Spine Evaluation John M Lavelle DO History n










 C 5")
 L 3: knee ext")








 n n Goal: To identify an upper")


 n n Goal: To identify radicular symptoms of")





 n n n Goal: to identify spondylolisthesis and/or facet")
 n n n Examiner's left thumb is placed on")





















- Slides: 53
Spine Evaluation John M Lavelle, DO
History n n n Onset of Pain: acute or chronic? Location of Pain: midline, lateralized? Radiation of Pain: down one leg or both legs?
History n n Strength: unilateral or bilateral loss of leg strength? Loss of bowel or bladder control? Type of pain: ache, burning, throbbing, Night Time? Parasthesia?
Observation n n Lordosis: cervical and lumbar Kyphosis: thoracic Scoliosis Pelvic Obliquity Pelvic tilt Hair tuft (faun’s beard) Lipoma Head Position Scapular Winging Muscle Atrophy
Observation n n Step off deformity Gait n n -trendelenburg -antalgic -foot drop/slap -circumducted
Range of Motion n Cervical n n n Thoracic n n n Cervical Thoracic Flexion/Extension: 45 degrees Thoracic Rotation: 50 degrees Lumbar n n Flexion: zero to 80 -90 degrees Extension: zero to 70 degrees Sidebending: zero to 20 -45 degrees Rotation: zero to 70 -90 degrees Forward Flexion: 40 to 60 degrees Extension: 20 to 35 degrees Lateral Flexion: 15 to 20 degrees Rotation: 3 to 18 degrees
Dermatomes: Cervical and Thoracic n n n C 2: C 3: C 4: C 5: C 6: C 7: C 8: T 1: T 2: T 4: T 6:
Dermatomes: Cervical and Thoracic n n n C 2: Posterior head C 3: Peri-auricular, pinna, jaw, upper neck C 4: Base of neck and shoulder C 5: Lateral arm, proximal to antecubital crease C 6: Lateral forearm, thumb, index finger C 7: Dorsal forearm, dorsal and volar index/middle and ring finger C 8: Ring and little finger, medial forearm T 1: Medial Arm T 2: Upper thorax T 4: Nipple Area T 6: Lower thorax
Dermatomes n n n n L 1: L 2: L 3: L 4: L 5: S 1: S 2: S 3: -S 5:
Dermatomes n n n n L 1: Groin and upper thigh L 2: Mid anterior thigh L 3: Lower anterior thigh L 4: Medial Malleolus L 5: Great toe and instep S 1: Lateral Foot S 2: Posterior Knee S 3: -S 5: Concentric Circles about the anus.
Myotomes n n n n C 4 -Scapular elevation (trapezius, levator scapulae) C 5 -Shoulder abduction (deltoid, rotator cuff) C 6 -Elbow Flexion (Biceps) Wrist extension (Extensor Carpi Radialis Longus and Brevis) C 7 -Elbow Extension (Triceps) Finger extension (extensor digitorum communis) C 8 -Thumb Extension (extensor pollicis Longus) ulnar deviation (flexor and extensor carpi ulnaris) T 1 -Hand intrinsics: adduction and abduction (interossei and Lumbricals) T 1 -T 12 -Thoracic extension, rotation and sidebending, rib elevation and depression T 6 -T 12 -Thoracic flexion
Myotomes n n n L 2: hip flexion ( psoas) L 3: knee ext ( quad) L 4: dorsilfexion ( tib ant) L 5: great toe ext ( EHL) S 1: plantarflex (gastroc/soleus)
Reflexes n n n n Biceps: C 5, 6 Brachioradialis: C 6, C 5 Triceps: C 7 -8 Hoffmann: upper motor lesion Babinski: upper motor lesion Jaw Jerk: CN V Adductor sign n n n Patellar: L 3 -L 4 Medial Hamstring: L 5 S 1 Achilles S 1 -S 2 Superficial Abdominal: T 7 -L 1 - no mov’t to stim Beevor’s Sign: positive if the umbilicus moves during active quarter sit up. – weak abs Cremasteric Reflex: T 12 -L 2 Anal Wink: S 2 -S 4
Palpation n n Subcutaneous tissue: hard, soft, puffy, warm, cold, boggy Fascia: restriction of motion Muscles: atrophy, hyper/hypotonic Vertebral motion: single and multi segmental - mov’t in rotation, flexion/extension, sidebending.
Palpation n Landmarks: n n n n T 2 - Sternal notch T 4 – sternal angle T 9 – Xyphoid process C 7 - vertebra Prominens T 3 – spine of scapula T 7 – Inferior angle of scapula L 4 – Iliac crests S 2 - PSIS
Palpation - Muscles n Cervical: n n n Posterior: Trap, Levator, Splenius, semispinalis, multifidus, Rectus capitus Anterior: SCM, Scalenes, longus capitus, Longus Coli Thoracic/Lumbar: n n Superficial: Iliocostalis, Longissimus, Spinalis, Rhomboids, serratus sup/inf Deep: Interspinalis, Rotatores, multifidus
Special Tests: Straight Leg Test n n Goal: To identify neurological impingement in the lumbar spine. Patient Position: supine, with the leg being tested medially rotated and the knee extended. Examiner Position: The examiner then flexes the hip until the patient complains of pain in the back or leg occurs. Positive Findings: If the pain is primarily in the back, disc is more likely herniated centrally. If the patient’s pain is more radicular, the herniated disc is more likely herniated laterally. Also, the range of hip flexion for this condition is found between 35 and 70 degrees of flexion. If the hip is flexed to greater than 70 degrees before pain, then hamstring etiology must be ruled out.
Special Test: Well Leg Raise n n Goal: To identify neurological impingement in the lumbar spine. Patient Position: supine, with the asymptomatic leg medially rotated and the knee extended. Examiner Position: The examiner then flexes the hip until the patient complains of pain in the back or leg occurs. Positive Findings: Pain recurring in the back or symptomatic leg. This test helps to reinforce a positive straight leg raising test.
Special Test: Bowstring Test n n Goal: To identify sciatic nerve irritation. Patient Position: Supine, with the affected leg internally rotated. Examiner Position: The examiner flexes the leg until pain is reproduced and then the knee is flexed until the pain is diminished. The examiner then pushes into the popliteal fossa. Positive Finding: pain reproduced with palpation of the sciatic nerve.
Special Test: Milgram n n Goal: to assess for intrathecal pathology Patient Position: supine Examiner Position: The examiner instructs the patient to raise both legs off the table approximately two inches. This position is held for 30 seconds. Positive Findings: Inability to initiate or maintain position, or pain. Indicative of intrathecal or extrathecal pathology, or pressure on the spinal cord.
Special Tests: Prone Knee Bending (Ely Test) n n Goal: To identify an upper lumbar nerve root lesion and/or femoral nerve root irritation. Patient Position: Prone. Examiner Position: The examiner passively flexes the knee to the buttock. If the patient cannot flex the knee, passive hip extension can be induced. Positive Findings: Pain in the lumbar, buttock or posterior thigh for a upper lumbar lesion. Anterior thigh represents a possible irritation of the femoral nerve.
Special Tests: Ober’s test n n Asses ITB Patient lies on their side with the unaffected leg on bottom and bent and the affected leg on top and straight. Examiner places a stabilizing hand on the patient's upper iliac crest and then lifts the straight upper leg, extends it at the hip and slowly lowers it behind the bottom leg, allowing it to adduct to the examining table. Positive if the patient can't adduct the leg to the examination table
Spurling Test n n Goal: To assess cervical radiculopathy Patient Position: Seated. Examiner Position: The test is peformed in stages. First axial compression is applied with the neck in neutral. Then the neck is extended and axial compression is applied. Finally, the neck is extended and rotated the affected side and axial compression is applied. The neck may also be sidebent to localize the symptoms. Positive Findings: A positive result is indicated if the patient experiences pain down into the arm on the same side as the compression.
Shoulder Abduction Relief Sign (Bakody’s Sign) n n Goal: To identify radicular symptoms of the lower cervical trunk Patient Position: supine or seated. Examiner Position: The examiner abducts the affected shoulder. Positive Findings: Relief of radicular symptoms is indicative of lower cervical nerve root impingement, most likely from a herniated disc.
Romberg Test n n Goal: to identify an upper motor neuron lesion. Patient Position: Standing Examiner Position: The examiner has the patient close the eyes and stand for 20 to 30 seconds. Additionally, the patient can be instructed to hold the arms outward and supinated. Positive Findings: loss of balance. If the hands are raised, the side in which the hand begins to pronate is the side of the lesion.
Adson Test n n Goal: to test for thoracic outlet syndrome Patient Position: The patient is seated and rotates the head to the affected side. Examiner Position: The examiner palpates the radial pulse and then instructs the patient to extend the head and take in a deep breath and hold it. The examiner then extends and externally rotates the arm. Positive Findings: The examiner identifies the disappearance of the radial pulse.
Halstead Test n n Goal: to test for thoracic outlet syndrome Patient Position: The patient is seated and rotates the head to the opposite side. Examiner Position: The examiner palpates the radial pulse and then instructs the patient to extend the head and take in a deep breath and hold it. The examiner then extends and externally rotates the arm. Positive Findings: The examiner identifies the disappearance of the radial pulse.
Elevated Arm Stress Test n n Goal: To identify thoracic outlet syndrome. Patient Position: sitting, with arms abducted to 90 degrees with elbows flexed to 90 degrees and hands pointing upward. Examine Position: The examiner instructs the patient to open and close hands repeatedly for 3 minutes. Positive Findings: inability to perform the maneuver for 3 minutes due to reproduction of symptoms is indicative of thoracic outlet syndrome.
Special Tests: Schober Test n n Goal: to identify loss of lumbar spine range of motion. Patient Position: Patient standing. Examiner Position: The examiner places a mark on the sacrum midway between the PSIS’s. A mark is then placed 5 cm below and 10 cm above the first mark (15 cm). The distance between the three marks is measured. The patient is then asked to flex forward and the distance between the three marks is remeasured. Positive Findings: A difference of less than 5 cm increase (20 cm) suggests a loss of lumbar spine flexion.
Special Tests: Stork Test (Gillet) n n n Goal: to identify spondylolisthesis and/or facet joint pathology. Patient Position: The patient stands on one leg and then extends the spine. This position is repeated with the other leg. Positive Findings: pain in the back. A unilateral fracture is indicated when pain is localized to one side with standing.
Special Tests: Stork Test (Gillet) n n n Examiner's left thumb is placed on the PSIS and the right thumb on the midline of the sacrum. Patient flexes the left hip and knee as much as possible with a minimum of 90 degrees of the hip flexion (the key is that the hip has to flex beyond its maximal amount of motion so that the innominate bone can posteriorly tilt with hip flexion). A negative test finds the left thumb on the PSIS moving caudal in relation to the right thumb on the sacrum. A positive finding occurs when the thumb on the PSIS does not move at all or moves cranially in relation to the thumb on the sacrum. Assess movement of the innominate bone posteriorly on the sacrum, Determine if the left or right SI joints are restricted.
Lhermitte’s Sign n n Goal: to identify spinal cord, upper motor neuron lesions, or dural tension. Patient Position: Long sitting position. Examiner Position: The examiner flexes the cervical spine while simultaneously flexing one hip. Positive Findings: Pain shooting down the spine and into the upper or lower extremities.
Special Tests: Slump Test n n n Goal: to assess for neurodynamic tension. Patient Position: Seated with the legs hanging over the edge of the table, the hips in neutral position, and the hands placed behind the back. . The patient is then put in a sequential series of positions. 1: The patient is asked to slump forward into thoracic and lumbar flexion, while the cervical spine is held in a neutral position.
Special Tests: Slump Test n n 2: The examiner pushes down on shoulders to maintain flexion while the patient actively flexes the cervical spine. 3: The examiner then applies pressure on the head to maintain cervical flexion while the patient is instructed to actively extend the knee. With the examiners caudad hand, passive dorsiflexion is initiated. The test is repeated with the other leg, and finally, with both legs. Positive Findings: reproduction of pain when the knee is extended, and symptoms are decreased when the cervical spine is extended, or increased symptoms when the patient is positioned are indicative of tension in the neuromeningeal system.
Special Tests: Hoover n n Goal: To test for malingering. Patient Position: Supine. Examiner Position: The examiner places the hands under both heels. The patient is then instructed to lift ONE leg at a time. Positive Findings: If the patient is attempting to lift one leg, downward pressure is unconsciously applied by the contralateral leg. If no downward pressure is felt, the patient may be malingering.
Waddell Signs n n n Tenderness tests: superficial and diffuse tenderness and/or nonanatomic tenderness Simulation tests: these are based on movements which produce pain, without actually causing that movement, such as axial loading and pain on simulated rotation Distraction tests: positive tests are rechecked when the patient's attention is distracted, such as a seated SLR Regional disturbances: regional weakness or sensory changes which deviate from accepted neuroanatomy Overreaction: subjective signs regarding the patient's demeanor and reaction to testing
Diagnostics: X-rays
Diagnostics: Discogram n n n Test use: This test is used to identify whether an intervertebral disc is the source of the patient’s low back pain. Procedure: a radio-opaque dye is introduced into the center of the vertebral disc. Results: If the patient’s pain is reproduced, then it is inferred that the intervertebral disc is the source of the pain. If the patient experiences pain that is different than the normal pain, then the disc is not responsible. This procedure is painful to the patient. A ct scan may also be performed to identify the integrity of the disc.
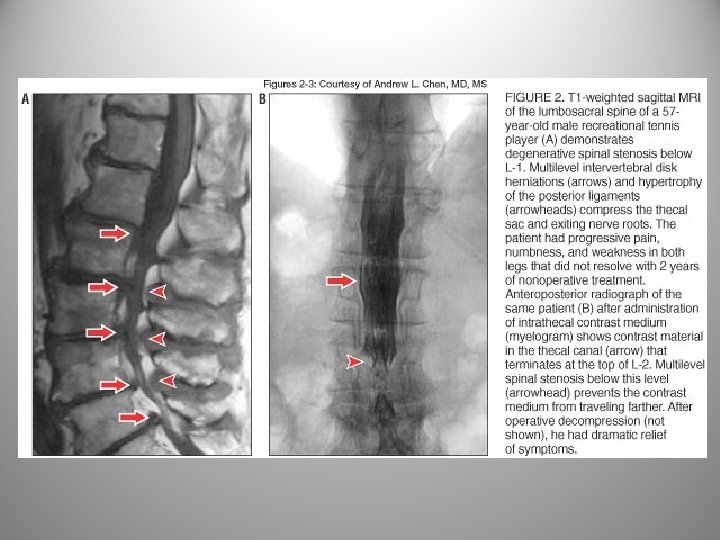
Diagnostics: Myelogram n n n Test use: To identify anatomical abnormalities within the spinal canal. Procedure: A radio-opaque dye is placed into the dural sac and a CT scan of the area is then performed. Results: The CT scan is then read to identify whether any filling defects are seen within the spinal cord and the nerve roots. Defects may represent, a herniated disc, bone spurs, infections, malignancies, etc.
MRI
CT scan
EMG/NCS
Bone Scan n n Nuclear scan in which radionuclide tracers are infused and then a the radioactive uptake is analyzed. Areas which are metabolically active will pick up more tracer than normal tissue.
Osteoporosis
Spondylolysis
Pott’s Disease Extrapulmonary TB that affects the spine. -
Paget’s Disease n n Condition in which the breakdown of bone by osteoclasts is greater than the build up by osteoblasts. This causes a weakening of the bony matrix and can lead to fractures. Often found incidentally on x -ray. Different from osteoporosis in that there is some bony remodelling. Paget’s Disease with “picture framing”
Compression Fracture
Osteomyelitis
Cancer of the Spine n Most are metastatic from other sites (breast, prostate, lung, colon), also, multiple myeloma can affect the spine.
Metastatic Breast Cancer and “Ivory Sign”
Thank you n Questions?