Status of Drug Trials for Rett Syndrome Jeffrey













 in children with Rett syndrome")
 in children with Rett syndrome")
 n n n Treatment with")
 n PHASE 2: Double blind,")
 n n All 30 subjects")
 in children with Rett syndrome")
 in RTT n")

, Aleksandra Djukic n Phase II, Open Label, Dose-escalating study")
 Stopped after 10 people completed trial n Results: n")
, Bruria Ben Zeev n n Phase II,")








, Aleksandra Djukic n n Phase II, Open Label, Dose-escalating study")







: E 1 -4.")


![Neuren compound NNZ-2566 Chemically modified IGF-I [1 -3] n More similar to compound used](https://slidetodoc.com/presentation_image_h/7480ba499e94fd0668160222f7b0fb04/image-45.jpg "Neuren compound NNZ-2566 Chemically modified IGF-I [1 -3] n More similar to compound used")
![Phase 2 Study of Two Dose Levels of NNZ-2566 ([1 -3] IGF-1 analog) Cohort](https://slidetodoc.com/presentation_image_h/7480ba499e94fd0668160222f7b0fb04/image-46.jpg "Phase 2 Study of Two Dose Levels of NNZ-2566 ([1 -3] IGF-1 analog) Cohort")





: E 1 -4.")




- Slides: 56
Status of Drug Trials for Rett Syndrome Jeffrey L. Neul M. D. , Ph. D. Division Chief of Child Neurology Department of Neurosciences University of California, San Diego Rady Children’s Hospital – San Diego
Disclosures n n n National Institutes of Health Rettsyndrome. org n Grant support n Medical Advisory Board Rett Syndrome Research Trust n Grant support Neuren Pharmaceuticals n Research support Newron Pharmaceuticals n Consulting Eloxx Pharmaceuticals n Research support
Potential therapeutic levels Knowledge Symptomatic Disease specific Disease modifying Disease reversing
Serotonin in Rett syndrome • Important neurotransmitter involved in many clinical features • • Control of breathing Mood Anxiety Decreased in people with RTT and mouse model dopamine serotonin dopamine norepinephrine serotonin
Sarizotan • • 5 HT 1 a agonist/D 2 antagonist Previous evaluated to treat schizophrenia or Parkinson Disease Improved breathing in RTT mice Newron Pharmaceuticals
A RANDOMIZED, DOUBLE-BLIND, PLACEBO-CONTROLLED, SIXMONTH STUDY TO EVALUATE THE EFFICACY, SAFETY AND TOLERABILITY OF SARIZOTAN IN PATIENTS WITH RETT SYNDROME WITH RESPIRATORY SYMPTONS n n n n n Phase 2/3 Double Blind, 2 dose levels + placebo 6 mo drug exposure + 6 mo blind extension Primary Outcome: Improvement in apneas Secondary Outcome: Safety and broad signals of efficacy Inclusion: Clinical Rett syndrome + MECP 2 mutation, + breathing abnormalities Age: Over 13 yo Goal enrollment: 90 (n=30 in each drug level) Sites n n n n University of California, San Diego University of Alabama-Birmingham Baylor College of Medicine Rush University, Chicago Sienna, Italy India Anticipated Start Date (at UCSD): Summer 2016
Mitochondrial abnormalities in Rett syndrome • • Mitochondria are “energy factories” of the cell Evidence of abnormal mitochondria in RTT • • Elevated serum and CSF lactate and pyruvate in some patients Abnormal mitochondria morphology Abnormal expression of proteins involved in mitochondrial function Hypothesis: Improving mitochondrial function will improve clinical features in RTT
Mitochondrial abnormalities in Rett syndrome: Triheptahoin • • C 7 fatty acid metabolized to C 4 and C 5 ketone bodies Provides alternative energy source to brain Improves mitochondrial function Improved seizures in Glut 1 deficiency • • • Improved metabolic profile Better motor performance Improved survival Preclinical treatment in RTT mouse model Park et al, PLOSOne, 2014
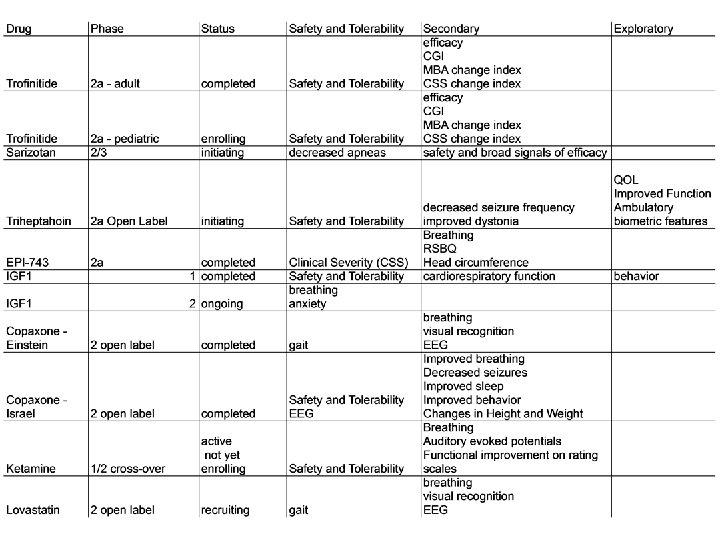
Triheptahoin clinical trial Emory University, Daniel Tarquinio n n Phase 2 a, open label study of 10 subjects Clinical RTT and mutation in MECP 2 n n n Primary outcome: Safety and Tolerability Secondary outcomes: n n n Improvement in seizure frequency Improvement in dystonia severity Exploratory outcomes: n n >4 seizures per month, >4 dystonic episodes per month Quality of life Improved function EEG and Ambulatory biometric devices (autonomic function, movement, oxygen saturation, electrodermal activity) Not yet enrolling
Triheptanoin Timeline
EPI-743 Siena, Italy n EPI-743 is a modified Co. Q 10 preparation n n Improves mitochondrial function Phase IIa, randomized, placebo controlled study in RTT with MECP 2 mutations Goal enrollment: N=24, <3 yo 6 mo treatment Outcome measures n n Primary: Improvement in clinical severity Secondary n n Completed n n Breathing Rett Syndrome Behavioral Questionaire Head circumference Improved head circumference Future: Edison Therepeutics considering future trials
Potential therapeutic levels Knowledge Symptomatic Disease specific Disease modifying Disease reversing
Disease modifying therapies Male Mecp 2 mice treated with tripeptide from N-terminus of IGF-I [1 -3] = Gly-Pro-Glu
IGF-I trials in Rett syndrome n Full-length IGF-I (mecasermin) in children with Rett syndrome n n Boston Children’s Hospital Trofinetide (NNZ-2566) in adults with Rett syndrome Baylor College of Medicine, Houston TX n University of Alabama-Birmingham n Gillette Children’s Hospital, St. Paul MN n
IGF-I trials in Rett syndrome n Full-length IGF-I (mecasermin) in children with Rett syndrome n n Boston Children’s Hospital Trofinetide (NNZ-2566) in adults with Rett syndrome Baylor College of Medicine, Houston TX n University of Alabama-Birmingham n Gillette Children’s Hospital, St. Paul MN n
Children’s Hospital Boston rh. IGF-1 clinical trial (NCT 01253317) n n n Treatment with full length IGF 1 (Mecasermin), initiated December 2010 n Phase I: open-label escalating subcutaneous twice daily doses (40, 80, and 120 ug/kg) for 4 weeks to assess safety Primary outcome: Safety Secondary: improvement in cardiorespiratory function as measured by respiratory inductance plethysmography and electrocardiogram Exploratory evaluation: Function, behavior, biomarkers Results: safe and some signals of efficacy
Children’s Hospital Boston rh. IGF-1 clinical trial (NCT 01253317) n PHASE 2: Double blind, placebo controlled, cross over, single dose study n n 30 people Randomized to drug or placebo n n 20 weeks exposure 10 week wash out 20 week exposure Primary outcomes-breathing, anxiety
Children’s Hospital Boston rh. IGF-1 clinical trial (NCT 01253317) n n All 30 subjects in the original cohort have completed the trial (entire study). US FDA recommended in early 2015 to increase the cohort size to at least 47 as well as to add more sites. n n n response to the request for considering the phase 2 trial pivotal. Because of drug supply issues, the expansion of the trial to two other sites (Chicago and Greenwood) and 17 additional subjects never took place. Ipsen requested to perform “interim” analyses of the original 30 -subject cohort. If the data are strong, they would prefer to move forward to a new phase 3 trial rather than expanding the current trial. The FDA also requested validation of the primary endpoint, the ADAMS. This is in process, with the first step already completed.
IGF-I trials in Rett syndrome n Full-length IGF-I (mecasermin) in children with Rett syndrome n n Boston Children’s Hospital Trofinetide (NNZ-2566) in adults with Rett syndrome Baylor College of Medicine, Houston TX n University of Alabama-Birmingham n Gillette Children’s Hospital, St. Paul MN n
Treatments to increase BDNF n Decreased Brain Derived Neurotrophic Factor (BDNF) in RTT n n BDNF is a growth factor important for neuronal growth and function Increasing BDNF in brain of mouse model improves survival Chang et al, Neuron, 2006
Copaxone trials n n Copaxone: An artificial copolymer of peptide pool composed of random sequence of 4 amino acids : glutamine, lysine, alanine and serine Used for >20 yrs for Multiple Sclerosis n n Elevated serum BDNF levels were detected in MS patients only during copaxone Increases BDNF in brain of RTT mice Control Copaxone Ben-Zeev et al, 2011
Copaxone trials-NYC n Montefiore (NYC), Aleksandra Djukic n Phase II, Open Label, Dose-escalating study in RTT with MECP 2 mutations n Need to be able to walk Goal enrollment: N=20, >10 yo n 24 week treatment, with dose escalation n Outcome measures n n Primary: Gait n Secondary n n n Breathing Visual recognition using eye tracking device EEG abnormalities
Copaxone trials-NYC n Montefiore (NYC) Stopped after 10 people completed trial n Results: n n Gait: 7/10 improved gait speed (13. 1%-95. 2%) n Breathing: 5/10 showed improved breathing holding index n Visual recognition: 5/7 showed improvement in cognitive assessment of face stimuli n EEG: Epileptiform discharges decreases in 4/4 who had them at baseline
Copaxone trials-Israel n Sheba Medical Center (Israel), Bruria Ben Zeev n n Phase II, Open Label, Dose-escalating study in RTT with MECP 2 mutations and EEG abnormalities Goal enrollment: N=10, 5 -15 yo 24 week treatment, with dose escalation Outcome measures n Primary n n n Safety Improvement in EEG abnormalities Secondary n n n Improved breathing Decreased seizures Improved sleep Improved behavior Changes in Height and Weight
Copaxone trials-Israel n 10 people recruited n n n One had increase in seizure frequency and decided to stop the trial 4/10 mild irritation at injection site After 3 mos one subject had flushing, mild generalized edema tremor and breath holding immediately after injection n n 2 wks later 2 more subjects reported similar (immediate) but more prolonged and prominent response after injection n Subsequent injections ok, continued on study one subsided spontaneously after few hours of observation in ER One had significant generalized edema , breathing difficulties followed by seizure and requiring adrenaline injection by paramedic and hospitalization, remission after 24 hours Report to IRB – Decision to hold study and investigate SAE
Copaxone trials-Israel Known Copaxone Side effects : n n Transient injection site reaction : erythema, induration, pruritus and pain lasting up to few hours (20 -60% ) Immediate post injection systemic reaction (IPISR) - (1016%) at least two of the following: flushing, chest pain, palpitations, anxiety, dyspnea, constriction of the throat, and urticaria - generally transient, self-limited (20 min) symptoms that do not require treatment- continuing treatment in many cases without recurrence and existing desensitization protocols Dyspnea, chest pain, transient systemic reaction (flushing, dizziness) and fatigue were observed in 7– 14% of pediatric patients treated with Copaxone Case reports : “anaphylactic” reaction with diffuse pruritic exanthema , hypotension, dyspnea , bronchospasm and angioneurotic edema immediately after injection requiring intervention
Copaxone trials-Israel n IRB Review n n Evaluation of events and input on safety from Montefiore Decision to reopen study 4 more subjects recruited 3 months into the study n similar severe response in one subject Edema, flushing, prolonged breath holding and possibly seizure immediately after injection –severe enough to call paramedic team and transfer to close ER – Spontaneous remission in 1 -2 hours n Response frightening enough to very experienced parents n n IRB review of SAE – decided to stop study
Copaxone trials-Conclusion n Montifiore Safe n Positive signals of efficacy n n Israel n n Multiple SAE Future - uncertain
Ketamine Treatment for RTT • • Ketamine is a NMDA antagonist used for sedation (amnestic) Evidence for efficacy at low doses for major depression Evidence of increased cortical neuronal excitability in RTT Preclinical treatment in mice • • • Delayed onset of breathing problems Improved sensory gating Improved survival Kron et al. , 2012; Mather et al. , 2014, Patrizi et al, 2014
Ketamine Treatment for RTT • • David Katz, Case Western Reserve University and Sumit Parikh, Cleveland Clinic Phase I/II placebo-controlled randomized crossover Goal enrollment: 30 Inclusion • • Clinical RTT and MECP 2 mutation Evidence of breathing abnormality Primary outcome: Safety Exploratory • • • Breathing Auditory evoked potentials Functional improvement on rating scales
Ketamine trial design n n n 4 in-hospital treatment sessions, each with an overnight stay, separated by 1 month between sessions During each treatment session, subjects will receive either placebo (one session) or one of 5 possible ketamine doses; treatments will be administered by i. v. infusion over 40 minutes Ordering of the treatments will be randomized for each patient, and patients earlier in the study will receive lower doses to ensure safety Parents will be asked to not be present during infusion and for 2 hours following to improve blinding Outcomes will be compared before and after drug infusion and between the placebo and drug administrations Status: Active but not yet recruiting
Targeting Cholesterol Metabolism n Treatment of RTT mice with statin drug Improved survival n Improved locomotor function n
Lovastatin-NYC n Montefiore (NYC), Aleksandra Djukic n n Phase II, Open Label, Dose-escalating study in RTT with MECP 2 mutations and can walk Goal enrollment: N=20, >3 yo 32 week treatment, with dose escalation Outcome measures Primary: Gait n Secondary n n n Breathing Visual recognition using eye tracking device EEG abnormalities Quality of Life Recruiting subjects
Reversibility in mouse model Mecp 2 Conditional Rescue 1 2 No Cre = “OFF” lox. P STOP 2 Mecp 2 Conditional Rescue 1 lox. P 3 4 Cre = “ON” lox. P 3 4 Guy et al. , Science 2007
Questions for discussion n n How can we improve existing outcome measures? What could be additional outcome measures? What is the best trial design? n Open label first? n Placebo controlled first? What other features would improve trial design?
Acknowledgements n n n Walter Kaufmann, Greenwood Genetics Daniel Tarquinio, Emory University, Atlanta GA Aleksandra Djukic, Children’s Hospital at Montefiore, Albert Einstein Medical School, New York, NY Bruria Ben-Zeev, Sheba Medical Center, Israel David Katz, Case Western University, Cleveland, OH Rett Syndrome Natural History Study – Alan Percy n n n NIH Rettsyndrome. org Rett Syndrome Research Trust
Thank you
Gene therapy in RTT? n Theoretical concern that adding normal copy of gene to all cells would cause problems Correction in ½ cells to 1 x n Overexpression in ½ cells to 1 x n n Difficulty getting gene into CNS
Cell-based therapy in RTT? BMT worked presymptomatically Required CNS irradiation to work
BMT – presymptomatic male animals Andrew Pieper UTSW University of Iowa Nature, 2015 May 21; 521(7552): E 1 -4.
Restore Mecp 2 expression genetically Nature, 2015 May 21; 521(7552): E 1 -4.
BMT Conclusions BMT did not ameliorate symptoms in symptomatic female RTT mice n BMT did not rescue survival or other phenotypes in pre-symptomatic male RTT mice n Genetic restoration of Mecp 2 expression in microglia did not rescue phenotypes n Me. CP 2 function may play important role in microglia function, but does not seem sufficient to reverse disease n
Conclusions n RTT is a disease that has a number of treatment options Disease course in models can be modified n Disease in models can be reversed n Number of existing and developing ideas for treatment n Potential for great impact n Ongoing needs n n Improved functional outcome measures n Communication n Hand skills n Ambulation
Neuren compound NNZ-2566 Chemically modified IGF-I [1 -3] n More similar to compound used in animal study than full-length IGF-I n Lacks insulinotropic and growth effects n n Concern given risk of metabolic syndrome in mice Orally active (strawberry flavored liquid) n Neuroprotective and seizure preventing in animal stroke and traumatic models n Currently in clinical trials (DOD funded) for traumatic brain injury n
Phase 2 Study of Two Dose Levels of NNZ-2566 ([1 -3] IGF-1 analog) Cohort 0 2: 1 Randomization 35 mg/kg BID or Placebo 14 Days Treatment N=9 Cohort 1 2. 1 Randomization 35 mg/kg BID or Placebo 28 days treatment Cohort 2: 1 Randomization n n 70 mg/kg BID or Placebo N=18 2 28 days of treatment N=29 N=56, Ages 15. 9 -44. 2 (mean 25. 3) Primary Outcome: Safety/Tolerability Secondary Outcome: Efficacy Funded by Neuren Pharmaceuticals (Sponsor) and the International Rett Syndrome Foundation 46
70 mg/kg BID Dose of NNZ-2566 Demonstrates Evidence of Efficacy Subject-Level Score Top 3 Concerns MBA Change Index n Achieved its primary endpoint - both dose levels of NNZ-2566 were welltolerated after 28 days of treatment and no safety concerns were identified. Higher dose exceeded the pre-specified criteria for improvement in core efficacy measures compared with placebo on group and subject level analysis CGI-I n Least Squares mean change from baseline to Day 26 (Direction of benefit = Up) *modified intent to treat group, n=55
Next steps: A Safety Study of NNZ-2566 in Pediatric Rett Syndrome n Double-blind, placebo controlled doseranging study n n n n 3 dose levels Similar in design to first trial (RTT-001) Younger age range (5 -15 yo) Clinical RTT and MECP 2 mutation Cannot have QTc prolongation Primary outcome: Safety Secondary outcome: Signals of efficacy Goal enrollment: >76
Next steps: A Safety Study of NNZ-2566 in Pediatric Rett Syndrome d 1 d-7 Screen d 14 d 21 d 28 d 42 d 54 Placebo d 66 50 mg/kg BID 100 mg/kg BID 200 mg/kg BID
Next steps: A Safety Study of NNZ-2566 in Pediatric Rett Syndrome n University of Alabama-Birmingham n n Greenwood Genetics Center, SC n n n n n Enrolling University of California, San Diego n n Enrollment started Plan to start enrolling June 2016 University of California, San Francisco Baylor College of Medicine Boston Children’s Hospital Rush University, Chicago IL Gillette Children’s Hospital, St. Paul, MN Colorado Children’s Hospital Cincinnati Children’s Hospital Vanderbilt University, Nashville, TN
Gene correction: Mutation specific therapy 36% of RTT-causing MECP 2 mutations are nonsense mutations n Compounds currently in clinical trials that “read-through” nonsense mutations n Trends in Molecular Medicine Volume 18, Issue 11 2012 679 - 688
Restore Mecp 2 expression genetically Nature, 2015 May 21; 521(7552): E 1 -4.
Deep brain stimulation Transcranial magnetic stimulation leads to increased lifespan and decreased anxiety n Striatal DBS: improved motor function n Fornix DBS: improved memory n
Is there a sodium channel defect in Mecp 2 Null/Y mice? n n n Most isolated cases of LQTS are due to loss of function in potassium channels. LQTS-3 is caused due to gain of function in sodium channels and propranolol is not very effective in preventing arrhythmias LQTS-3 is associated with an increased persistent Na+ current
Persistent INa in RTT cardiomyocytes
Acute Na-channel inhibition corrects long QTc and prevents cardiac arrhythmias n Acute Treatment with Na-Channel blockers but not beta-blockers decrease QTc and VT induction