Spleen Diaphragmatic trauma By AMGAD FOUAD Professor Of


Spleen & Diaphragmatic trauma By AMGAD FOUAD Professor Of Surgery Gastroenterology Center Mansoura University.

INTRODUCTION � Abdominal injuries are common in patients who sustain major trauma. � Unrecognized abdominal injuries are frequently the cause of preventable death. � Approximately one-fifth of all traumatized pt requiring operative intervention have sustained trauma to the abdomen. 3

Abdominal trauma � Abdominal trauma is an injury to the abdomen. It may be blunt or penetrating and may involve damage to the abdominal organs. 4

TYPES OF INJURIES q Blunt abdominal trauma is a leading cause of morbidity and mortality among all age groups. Blunt trauma: liver …spleen (most common). q Penetrating: liver, small bowel and stomach. Penetrating: present with single or multiple injuries 5
 is usually diagnosed based on clinical signs, blunt abdominal trauma")
�Penetrating abdominal trauma (PAT) is usually diagnosed based on clinical signs, blunt abdominal trauma is more likely to be missed because clinical signs are less obvious. �Penetrating trauma is further subdivided into stab wounds and bullet wounds, which have different treatments. 6

Key responses to decrease mortality and morbidity include Ø Aggressive Resuscitation Efforts, Ø Adequate Volume Replacement, Ø Early Diagnosis Of Injuries, And Ø Surgical Intervention If Warranted

ORGANS Solid Organs Hollow Organs Liver Spleen Kidneys Pancreas Stomach Small bowel Large bowel Bladder

Spleen Injuries Contusion, Laceration

Abdominal Quadrants Right Upper ◦ Liver, Pancreas, Kidney, and Lung Right Lower ◦ Appendix, Ureter, Bladder, Colon, and Gonads Left Upper ◦ Heart, Spleen, Kidney, Stomach, and Lung Left Lower ◦ Ureter, Bladder, Colon, and Gonads

Spleen Function � The primary filtering element for the blood. Acts as a filter against foreign organisms that infect the blood stream. � The site of red blood cell and platelet storage. � Filters out old red blood cells and recycles them.

More About The Spleen � The spleen is the organ most often damaged in cases of abdominal trauma. � Any injury to the spleen cause severe internal hemorrhage and shock. � If surgically removed, the liver and red bone marrow can take over the functions normally carried out by the spleen.

Still More About That Wonderful Spleen � During periods of high infection, the spleen may become enlarged, increasing its ability to become injured. � Infectious mononeucleosis is the most likely cause of spleen enlargement.

Method of Injury �Blunt trauma �Infection causes spleen to swell �Increasing chance of contusion to spleen

Signs & Symptoms � History of blow to upper left quadrant � Pale skin � Light headed � Blood pressure low � Heart rate up � Nausea � Abdominal rigidity � Pt tender in upper left quadrant but less tender if muscles are tense � KEHR's sign-pain in left shoulder

What is a spleen laceration? �A significant tear that involves the main blood vessels to the spleen which causes complete destruction of the spleen.

Spleen Laceration External lateral view of a spleen. Notice the normal slate-gray color of the spleen. Towards the right of this specimen, extending from the very top diagonally across to the bottom of the specimen, is a large tear in the capsule of the spleen, exposing the pulp. Splenic lacerations are common in automobile accidents and are particularly common if the spleen has undergone enlargement due to some reason.

Treatment � Monitor even if just had wind knocked out � See MD if symptoms persist � Nonoperative treatment is recommended with a week of hospitalization. � No activity for three weeks. Can resume light activity at three weeks to full recovery at four weeks. � If surgical repair is needed, then will require 3 months to recover, whereas spleen removal will require six months before the athlete can return to activity

Diaphragmatic Injuries

Etiology Treatment Pathology Diaphragmatic Injuries Diagnosis Clinical Presentation

Etiology Penetrating trauma Blunt trauma. Iatrogenic injury. Spontaneous rupture during pregnancy. Unexplained Spontaneous rupture. Two categories: Recognition during initial hospitalization Late Recognition

Recognition During Initial Hospitalization �Blunt Diaphragmatic Trauma ◦ Incidence of 3% in severe blunt trauma ◦ Most commonly occurs in the left leaf. ◦ The ratio of rupture of the left versus the right hemidiaphragm>>5: 1

�Various Reports of laterality incidence ◦ 34% incidence of right-sided rupture. ◦ The left diaphragm in 68. 5% of cases. the right in 24. 2%. � Other types of injury ◦ Bilateral –Pericardial- Central tendon rupture ◦ Avulsion

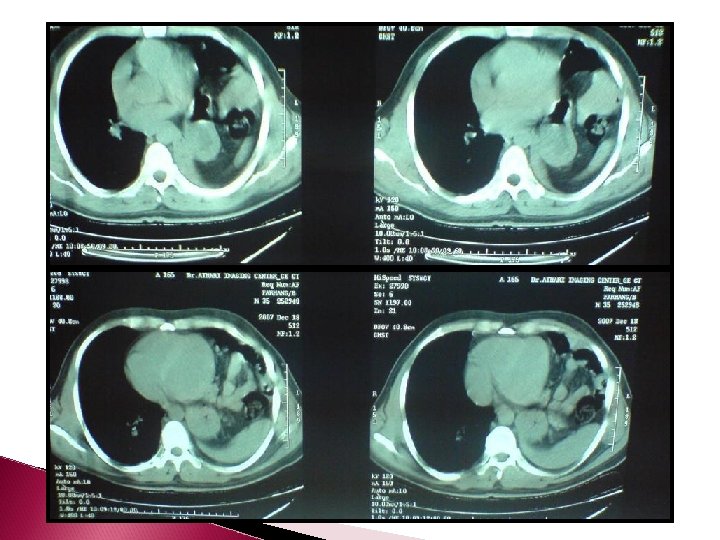
Pathology � On the left side the organs most commonly herniated into the chest are the stomach, spleen, large bowel, liver, small intestine and omentum. � On the right when herniation occurs the liver is always present and the colon is occasionally herniated. Vascular injuries (tears of the juxtahepatic vena cava and hepatic vein injuries) as well as lacerations of the liver frequently are associated

Recognition during initial hospitalization blunt diaphragmatic trauma Symptomatology �Respiratory distress, Cardiac disturbances, Deviated trachea. �Bowel sounds in the chest >>in the inority �Symptoms that are present are related to other organ injuries, such as those to the heart, lungs, or spleen, or are due to the presence of hypovolemic shock.

Blunt Diaphragmatic Trauma. Methods of Diagnosis 1. 2. 3. 4. 5. 6. 7. 8. 9. History& Physical exam Chest X Ray Sonography CT Scan MRI Contrast Studies Laparoscopy Thoracoscopy Operative Intervention DPL?

Difficulties with assessing the diaphragm. Portions of the diaphragm may abut structures of Similar attenuation (eg, liver, spleen) normally Segments of the diaphragm dome are parallel to the normal axial planes that are used in CT

Several normal variants may lead to diagnostic confusion: � Incidental poster lateral diaphragmatic defects (0. 17% to 6% of otherwise normal patients) � Areas of apparent discontinuity can be seen where the diaphragm inserts on the costal margins � There may be areas of marked localized thinning (ie, eventration ) � Advancing age also predisposes to increasing areas of nodularity and contour irregularity

Blunt Diaphragmatic Trauma. Methods of Diagnosis Chest radiography Supine positioning, portable technique, and reduced patient cooperation can limit diagnostic quality Serial radiographs may be particularly useful in ventilated patients in whom positive-pressure support overcomes the natural negative pressure gradient that normally would facilitate herniation

Concurrent abnormalities, such as ◦ Pulmonary contusion ◦ Atelectasis ◦ Pleural effusion may mask diaphragm injury

Specific radiographic signs of diaphragm injury include: ◦ Intrathoracic location of abdominal viscera, with or without a site of focal constriction (ie, “collar sign”) ◦ Clear demonstration of a nasogastric tube tip above the left hemidiaphragm
")
� Highly suggestive sign: Elevation of the left hemidiaphragm (>4 cm than the right) without associated atelectasis In 90 % of normal patients, the left diaphragm dome is 1 to 3 cm lower than the right marked

� Other sensitive, but nonspecific, findings: ◦ Obscuration or distortion of the diaphragm margin ◦ Diaphragm elevation with contralateral mediastinal shift ◦ Elevation of the right diaphragm apex
")
Blunt Diaphragmatic Trauma-Methods of Diagnosis CT �Helical CT and the newer, multidetector CT (MDCT) are mainstays in the assessment of the polytrauma Patient �Because associated visceral injuries are the immediate concern, intravenous contrast is administered routinely (150 m. L of iohexol [300 mg. I/ m. L] at 3 m. L/sec with a 45 -sec scan delay). Typically, oral contrast is administered, although it is not mandatory.

Signs of diaphragm injury : � Direct visualization of injury � Segmental diaphragm nonvisualization, � Intrathoracic herniation of viscera � The collar sign � The dependent viscera sign � Diaphragm thickening � Peridiaphragmatic active contrast extravasation

� Segmental diaphragm nonvisualization ◦ This sign must be used with caution when seen in isolation, especially in the elderly, in whom it can be a normal variant ◦ In the absence of visceral herniation, hemothorax and atelectasis may blur the diaphragm margins, and thereby, yield a false positive examination ◦ The usefulness of this sign increases when other signs of injury are present

� Intrathoracic herniation of viscera ◦ Factors that may hinder intrathoracic herniation: ◦ The presence of intrathoracic space-occupying abnormalities, such as a large hemothorax ◦ Increased intrathoracic pressure secondary to positive pressure ventilation

Herniation through torn hemidiaphragm. Hemothorax secondary to bleeding herniated omentum.

Signs of diaphragm injury COLLAR SIGN � If an abdominal structure herniates through a diaphragm rent, the free edges of the diaphragm can constrict the herniated organ, and thereby, result in a “collar. ”

DEPENDENT VISCERA SIGN � Normally, the intact diaphragm prevents the upper abdominal viscera from contacting the posterior chest wall in the supine patient. When the diaphragm is torn, its constraints are released, and the viscera may lie “dependent” against the posterior chest wall.

ABNORMALLY THICK DIAPHRAGM � In the presence of injury, intramuscular hematoma or edema or muscle retraction accounts for the abnormallythick diaphragm

Diaphragm injury DIAGNOSTIC PITFALLS OF CT � Failure to recognize normal variations � Overemphasis � Failure to recognize subtle signs of injury � Scanning � Repeat of nonspecific signs of injury artifacts scanning with oral contrast and thinner image reconstruction, or follow-up scanning after several days, may improve diagnostic confidence

MR IMAGING � Provide direct sagittal and coronal images � Imaging the entire diaphragm � Excellent � Clear contrast resolution discrimination between the diaphragm and adjacent structures, such as the liver and atelectatic lung

� The limitations of MR imaging in the setting of acute trauma � Currently available MDCT technology and videoscopic techniques � In cases of suspected delayed presentation or equivocal diagnosis by CT, MR imaging can play a valuable role as a noninvasive means to assess diaphragm integrity.

Other imaging modalities � Hepatobiliary � Barium scanning studies � Fluoroscopy � Given current CT and MR imaging technology, none plays an active role in the acute management

Sonographic signs of diaphragm injury � Herniation of viscera through the diaphragm � Diaphragm disruption � Diaphragm nonvisualization � Absent diaphragm excursion during the respiratory cycle

Ultrasound assessment of the diaphragm can be compromised by: � Pulmonary � Gastric aeration and colonic gas � Subcutaneous � Bandages and support appliances � Abdominal � Obesity emphysema pain

Diaphragm injury Given its limitations, ultrasound is not recommended as a primary tool for diagnosing diaphragm injuries.

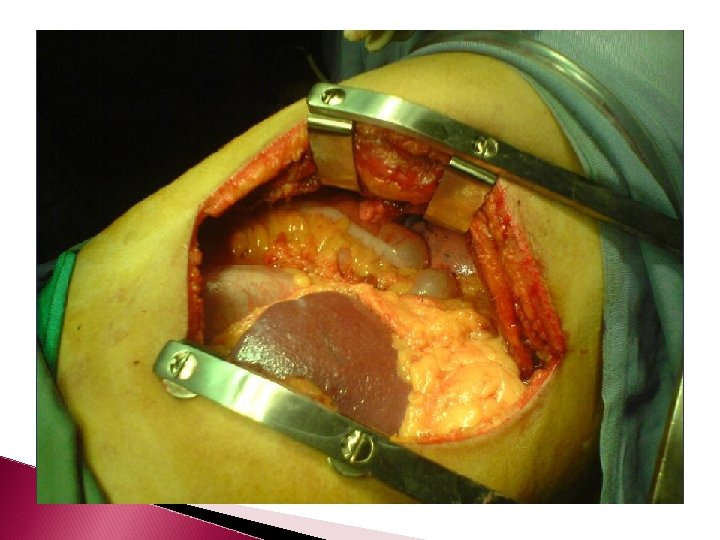
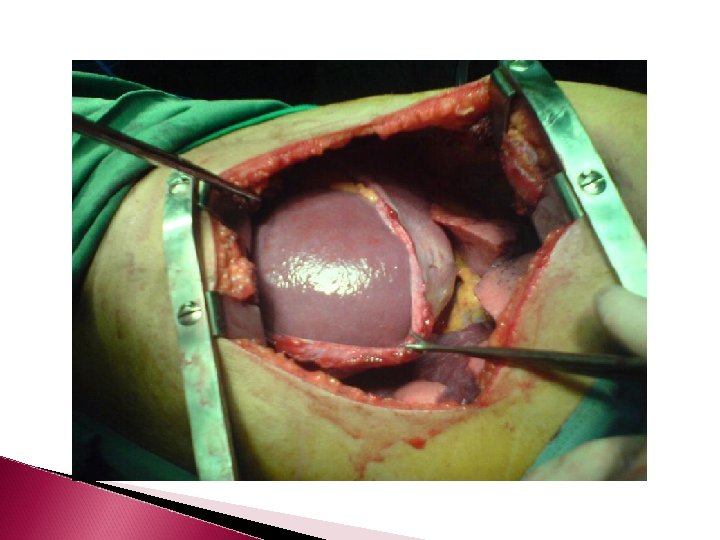
Treatment Because of the danger of development of respiratory and even circulatory embarrassment or visceral obstruction, with incarceration or strangulation of the involved portion of the gastrointestinal tract, diaphragmatic injuries should be repaired surgically as soon as possible Tears of the left hemidiaphragm are most often repaired through the abdomen

Tears of the right hemidiaphragm, when recognized preoperatively, are best repaired through a right thoracotomy , depending primarily on which cavity (thorax or abdomen) shows continued evidence of bleeding. When injury to the retrohepatic vena cava or hepatic veins is encountered during an abdominal approach, extending the incision by a median sternotomy to place a temporary vena cava shunt to control the bleeding.

After control and repair of other associated visceral injuries, the diaphragmatic tear is closed with interrupted figure-of-eight No. 0 non-absorbable sutures. Prosthetic material is rarely needed in acute blunt trauma injuries. Disruption of the repaired diaphragmatic leaf is rare.

Laparoscopic repair has been successful in selected cases. It is diagnostic in both left- and right-sided diaphragmatic injuries but only the leftsided injuries can be repaired Thoracoscopy for repair of the right -sided injuries.

Mortality � The mortality rate may be high as the consequence of other severe visceral trauma. � Reported 40. 5%. mortality rates>>> 22% , 14% , 17%,

Penetrating Diaphragmatic Injuries Result from stab wounds or gunshot wounds of the lower chest ( below the nipples), the upper abdomen ( epigastrium), the flanks, or the back Injury to either diaphragmatic leaf occurs with almost equal frequency.

Pathology � The diaphragmatic injury is generally small, and herniation of the abdominal viscera into the chest is usually absent � Only if the injury is missed does late herniation occur because of the different pressures in the two cavities.

Symptomatology � The presence of abdominal complaints or findings in a patient who has sustained a chest wound is strongly suggestive of diaphragmatic injury, as is the presence of chest findings when the site of entrance of the wound is the abdomen or flank � This event most often occurs with stab wounds, because patients with gunshot wounds of the trunk usually undergo either emergency abdominal or thoracic exploration.

Radiographic Findings � Radiograph � The of the chest >>>> normal in up to 43% abnormalities were a hemothorax, pneumothorax, or both in 96% � Herniated abdominal pneumoperitoneumin 2% each. contents or

� Ultrasonography and Computed Topographic examinations are of limited value. � When the diagnosis cannot be established and chest radiography shows an otherwise unexplained, persistent abnormality of the diaphragm or the lower lung field Laparoscopy

Treatment � In the absence of intrathoracic organ injury or major intrapleural bleeding, the abdominal approach is always preferred: � To detect non-evident intraabdominal injury � To examine both diaphragmatic leaflets

Mortality � Diaphragmatic � Of injury should not cause death. 185 patients with penetrating injuries treated, 4 2. 2%. deaths occurred, a mortality of

Diaphragmatic Injuries LATE RECOGNITION �The initial injury to the diaphragm, from either blunt or penetrating trauma, may be undetected during the patient's first hospitalization �It most likely result from missed stab wound injuries

�These hernias may be recognized any time from a few weeks to over three or four decades after the original injury. �The hernias resulting from blunt trauma tend to be larger and to contain multiple abdominal viscera.

�In order of frequency, the stomach, colon, small bowel, omentum, and spleen herniate through a left diaphragmatic traumatic defect �The colon and liver are the most commonly herniating organs through a right defect. �Those from penetrating trauma tend to contain only colon or a portion of the stomach, or both

Symptomatology ◦ The larger hernias are more likely to produce ventilatory signs and symptoms caused by reduction of the lung Volume � Gastrointestinal problems : ◦ The smaller hernias that contain only a loop of large bowel or stomach become symptomatic because of partial, and at times complete, obstruction

Diagnosis � Radiographic abnormality may include only an obscured or abnormal diaphragmatic shadow a Radiodensity a Radiolucency or one or more air fluid levels in the lung fields with or without mediastinal shift.

�The most important studies for the diagnosis are either Barium by mouth or a barium enema �The points of entry and exit are closely allied and constricted. This results in a side-by-side beaklike narrowing of the barium column

� Treatment ◦ Once the hernia is recognized, reduction of the hernia And repair of the diaphragmatic defect through the trans-thoracic route is indicated. ◦ The frequent presence of marked adhesions between the herniated viscus and thoracic contents necessitates this route ◦ Video-assisted thoracoscopy repair has been reported and Laparoscopic

Mortality � When the procedure is done electively, the mortality should approach zero. � In those patients who present with a strangulated, gangrenous viscus the mortality maybe as high as 80%

Thank you
- Slides: 72