Standard reporting in infertile patients color doppler uterine


: Ovarian Volume Structure Relation to the uterus R/O of PCO")


: Ovarian Volume Structure Relation to the uterus R/O of PCO")

: Ovarian Volume Structure Relation to the uterus R/O of PCO")

: Ovarian Volume Structure Relation to the uterus R/O of PCO")
: Ovarian Volume Structure Relation to the uterus R/O of PCO")

: Ovarian Volume Structure Relation to the uterus R/O of PCO")
 Functional ovarian cysts:")
: Ovarian Volume Structure Relation to the uterus R/O of PCO")

: Ovarian Volume Structure Relation to the uterus R/O of PCO")












 1. Endometrial thickness in greatest AP dimension")
 zone 2 (outer hyperechogenic zone) zone 3(inner hypoechogenic zone)")
 1. Endometrial thickness in greatest AP dimension")
. Absent = 0 Present =")

- Slides: 37
Standard reporting in infertile patients, color doppler, uterine BPP E, Keshavarz MD Assistant Professor of Radiology SBMU
Baseline US Between days 1 and 5 of menstrual cycle: Uterus(size, shape, endometrium, any mass lesion and its relation to the endometrium) Ovaries……
Baseline US Ovaries(report separately): Ovarian Volume Structure Relation to the uterus R/O of PCO Any mass lesion AFC Any echofree lesion larger than 15 mm Ovarian stromal perfusion
Ovarian Volume In combination with AMH : Future fertility chance Larger volume: Higher risk of developing OHSS More follicles Higher clinical pregnancy rate
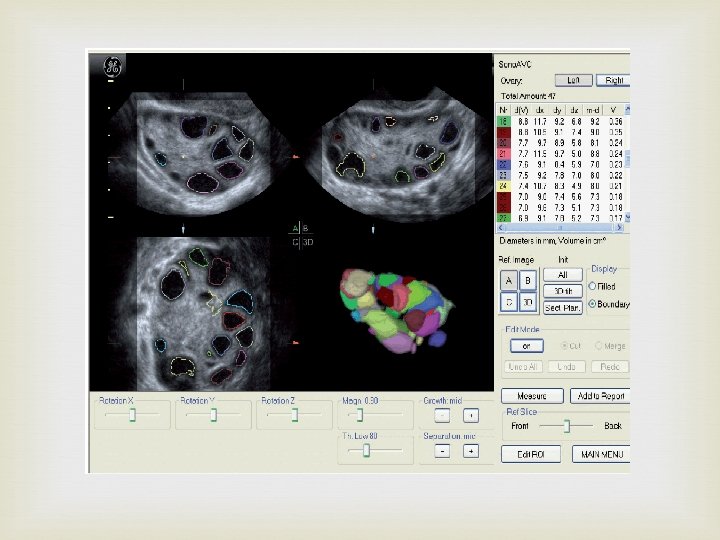
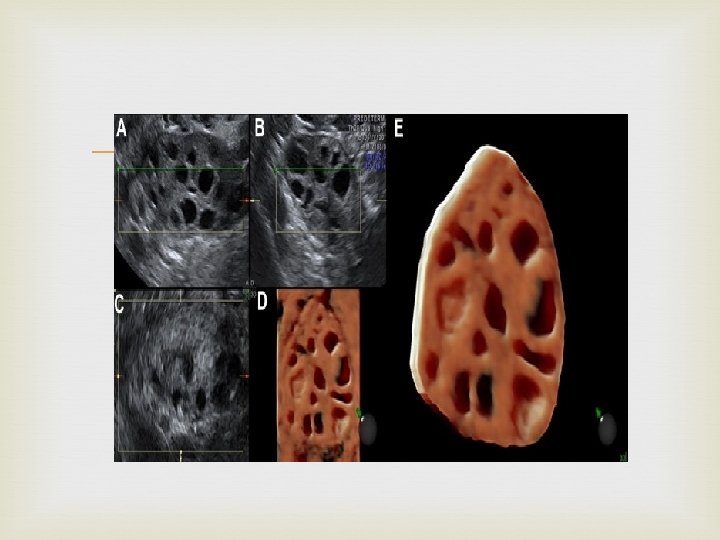
Ovarian Volume The best technique is 3 D VOCAL Strictly speaking, the ellipsoid defined with this formula is not prolate
Baseline US Ovaries(report separately): Ovarian Volume Structure Relation to the uterus R/O of PCO Any mass lesion AFC Any echofree lesion larger than 15 mm Ovarian stromal perfusion
Structure PCO versus multi follicular/multi cyctic ovaries PCO: 12 or more follicles measuring 2– 9 mm in diameter, subjective impression of increased stromal echogenicity Multifollicular ovary: 6 or more follicles, usually 4– 10 mm in diameter, with normal stromal echogenicity
Baseline US Ovaries(report separately): Ovarian Volume Structure Relation to the uterus R/O of PCO Any mass lesion AFC Any echofree lesion larger than 15 mm Ovarian stromal perfusion
Relation to the uterus Adhesion Previous surgery Endometriosis
Baseline US Ovaries(report separately): Ovarian Volume Structure Relation to the uterus R/O of PCO Any mass lesion AFC Any echofree lesion larger than 15 mm Ovarian stromal perfusion
Baseline US Ovaries(report separately): Ovarian Volume Structure Relation to the uterus R/O of PCO Any mass lesion AFC Any echofree lesion larger than 15 mm Ovarian stromal perfusion
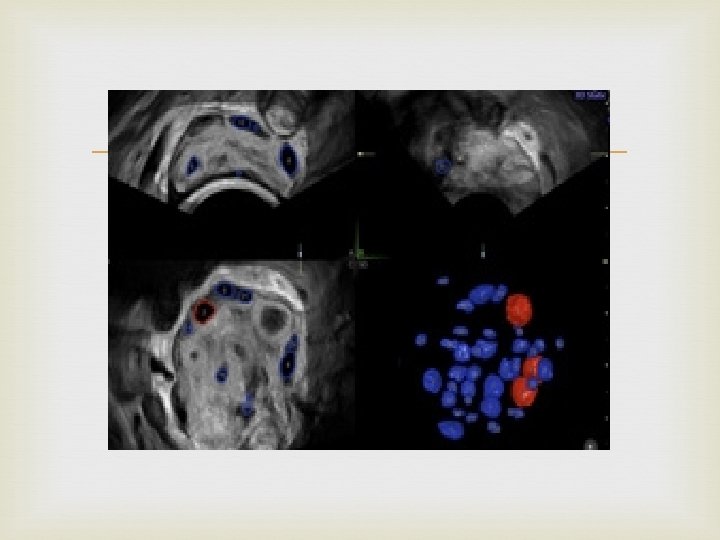
AFC AFC: antral follicle counts FNPO: follicle number per ovary Normal range: 5 -15 Choosing the stimulation protocol Higher risk of developing OHSS More follicles? ? Higher clinical pregnancy rate? ?
Baseline US Ovaries(report separately): Ovarian Volume Structure Relation to the uterus R/O of PCO Any mass lesion AFC Any echofree lesion larger than 15 mm Ovarian stromal perfusion
Any echofree lesion larger than 15 mm (may be 10 mm) Functional ovarian cysts: Any intraovarian sololucent structure measuring>15 mm in the mean diameter causing elevation of serum stradiol above 150 pm/l. They have negative effect on the pituitary ovarian axis, needs higher dose of Gn. RH in the stimulation protocol. Ovulation induction is not recommended.
Baseline US Ovaries(report separately): Ovarian Volume Structure Relation to the uterus R/O of PCO Any mass lesion AFC Any echofree lesion larger than 10 mm spe 15 mm Ovarian stromal perfusion
Ovarian stromal perfusion Positive independent relationship between the ovarian stromal PSV at the time of baseline ultrasound scan and the subsequence follicular response. (needs further studies)
Baseline US Ovaries(report separately): Ovarian Volume Structure Relation to the uterus R/O of PCO Any mass lesion AFC Any echofree lesion larger than 15 mm Ovarian stromal perfusion
Follicular development monitoring Size : interdiameter of the follicle in two planes and the average diameter is then calculated Grow by 2 -3 mm per day. Follow up is depends on patients response.
Follicular development monitoring HCG administration: larger number of mature eggs would be retrieved if smaller follicles were allowed to reach at least 13 -14 mm in diameter. Oocyte recovery rate start to decreased after the follicles exceed in diameter. 24 mm No difference in the oocyte quality obtained from the follicles between mm in diameter. 18 and 22
Mid cycle US Between days 12 and 14 of menstrual cycle: Uterus(size, shape, endometrium, any mass lesion and its relation to the endometrium). Uterine biophysical profile Ovaries(report separately): Ovarian Volume Relation to the uterus Any mass lesion Any follicles larger than 10 mm Perifollicular vascular perfusion
Perifollicular vascular perfusion Diameter of follicle : Predict oocyte maturity(Follicle with the largest diameter may not necessarily be the maturest one) but NOT quality. Perifollicular vascular perfusion: Predict Follicle maturity Morphologically normal embryo Higher pregnancy rate
Increase in perifolliclular vascularity of dominant follicle in theca layer starts developing as early as cycle. 8 th day of the
Fall in perifollicular RI starts 2 days before ovulation, reaches nadir at ovulation, remains low for 4 days and then with gradual rise reaches 0. 5 in mid luteal phase (P. I. falling to 1. 1 + 0. 4). The follicular PSV goes as high as 45 cms/sec before an hour of ovulation under the effect of rising LH.
“Follicular RI and PSV are more important in decision making than the size of the follicle. ”
3/4 th of the follicle RI 0. 4 – 0. 48 - PSV >10 c. m/s
Probability of producing embryos was. . . 75% if PSV was > 10 cms/sec, 40% if PSV was < 10 cms/sec 24% if there was no perifollicular flow
Fertilization of a follicle with a PSV of less than 10 cms/sec, have high chances of developing an embryo with chromosomal abnormality.
Unlike spontaneous cycles it is impossible to describe the dominant follicle on endosonography, due to follicular multiplicity and synchronicity. Exact vascularization of each single follicles may be difficult.
Uterine Biophysical Profile
The uterine scoring system for reproduction (USSR) 1. Endometrial thickness in greatest AP dimension 2. Endometrial layering 3. Blood flow within zone 3 using color Doppler 4. Myometrial blood flow(internal to the arcuate vessels). 5. Uterine artery blood flow (PI) 6. Homogeneous myometrial echogenicity. 7. Myometrial contractions causing a wave like motion of the endometrium.
zone 1 (subendometrial) zone 2 (outer hyperechogenic zone) zone 3(inner hypoechogenic zone)
The uterine scoring system for reproduction (USSR) 1. Endometrial thickness in greatest AP dimension <7 mm = 0 7 -9 mm = 2 10 -14 mm = 3 > 14 mm = 1 2. Endometrial layering No layering = 0 Hazy five-line appearance = 1 Distinct five-line appearance = 3 3. Blood flow within zone 3 using color Doppler Absent = 0 Present, but sparse = 2 Present multifocally = 5
4. Myometrial blood flow(internal to the arcuate vessels). Absent = 0 Present = 2 5. Uterine artery blood flow (PI) PI PI >=3. 0 = 0 2. 99 -2. 49 = 0 2 -2. 49 = 1 <2=2 6. Homogeneous myometrial echogenicity. Coarse/inhomogeneous echogenicity = 1 Relatively homogeneous echogenicity = 2 7. Myometrial contractions causing a wave like motion of the endometrium.
THANK YOU