SPINAL CORD LEYE OLABIYI DEPT OF ANATOMY CMUL

SPINAL CORD ‘LEYE OLABIYI DEPT. OF ANATOMY CMUL

OUTLINE • • Introduction External Features Internal Features Blood Supply Grey Matter The White Matter Applied Anatomy
 SEGMENTATION COVERINGS")
INTRODUCTION • • • LOCATION SIGNIFICANCE SHAPE EXTENT AND DIMENSIONS (ENLARGEMENTS) SEGMENTATION COVERINGS

Structure of the Spinal Cord • About 18 inches long • Extends from the foramen magnum to the level of the 1 st-2 nd lumbar vertebrae • Very well protected by the vertebral column, meninges, CSF, vertebral ligaments • Gives rise to 31 pair of spinal nerves

MENINGES • Pia mater – sub-arachnoid space • Arachnoid – sub-dural space • Dura mater • Meningitis

GROSS EXTERNAL ANATOMY • • • FISURES AND SULCUS NERVE ROUTES SWELLINGS SPINAL ACCESSORY ROUTLETS TERMINATION – CONUS MEDULLARIS – FILUM TERMINALE – CAUDA EQUINA

Spinal Cord: External Features • a. blood supply: paired posterior spinal arteries and single anterior spinal artery • b. sulci: ventral median, ventrolateral, dorsal-intermediate, dorsal median • c. regionalization: segments corresponding to spinal nerves: 8 cervical, 12 thoracic, 5 lumbar, 5 sacral, 1 coccygeal (this in humans; in rats: 8 cervical, 13 thoracic, 6 lumbar, 4 sacral and 3 caudal); cervical and lumbar enlargements

External Anatomy • • • Cervical enlargement Lumbar enlargement Conus medullaris Filum terminale Cauda equina

INTERNAL FEATURES • GREY MATTER – ANTERIOR/VENTRAL GREY COLUMN – POSTERIOR/DORSAL GREY COLUMN – LATERAL GREY COLUMN – CENTRAL CANAL • WHITE MATTER – FUNICULI

Spinal Cord: Internal Features • a. dorsal horn: sensory • b. ventral horn: motor • c. lateral horn: intermediolateral cell column T 1 -L 2; preganglionic sympathetic • d. white matter divided into funiculi containing fasciculi or tracts – i. dorsal funiculus – ii. lateral funiculus – iii. ventral funiculus

Internal Anatomy • • Central canal containing CSF Anterior median fissure Posterior median sulcus Gray matter – inner portion in the shape of a butterfly – Anterior, posterior, and lateral gray horns

Dorsal horn Dorsal Funiculus Lateral Funiculus Ventral Funiculus Central Canal Ventral horn


• White matter - 6 columns that contain ascending and descending fiber tracts • These white tracts are paired and decussate • Ascending tracts - Sensory tracts – spinothalamic tract, posterior columns (fasciculus gracilis and cuneatus) • Descending tracts - Motor tracts – corticospinal tracts

BLOOD SUPPLY • SPINAL ARTERIES • RADICULAR ARTERIES

Gray Matter • The gray matter of the spinal cord consists of nerve cell bodies, dendrites and axon terminals(unmyelinated) and neuroglia. It is pinkish-gray color because of a rich network of blood vessels. • The gray matter forms an H shape and is composed of three columns of neurons-posterior, anterior and lateral horns. The projections of gray matter toward the outer surface of spinal cord are called horns. • The two that run dorsally-posterior horns which function in afferent input. The two that run ventrally-anterior horns which function in efferent somatic output. The two that extend laterally-lateral horns. • The nerve fibers that form the cross of the H are known as gray commisure-functions in cross reflexes.

G. MATTER NUCLEI GROUPS
: sensory relay and interneurons;")
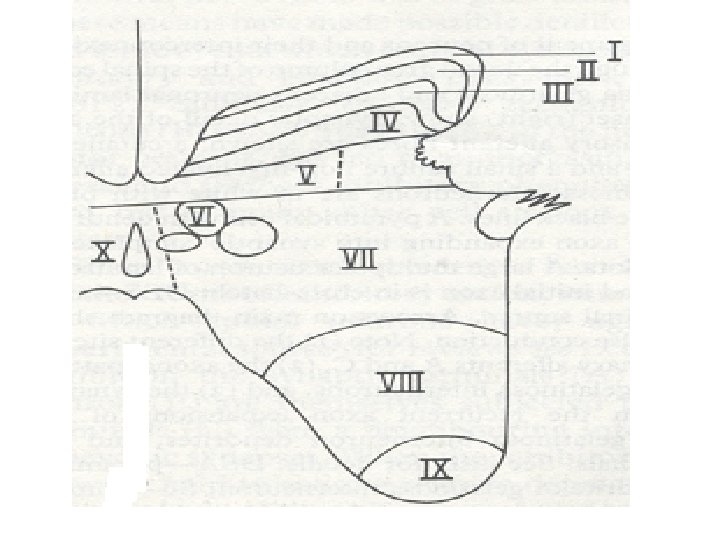
Spinal Cord: Rexed Laminae • I-IV (head or dorsal horn): sensory relay and interneurons; substantia gelatinosa is lamina II • V, VI sensory “reticular” (neck and base of dorsal horn) • VII, VIII motor “reticular” • IX motorneurons • X autonomic preganglionic neurons
 • Nucleus proprius (IV)")
Rexed’s Lamina • Some important nuclei • Substantia gelatinosa (II) • Nucleus proprius (IV) • Dorsal nucleus of Clarke • Intermediolateral cell column • Motor neuron pools

White Matter • The white matter gets its name because it is mainly composed of myelinated nerve fibers, and myelin has a whitish color. • The white matter is divided into three pairs of columns or funiculi of myelinated fibers-anterior, posterior, lateral and a commisure area. • The bundles of fibers within each funiculus are divided into tracts called fasciculi. • Ascending tracts-sensory fibers carry impulse up the spinal cord to the brain. • Descending tracts-motor neurons transmit impulse from the brain down the spinal cord.

Tracts • Each pathway is composed of organized sequences of neurons. • Upper motor neurons in the brain influence the activity of lower motor neurons in the cranial and spinal nerves. • Some neurons have long axons that terminate in processing centers-called nucleus, ganglion, gray matter of spinal cord or cortex of the brain. • Many tracts are named after their nuclei of origin, their termination as well as their location in the spinal cord (eg. Lateral spinothalamic tract). • Anterolateral System: this consists of the lateral spinothalamic tract, spinoreticulothalamic tract and anterior spinothalamic tract. This involves the general sensatins of pain, temperature and light touch. • Posterior-column medial lemniscus pathway.

Spinal Cord Tracts • Clinically important anatomy – Descending & ascending tracts • Motor 1. corticospinal tract • distal muscles – only descending tract with overt effects ~

Spinal Cord Tracts • Sensory 2. Dorsal column-medial lemniscal tract – touch, vibration, & proprioception – axons ascend ipsilaterally – synapse then decussate at medulla 3. Spinothalamic tract (lateral) – pain & temperature – decussate at SC entry level – ascends contralaterally ~

Spinal Cord Tracts 4. Spinocerebellar tract – position of body in space & relative position of limbs – affected in hereditary ataxias • no symptoms in other diseases ~

S. CORD TRACTS

CORTICOSPINAL TRACTS

SPINOTHALAMIC TRACT

Pain S 1 Thalamus VPL & intralaminar Spinothalamic Tract Spinoreticular Tract Reticular Formation DRG Spinal Cord R

DORSAL COLUMNS

S 1 Thalamus - VP Touch Dorsal column-medial lemniscal pathway Medial lemniscus Medulla Dorsal Column DRG Spinal Cord R

Spinal Cord Injuries • Who’s at risk? – ADULT MEN BETWEEN 15 AND 30 YEARS – Anyone in a risk-taking occupation or lifestyle • SCI in older clients increasing largely due to MVAs
 – MVA – Gunshot wounds/acts")
Spinal Cord Injuries • Causes (in order of frequency) – MVA – Gunshot wounds/acts of violence – Falls – Sports injuries

Spinal and Neurogenic Shock • Below site of injury: – Total lack of function – Decreased or absent reflexes and flaccid paralysis – Lasts from a week to several months after onset. – End of spinal shock signaled by muscular spasticity, reflex bladder emptying, hyperreflexia
 – Hyperextension (backward)")
Classification of SCI • Mechanism of injury – Flexion (bending forward) – Hyperextension (backward) – Rotation (either flexion- or extension-rotation) – Compression (downward motion)

Pathophysiology of SCI • Insert stuff here • Insert picture here
")
Classification of SCI • Level or Injury – Cervical (C-1 through ? ? ) – Thoracic (T-1 through ? ? ) – Lumbar (L-1 through ? ? ) • Degree of Injury – Complete • Total paralysis and loss of sensory and motor function although arms or rarely completely paralyzed – Incomplete or partial
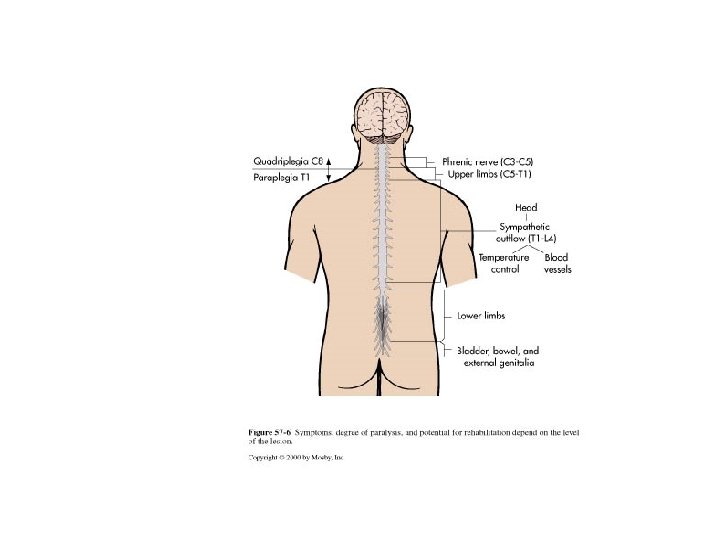

Degree of Injury – Complete transection • Total paralysis and loss of sensory and motor function although arms or rarely completely paralyzed – Incomplete (partial transection) • Mixed loss of voluntary motor activity and sensation • Four patterns or syndromes

Incomplete cord patterns – Insert picture of cord here – Central cord syndrome More common in older clients • Frequently from hyperextension of spine • Weakness in upper and lower ext, but greater in upper. – Anterior cord syndrome – Posterior cord syndrome – Brown-Sequard syndrome
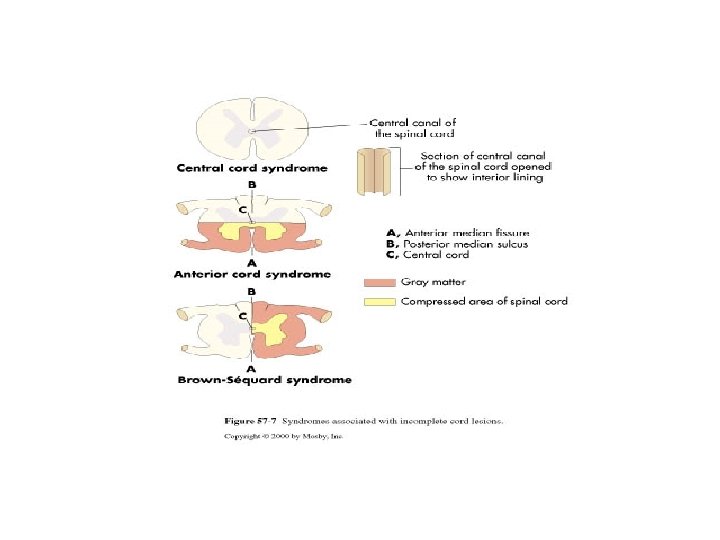

Anterior cord syndrome – Compression of the ant. Cord, usually a flexion injury – Sudden, complete motor paralysis at lesion and below; decreased sensation (including pain) and loss of temperature sensation below site. – Touch, position, vibration and motion remain intact.

Posterior cord syndrome • Assoc with cervical hyperextension injuries • Dorsal area of cord is damaged resulting in loss of proprioception • Pain, temperature sensation and motor function remain intact.

Brown-Sequard syndrome • Damage to one half of the cord on either side. • Caused by penetrating trauma or ruptured disk. ischemia (obstruction of a blood vessel), or infectious or inflammatory diseases such as tuberculosis, or multiple sclerosis. BSS may be caused by a spinal cord tumor, trauma (such as a puncture wound to the neck or back), . • a rare SCI syndrome which results in – weakness or paralysis (hemiparaplegia) on one side of the body and – a loss of sensation (hemianesthesia) on the opposite side.
- Slides: 46