STAPHYLOCOCCI INTRODUCTION Staphylococci are Grampositive spherical bacteria arranged

STAPHYLOCOCCI

INTRODUCTION Staphylococci are Gram-positive spherical bacteria arranged in microscopic clusters resembling grapes Staphyloccocci – Greek word “stapyle” =bunch of grapes and “kokkos”= a berry. This group includes a major human pathogen and skin commensals

Grouping for Clinical Purposes 1. Coagulase positive Staphylococci Staphylococcus aureus- major pathogen 2. Coagulase negative Staphylococci Staphylococcus epidermidis Staphylococcus saprophyticus Staphylococcus hemolyticus

Staphylococcus aureus Major human pathogen Habitat - S. aureus colonizes mainly the nasal passages, but it may be found regularly in most other anatomical sites, including skin, oral cavity and gastrointestinal tract Source of organism - can be infected human host and carrier , directly or through fomite

Nearly all strains of S. aureus produce the enzyme coagulase S. aureus should always be considered a potential pathogen

Important phenotypic characteristics of S. aureus Gram-positive, cluster-forming cocci facultative anaerobe -fermentation of glucose produces mainly lactic acid Catalase positive, Coagulase positive Golden yellow colony on agar Normal flora of humans found on nasal passages, skin and mucous membranes Pathogen of humans: causes suppurative infections, food poisoning, toxic shock syndrome

Virulence factors of S. aureus Enzymes: Coagulase – coagulates plasma and blood; produced by 97% of human isolates; diagnostic Hyaluronidase – digests connective tissue Staphylokinase – digests blood clots DNase – digests DNA Lipases – digest oils; enhances colonization on skin Penicillinase – inactivates penicillin 9
 – lyse red")
Virulence factors of S. aureus Toxins: Hemolysins (α, β, γ, δ) – lyse red blood cells Leukocidin – lyses neutrophils and macrophages Enterotoxin – induce gastrointestinal distress Exfoliative toxin – separates the epidermis from the dermis Toxic shock syndrome toxin (TSST) – induces fever, vomiting, shock, systemic organ damage 10

11

Natural history of disease Neonates, children, adults -intermittently colonised by S. aureus Usual sites - skin, nasopharynx, perineum Breach in mucosal barriers - can enter underlying tissue- Characteristic abscesses Disease due to toxin production

DISEASES Due to direct effect of organism Local lesions of skin Deep abscesses Systemic infections Toxin mediated Food poisoning Toxic shock syndrome Scalded skin syndrome
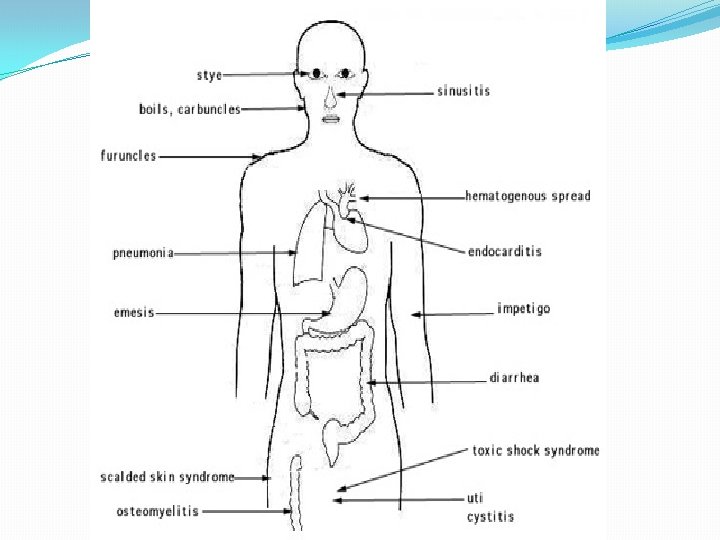

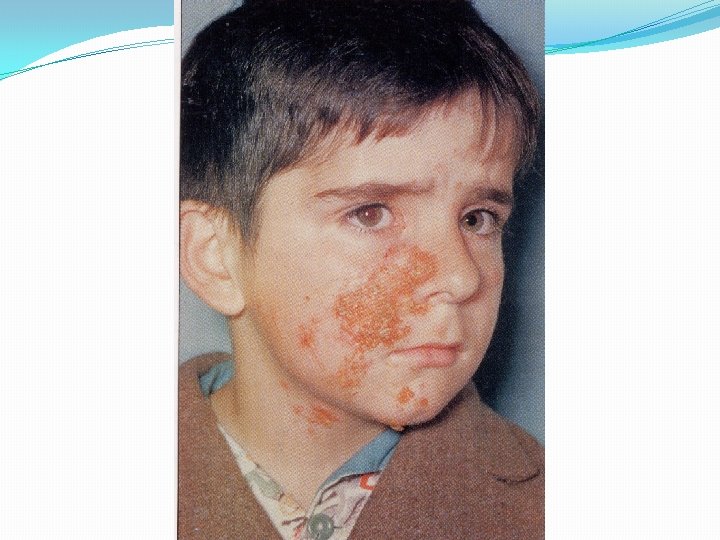
Staphylococcal Disease Range from localized to systemic Localized cutaneous infections – invade skin through wounds, follicles, or glands Folliculitis – superficial inflammation of hair follicle; usually resolved with no complications but can progress Furuncle – boil; inflammation of hair follicle or sebaceous gland progresses into abscess or pustule Carbuncle – larger and deeper lesion created by aggregation and interconnection of a cluster of furuncles Impetigo – bubble-like swellings that can break and peel away; most common in newborns 15

Cutaneous lesions of S. aureus 16

Styes Abscess

Systemic infections Osteomyelitis – infection is established in the metaphysis; abscess forms Bacteremia – primary origin is bacteria from another infected site or medical devices; endocarditis possible 19

Staphylococcal osteomyelitis in a long bone 20

Toxigenic disease Toxic shock syndrome – toxemia leading to shock and organ failure 21

Effects of staphylococcal toxins on skin 22

Toxic Shock Syndrome Toxin Superantigen Non-specific binding of toxin to receptors triggers excessive immune response

TSS Symptoms 8 -12 h post infection Fever Susceptibility to Endotoxins Hypotension Diarrhea Multiple Organ System Failure Erythroderma (rash)

Staphylococcal food poisoning Due to production of entero toxins- heat stable entero toxin acts on gut Produces severe vomiting following a very short incubation period Resolves on its own within about 24 hours

Scalded skin syndrome Disease of young children Mediated through minor Staphylococcal infection by ‘epidermolytic toxin’ producing strains Mild erythema and blistering of skin followed by shedding of layers of epidermis

Antibiotic sensitivity pattern Very imp. In Pt. Management Antibiotic resistance mechanisms 1. Β-lactamase production - plasmid mediated Has made S. aureus resistant to penicillin group of antibiotics - 90% of S. aureus B lactamase stable penicillins (cloxacillin, methicillin) used
 Has made S. aureus resistant to")
2. Alteration of penicillin binding proteins- (Chromosomal mediated) Has made S. aureus resistant to β-lactamase stable penicillins (MRSA) 10 -20% S. aureus are resistant to all Penicillins and Cephalasporins Vancomycin is the drug of choice

MRSA detected in the lab using methicillin In Japan emergence of VIRSA(vancomycin intermediate resistant S. aureus) No effective antibiotics for successful treatment

DIAGNOSIS �In all pus forming lesions �Gram stain and culture of pus �In all systemic infections �Blood culture �In infections of other tissues �Culture of relevant tissue or exudate

Staphylococcal Lab Identification & Diagnostic Tests � Microscopic � Lab isolation � Coagulase positive • ü S. aureus
 Staphylococcus aureus")
Mannitol Salt Agar (MSA) Staphylococcus aureus

Differential Characteristics Catalase 2 H 2 O 2 + 2 H 2 O Streptococci vs. Staphylococci

Catalase POS Staphylococcus Catalase NEG

Differential Characteristics S. aureus Coagulase Fibrinogen Fibrin
 Coagulase testi) Slide coagulase test- Positive. ii) Tube coagulase test- Positive. SLIDE COAGULASE")
2) Coagulase testi) Slide coagulase test- Positive. ii) Tube coagulase test- Positive. SLIDE COAGULASE TEST TUBE COAGULASE TEST

Staphylococcus aureus Coagulase POS Coagulase NEG

Treatment Drain infected area Deep/metastatic infections Semi-synthetic penicllins Cephalosporins Erythromycin, Clindamycin Endocarditis semi-synthetic penicillin + an aminoglycoside MRSA: Vancomycin

Prevention Carrier status prevents complete control Proper hygiene, segregation of carrier from highly susceptible individuals Good aseptic techniques when handling surgical instruments Control of nosocomial infections

2. Staphylococcus epidermidis Skin commensal Has predilection for plastic material Ass. With infection of IV lines, prosthetic heart valves, shunts Causes urinary tract infection in cathetarised patients Has variable ABS pattern Treatment should be aided with ABST

3. Stapylococcus saprophyticus Skin commensal Imp. Cause of UTI in sexually active young women Usually sensitive to wide range of antibiotics
- Slides: 42