Stephania Cormier Ph D scorm 1lsuhsc edu Outline







 Corticosteroids - inhaled Corticosteroids")

 Adrenaline (epinephrine)…. ephedrine β 1, β")
; selective β 2 agonists �")
 formoterol (FORADIL)")

 Administration: Oral, Inhaled, (rectal, IV) Pharmacokinetics: Onset: unknown")


: Onset: unknown Effect: unknown Duration: 24 h Warning: compliance poor!")


 Phenobarbital Rifampin Zafirlukast (Accolate) Increased metabolism Result Decreased montelukast levels")





 � Desensitization")



- Slides: 31
Stephania Cormier, Ph. D scorm 1@lsuhsc. edu
Outline Asthma Chronic Bronchitis Emphysema COPD Chronic bronchitis Emphysema
Asthma 23 million Year 12. 4 million “attack” 1. 8 million ER visits $21 billion health care costs & meds >5000 deaths
Asthma Normal Lung Efficient gas exchange Asthmatic Lung Inflammation Lower airways obstruction: inflammation, constriction, mucus Airway hyperresponsiveness Airway remodeling Chronic and PROGRESSIVE!
Immunopathogenesis of Asthma
Allergen Mast Cell Mediators • Histamine • Leukotrienes • Prostaglandins • Interleukins Inflammatory cell recruitment • Eosinophils Mediators • Cytokines • Leukocytes • macrophages • Interleukins BRONCHOSPASM Airflow Limitation Triggers • Cold air • Exercise • Tobacco smoke • Other smoke • Pollutants • Leukotrienes INFLAMMATION Bronchial hyperreactivity
COPD 12 million 4 th leading cause of death Year $26 billion / year >127, 000 deaths
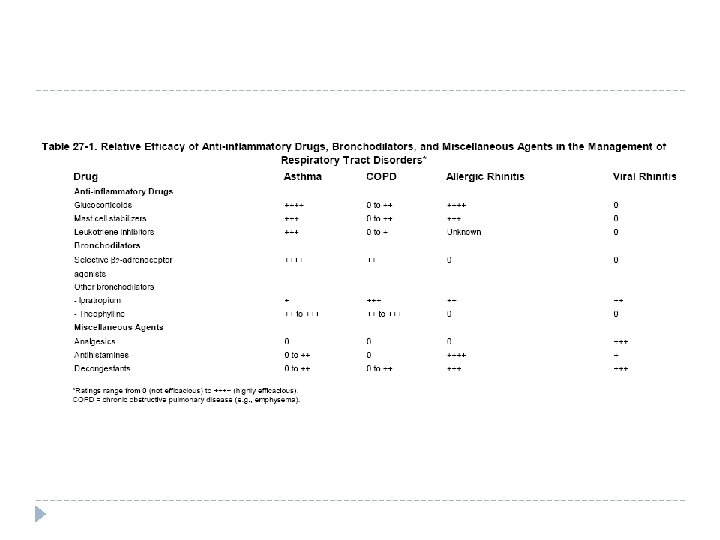
Medications Used for Asthma Relief Long-term Control Quick Relief (RESCUE) Corticosteroids - inhaled Corticosteroids – I. V. Cromolyns Short-acting β 2 -agonists Leukotriene modifiers Methylxanthines Long-acting β 2 -agonists Anticholinergics Sustained-release methylxanthines Antagonism of Ig. E • Control and prevent asthma symptoms • Make airways less sensitive to triggers and prevent inflammation that leads to an acute asthma episode (Immunomodulatory) • Taken on a daily basis • Provide relief of acute asthma episodes • Bronchodilators
β 2 Adrenergic Receptor Agonists Inflammatory Cells • Vasoactive amines • Lipid mediators • SMC hyperplasia
β 2 Adrenergic Receptor Agonists Relievers: short-acting (SABAs) Adrenaline (epinephrine)…. ephedrine β 1, β 2 Stimulates c. AMP production Terbutaline, albuterol, pirbuterol, bitolterol, levalbuterol (R -albuterol): β 2 > β 1 (220 - 400 x) Pharmacokinetics S-albuterol more (Ma-Huang): α, active at β 1 Onset: 5 -10 m Effect: 30 m Duration: 4 - 6 h Administration: inhaled, oral (terbutaline: SC) Side Effects: tremor, tachycardia – cardiac β 1 receptors.
β 2 Adrenergic Receptor Agonists � Controllers: long-acting (LABAs); selective β 2 agonists � Formoterol � Salmeterol � Pharmacokinetics � Onset: 15 - 30 m � Peak Effect: 22 h � Duration: 12 -24 h � Administration: inhaled � Side Effects: hypotension, hypertension, vascular headaches, tremors. Tolerance over time. � Warning: Warning increased chance of serious or fatal asthma
Salmeterol xinafoate (SEREVENT) formoterol (FORADIL)
Methylxanthines MOA Inhibits PDE High levels c. AMP SM relaxation Inhibits Ig. E release of mast cell mediators Competitive antagonist at adenosine (A 2) receptors Adenosine Bronchoconstriction Potentiate inflammatory mediator release Forms Theophylline, Caffiene (>) Synthetic: Aminophyline (>theophylline) , Dyphilline, Oxtriphyline
Methylxanthines Use: very limited (CNS stimulants) Administration: Oral, Inhaled, (rectal, IV) Pharmacokinetics: Onset: unknown Effect: 1 -2 h Duration: varies Side Effects: nausea, vomiting, anorexia Cardiac effects: sinus tachycardia, extrasystole, palpitations, arrhythmia Kidney: weak diuretic Skeletal Muscle: increase contractions
Anticholinergics � 1896: asthma cigarettes � � Stramonium Atropine, ipratropium, and tiotropium MOA: Competitive antagonists of muscarinic Ach receptors � Use: � � Asthma � � Chronic bronchitis/emphysema/COPD Administration: A: IV, I, T: inhalation, T: oral Pharmacokinetics: � not responsive to inhaled β 2 -adrenergic agonists inhaled β agonists are contraindicated (i. e. cardiac ischemia or arrhythmia) Onset: 5 -15 m Effect: 1 -2 h Duration: 4 -5 h Side Effects: dryness of mouth and airway, headache. Rarely: tachycardia, dry eyes/blurred vision, urinary retention
Corticosteroids � MOA: gene regulation Anti-inflammatory � Immunosuppression � � Administration � Inhaled: beclomethasone, triamcinolone, fluticasone, budesonide, flunisolide, mometasone � � Side Effects: Oropharyngeal candidiasis, dysphonia oral (most potent): dexamethasone, prednisone Side Effects: mood disturbances, increased appetite, impaired glucose control in diabetics, and candidiasis � Long-term use: bone resorption � Inhaled Prednisone �
Corticosteroids Pharmacokinetics (inhaled): Onset: unknown Effect: unknown Duration: 24 h Warning: compliance poor!
Cromolyns: Mast Cell Stabilizers Cromolyn, nedocromil MOA: Alter fxn of delayed Clchannels (inhibiting their activation) Blocks release of inflammatory mediators: mast, eosinophil, basophil, lymphocyte Use: prophylactic therapy for mild-moderate allergic asthma Allergic rhinitis (C) Administration: Inhalation Pharmacokinetics: Side Effects: Effect: wks C: safest of all increased coughing, wheezing Age matters: Cromolyn: children, adolescents Nedocromil: ≥ 12 yoa
Leukotriene Modifiers � Strategies � Leukotriene-Synthesis Inhibitors � � Leukotriene Receptor Antagonists � � � “responder” mild chronic asthma allergic rhinitis Administration: Inhalation (, oral (M, Z) Pharmacokinetics: � Montelukast, zafirlukast Use: � � Zileuton Onset: 3 -6 h Effect: 4 h Duration: 24 h Side Effects: Churg-Strauss syndrome … happens in the un. LUc. Kiest
Drug Interactions Montelukast (Singulair) Phenobarbital Rifampin Zafirlukast (Accolate) Increased metabolism Result Decreased montelukast levels Drugs MOA Aspirin: Zafir Erythromycin: Zafir Tolbutamide, phenytoin, carbamazepine: levels Warfarin: levels Zileuton (Zyflo) Drugs: levels Propranolol Theophylline Warfarin
Antagonism of Ig. E � Anti-Ig. E: omalizumab � 95% humanized � High cost >$10 K/yr � Use: moderate-tosevere persistent asthma � Administration: SC Pharmacokinetics: Pk Plasma: 7 -8 d Duration: 26 d � Side Effects: injectionsite reaction, infections, anaphylaxis, cancer
Drug Delivery Metered Dose Inhaler Nebulizers Dry Powder Inhaler Injection
MDI
Monotherapy
Combi-therapies � Budesonide + formeterol fumerate � Refer to each component � Moderate-severe uncontrolled asthma � Fluticasone � Refer proprionate + salmeterol xinofate to each component � Moderate-severe uncontrolled asthma
Potential New Therapies for Asthma � Vaccines (DNA vaccine; Mycobacterium, Cp. G) � Desensitization (allergen-specific immunotherapy including recombinant gene-manipulated antigens and peptides) � Cytokine modulators (gene, protein) Anti IL-4, IL-5, IL-13 � IL-12 � IL-10 � � Selective phosphodiesterase inhibitors � Selective tryptase inhibitors � Potassium channel activators � Adhesion molecule inhibitors � Gene therapy Targeting susceptibility genes � Targeting polymorphism of receptors for drugs � � Others
Step-wise Approach to Asthma Therapy
Staging COPD - GOLD
Gq-coupled receptor signaling in airway smooth muscle Billington et al. Respiratory Research 2003, 4: 2