Stiffness after Total Knee Arthroplasty H Makhmalbaf MD

Stiffness after Total Knee Arthroplasty H. Makhmalbaf MD Consultant Orthopaedic Surgeon Assistant Professor Mashad University

Manipulation




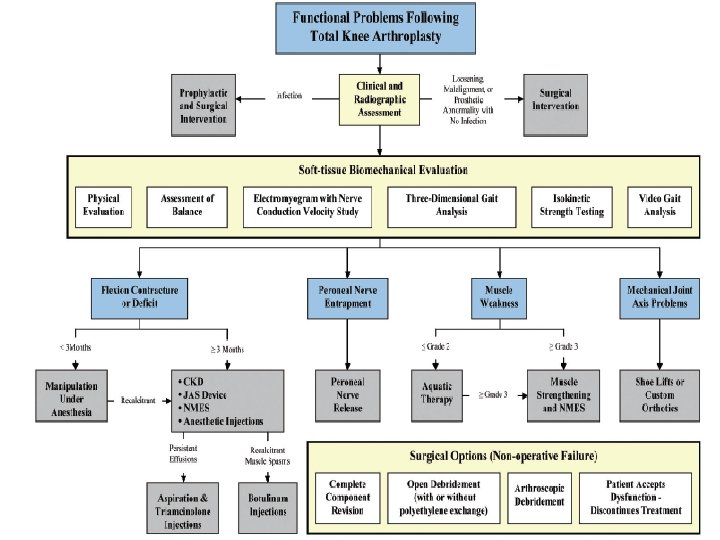
Functional problem & arthrofibosis following total Knee Arthroplasty • Thorsten M. Seyler Et al JBJS Am. 2007 • Small number of patients with persistent dysfunction that is difficult to treat • Persistent pain, Instability • & limitation of ROM • Decreased ROM , quality of life • Decreased patient satisfaction

Functional problems • • Continued dysfunction despite initial rehab. Noninvasive & invasive treatment Revision surgery If well-fixed, well-aligned prosthetic components will not benefit from a complete revision

Non operative • • • Rehabilitation protocols Static or dynamic splinting Injections Application of serial casts MUA

Invasive procedues • Arthroscopic debridment • Open debridement with or without PE exchange • Complete component revision

• • Careful radiographic & clinical evaluation Component loosening, malalignment Retained bone cement Indicated the need for revision surgery Infection: aspiration & culture Diagnosis & identify organism Proper antibiotic therapy & timely surgical treatment

Stiffness : AAOS • Is a debilitating complication of TKA • Is inadequate or smaller than expected ROM • If ROM is between 10 -90 & no pain or functional difficulties it is not a stiff knee • Difficulty getting out of a chair • Pain when climbing stairs • An observable stiff-knee gait

Stiffness: AAOS instructional course Lectures • Is closely related to pain • Patient’s experience in attempting to move the knee • Is closely related to patient’s motivation • Tolerate the pain to achieve the goal • No better results with CPM • Physiotherapy & Supervision lower risk

Preoperative Risk Factors • Limitation of range of motion • Underlying diagnosis • History of prior surgery

Stiffness after TKA: Laskin Rs J arthroplasty 2004 Jun • • Improper flexion-extension gap balancing Oversizing or malpositioning of components Inadequate femoral or tibial resection Excessive joint line elevation Creation of anterior tibial slope Inadequate resection of posterior osteophytes Tight posterior cruciate ligament

Postoperative Factors • • • Poor patient motivation Arthrofibrosis Infection Complex regional pain syndrome Heterotopic ossification

Management • • • Mobilizing the patient & Instituting physical therapy If fails: Manipulation Lysis of adhesions Revision arthroplasty

Management: • Closed manipulation is successful within 3 m. • Arthroscopic or open lysis after 3 months • Revision arthroplasty is preferred for stiffness from malpositioned or oversized components • If flexion is good initially but stiffness develops later , should be assessed for intrinsic as well as extrinsic causes.

Prevention & treatment of stiffness following TKA • • • Current Opinion in Orthopaedics Jan 2008 Range 1 -6% Poor preopeative ROM Poor intraoperative ROM Patella infera The best treatment is avoidance

Prevention of stiffness: Current Op. in Orth. 2008 • • • Proper patient motivation Physical therapy Careful surgical technique Careful ligamentous balancing Flexion-extension gap equalization Maintenance of posterior condylar offset

Management of Stiffness Following TKA J. Parvizi et al. JBJS Am 2006 • • • Stiffness is a disabling complication Exact etiology can not found in most cases Prevalence 1. 3% to 12% Preoperative ROM Contracture of extensor mechanism & Capsular structure

Management of stiffness • • • Lack of patient compliance Patient threshold for pain Technical factors such as: Overstuffing of the PFJ Mismatch of the flexion & extension gaps Inaccurate ligament balancing

Management of stiffness J. Parvizi et al • • • Component malpositioning Use of oversized components Joint-line elevation Excessive tightening of the extensor mechan. Underresection of the patella Anti-oxidants Or high dose of Vit. C

Stiffness & operation scars

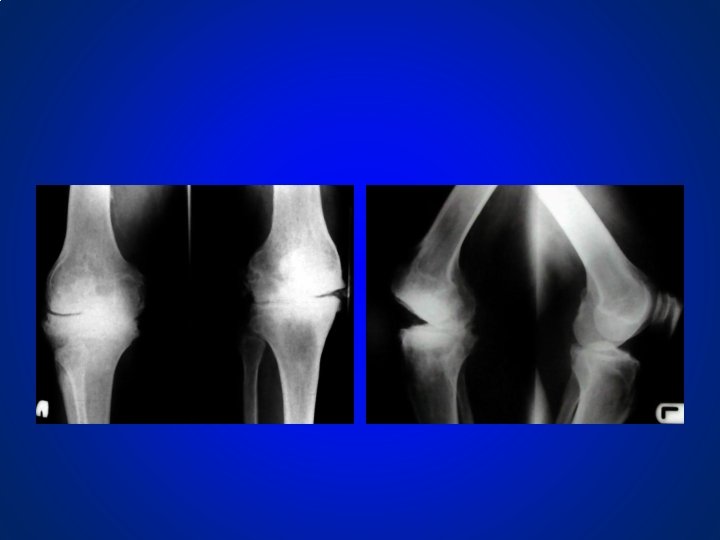
stiff knee , sever OA

Sever 3 compartment OA

Stiffness after TKA Maloney • • • The most important factor is pre-op ROM Design of prosthesis Evaluate patients X-ray Malrotation of components Stuffing of the PFJ Balance the PCL MUA up to 3 mo Open release of arthrofibrosis, PCL, med & lat gut Revision surgery

Previous operation & patellectomy

Severe OA

Sever pain & Stiffness

30 deg. ROM pre-op.

Sever OA & synovitis

PS Prosthesis 100 deg ROM • Osteoprotic bone • Adhesions in the suprapatella pouch • Patella subluxating • Release of adhesions • Patella realigned

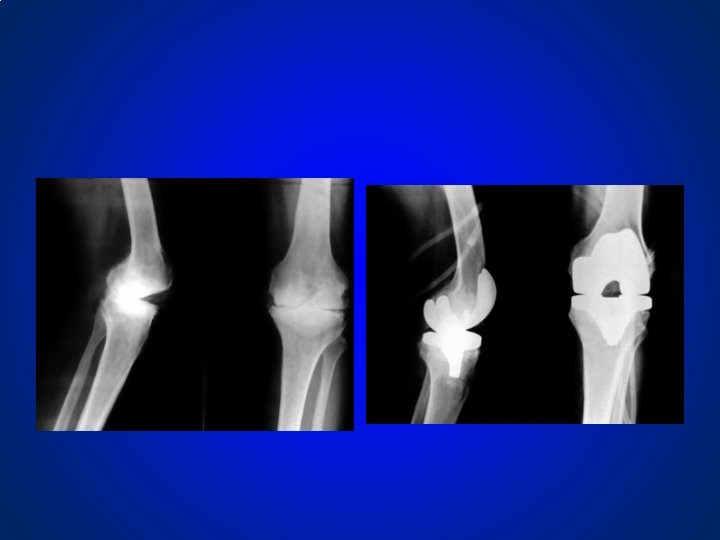
ROM after closure

Post op X-ray

Causes of stiff Knee: Hofmann • • ROM between 20 -70 Infection, Trauma, deformity, RA, HTO Fixed extensor mechanism Scarred recesses, patella ankylosis Patella baja, avulsion lig. patella Disruption quad. tendon. Patella fracture

Surgical technique: • • Synovectomy Release recesses Release lig. Patella Optional distal femur cut Quadriceps snip Sliding patella Tuberosity osteotomy

Stiff Knee post OP • Sufficient analgesia – Epidural catheter – PCA – Opioids & NSAID • Immediate CPM 0 -90 • Intensive physiotherapy

The best treatment is through Avoidance THANK YOU
- Slides: 41