 2009) : $37. 2 billion
Prevalence of Heart Failure by Age Prevalence of heart failure by sex and age (National Health and Nutrition Examination Survey: 2005– 2008). AHA Heart Disease and Stroke Statistics 2012 Update Copyright © American Heart Association
Lifetime Risk for HF by Sex and Age Framingham Heart Study A person aged 40 or over has a lifetime risk of heart failure of one in five, which is doubled if they have high blood pressure. Donald Lloyd-Jones Circ 106 : 3068 (2002)
Hospital Discharge for HF Hospital discharges for heart failure by sex United States: 1979– 2009 AHA Heart Disease and Stroke Statistics 2012 Update Copyright © American Heart Association
Trends in Incidence of HF Olmstead County , 1979 - 2000 Roger, V. L. et al. JAMA 2004; 292: 344 -350 Copyright restrictions may apply.
Incidence and Prevalence of HF in Medicare Patients , 1994 - 2003 Incidence Lesley Curtis et al; Arch Intern Med 2008 Prevalence Year Prevalence /1000 1994 89. 9 1996 104. 4 1998 114. 9 2000 119. 9 2002 121
Risk Factors and PARS for HF Olmstead County, 1979 -1999 Risk Factor Prevalence Odds Ratio (95%CI) PAR (95% CI) CAD 27% Hypertension 67% Obesity 24% Diabetes 19% 3. 08 (2. 26 – 4. 19) 1. 78 (1. 40 – 2. 25) 2. 54 (1. 84 – 3. 50) 3. 08 ( 2. 14 – 4. 44) 0. 18 ( 0. 14 - 023 ) 0. 29 (0. 19 - 0. 39) 0. 14 ( 0. 10 - 0. 19) 0. 13 ( 0. 09 -0. 17 )
Prevalence and Prognosis of HF Stages, Olmstead County Ammar et al. Circulation 2007; 115: 1563 -1570
Is the HF Epidemic a Consequence of Our Successes or our Failures ? ü Successes § Improved survival after MI incidence § Improved survival in patients with HF leading to prevalence ü Failures § Failure to control HTN § Failure to prevent progression from MI to HF ü Neither § Immutable consequence of an aging population
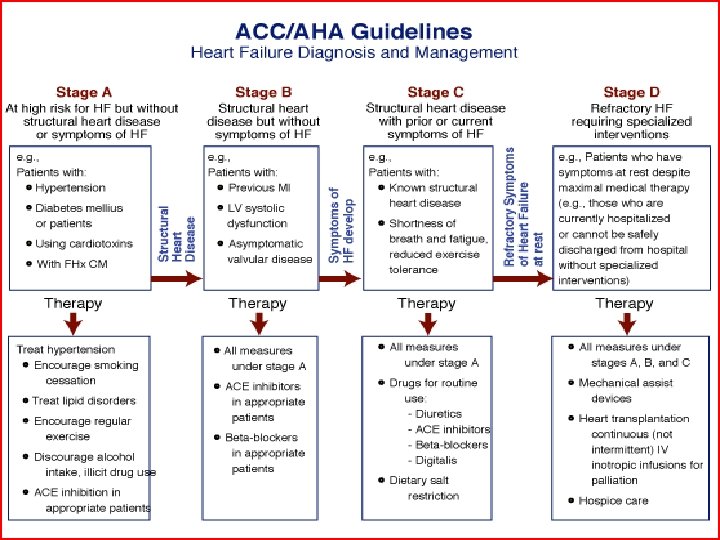
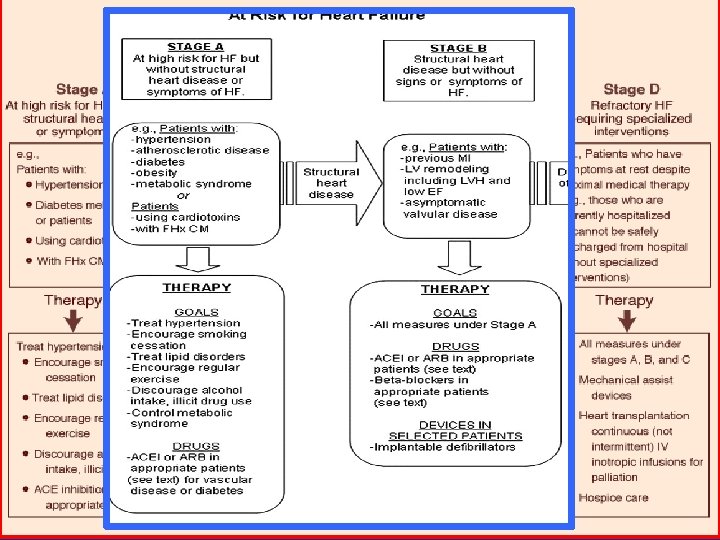
Primordial and Primary Prevention of Heart Failure • Prevention in all patients • Prevention in patients with asymptomatic LV systolic dysfunction ( ASLVD) • Prevention in patients with hypertension (HTN) • Prevention in patients with CAD • Prevention in patients with diabetes
Dietary and Lifestyle Factors • Major Risk Factors for HF all linked ( CAD , HTN , Diabetes , Obesity , Renal Disease) • All of these predisposing factors can be prevented or mitigated by diet and physical activity – Eg dietary sodium , vegetables /fruits, fat , less saturated fats , weight maintenance , weight loss
Role of Screening for Asymptomatic Systolic LV Dysfunction ( ASLVD ) • Not recommended as a “routine” • All AHA Stage A patients should be questioned about signs & symptoms of HF routinely. • Recommendation for echo screening for selected patient groups at “high risk” Eg Patients with hx of previous MI ( especially anterior) ; patients who received cardiotoxic interventions ; patients with strong family hx of HF in absence of other factors ( LBBB on ECG) • The future ? ? – BNP may be a “cost effective” means for yield
HTN and Asymptomatic Systolic LV Dysfunction (ASLVD) • Community Based Studies – Prevalence of ASLVD varies from 2 - 5% – Among those with ASLVD , the prevalence of HTN varies from 23% - 73% ……. Similar to prevalence of MI. • Progression from ASLVD to HF can be prevented ……. Wang et al. Ann Intern Med 2003
SHEP Trial : Cardiovascular Disease Endpoints - 13% -36% - 25% - 54% JAMA 265: 3255 ( 1991) - 32%
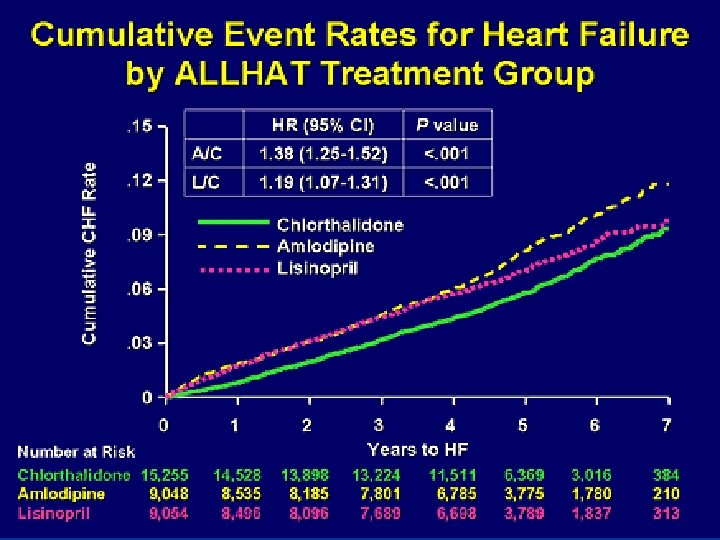
ALLHAT • N = 42, 488 factor : HTN , Age 55 PLUS 1 other CVS risk – Previous MI /stroke ; revascularization , Type II DM , low HDL , LVH , smoking – Excluded recent event , CHF or EF < 35% , Crt > 185 – Untreated BP 140 -180 / 90 -110 mm. HG – Treated ( 1 or 2 meds) BP <160/100 mm. Hg • Randomized to Cholthalidone vs Amolodipine vs Lisinopril vs Doxazocin [ 1. 7 : 1 : 1 ] • Enrolled 1994 1998 ; follow-up to 03 /2002 • Primary Endpoint : CAD death or non fatal MI
ALLHAT – Doxazosin Arm • 3. 3 years of follow-up • Relative Risk for: – All Cardiovascular Events 1. 25 ( P< 0. 001) – For Stroke 1. 19 ( P = 0. 04) – For Heart Failure 2. 04 ( P < 0. 001)
Hypertension in the Very Elderly Trial (HYVET ) Design • International multicentre trial • Patients ≥ 80 years with HBP – SBP 160 – 199 mm. Hg – SBP after standing 2 minutes ≥ 140 mm. Hg • Randomized to Indapamide 1. 5 mg OD vs Placebo – Target BP < 150 / 80 mm. Hg – Can receive Perindopril 2 – 4 mg OD vs placebo • Primary Endpoint: Fatal or non-fatal stroke • Secondary Endpoints : mortality , CVD death, cardiac death, stroke death , fatal / non-fatal CHF NEJM 358: 1887 (2008)
HYVET ––Heart HYVET Heart. Failure Subset Results • 64% RRR • NNT = 52 over 2 years NEJM 358: 1887 (2008)
Choosing an Antihypertensive Agent • Most important goal – get the BP down. üMore then likely will require ≥ 2 meds üFor patients who are at particular risk for symptomatic HF DIURETICS üFor patients with cardiovascular disease or significant CV risk factors DIURETIC ( ALLHAT) or ACEi (HOPE) üFor patients with LVH OPTIMAL TREATMENT ? ? ? Can consider ACEi or ARB or diuretic üAll other patients : path to HF leads thru HTN /LVH and /or MI INDIVIDUALIZE
Prevention of HF in Patients with Cardiovascular Disease • Prevention of ongoing ischemic damage üRisk factor modification ( smoking cessation , lipid-lowering , BP lowering , weight loss , optimization of diabetic management ) ü“Plaque Stabilization” with statin , ACEi , β-Blockers üRevascularization ( where practical AND possible) • Prevention / “reversal” of LV remodeling
ACEi Trials of Primary Prevention Trial SAVE SOLVD - P TRACE HOPE Entry Post MI , Asymptomatic Drug Captopril HF Result HF Hospitalization by 22% HF by 37% Asymptomatic Enalapril LVSD Post MI , EF Trandolapril HF by 29% <35% Hi Risk for CAD Ramipril HF by 23%
SOLVD Prevention Trial Death or Development of CHF Risk Reduction 29% p<0. 001 • Death or Development of CHF by 29% • Development of CHF by 37% • CHF hospitalizations by 44% N Engl J Med 1992; 327: 685 -91
PEACE Trial • Tested addition of ACEi (trandolapril) to usual therapy in stable cardiovascular patients with normal or mildly reduced LVEF plus other risk factors well controlled. • Primary Endpoint : CVD death , MI or need for revascularization - no additional benefit ( p = NS) • Secondary Endpoints: ü HF Hospitalization or death : 25% RR ; 3. 7% vs 2. 8% (p =0. 02) ü HF Hospitalization: 23% RR ; 3. 2% vs 2. 5% ( p = 0. 05 ) ü HF Death : 41% RR ; 0. 6% vs 0. 4% ; p = 0. 11
Prevention of HF in Patients with Diabetes Mellitus • Diabetes + cardiovascular disease at VERY HIGH RISK for development of heart failure • Diabetes in itself at HIGH RISK for HF development over the longterm. • Must focus on multiple risk factors üBP control critical : ACEi , ARB , Diuretics üSome evidence for glycemic control and HF eg HF 29% at 1 year post MI in diabetics with tight glycemic control
Conclusions / Implications • Development of HF still portends a grim prognosis • HF prevalence epidemic likely to continue • Caused mostly by aging , uncontrolled HTN § Apparent contribution from improved survival with HF § ? Contributions from MI survival per se • Effective therapies exist but are under-utilized § Especially for Primary Prevention of HF in HTN • Maximal medical therapy to prevent HF in patients with CV disease / post myocardial infarction also critical
Key Targets for Preventing HF • Prevention can be very successful üWeight maintenance , diet and physical activity üControl HTN and prevent LVH • ACEi , CCB , ARB , Thiazides üPrevent progression of ASLVD üPrevent CAD and MI ( 10 and 20 prevention ) üIn setting of CVS disease or diabetes mellitus, intensive risk-factor modification is warranted.