SPINAL CORD INJURY Rehabilitation unit Nakornping hospital Primary

SPINAL CORD INJURY Rehabilitation unit, Nakornping hospital

Primary Cause of Death

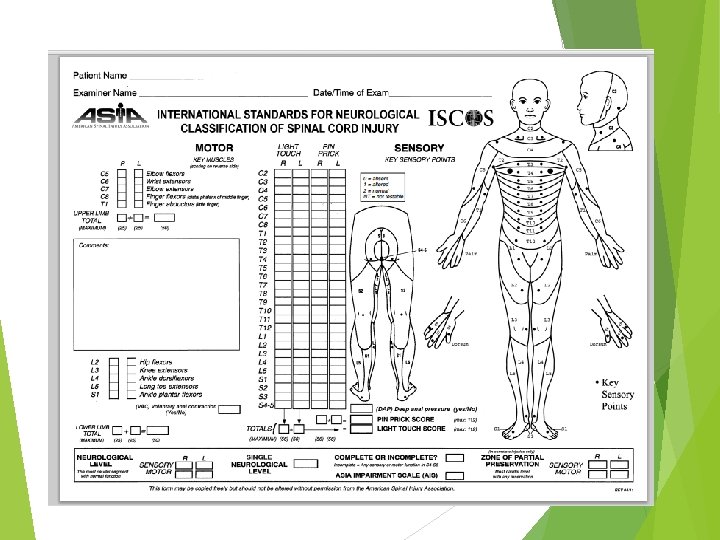

Key Muscles C 5 -elbow flexors C 6 -wrist extensors C 7 -elbow extensors C 8 -finger flexors (distal phalanx of 3 rd finger) T 1 -small finger abductors


Key Muscles L 2 - hip flexors L 3 - knee extensors L 4 - ankle dorsiflexors L 5 - long toe extensors S 1 - ankle plantar flexors PR for sphincter tone assessment

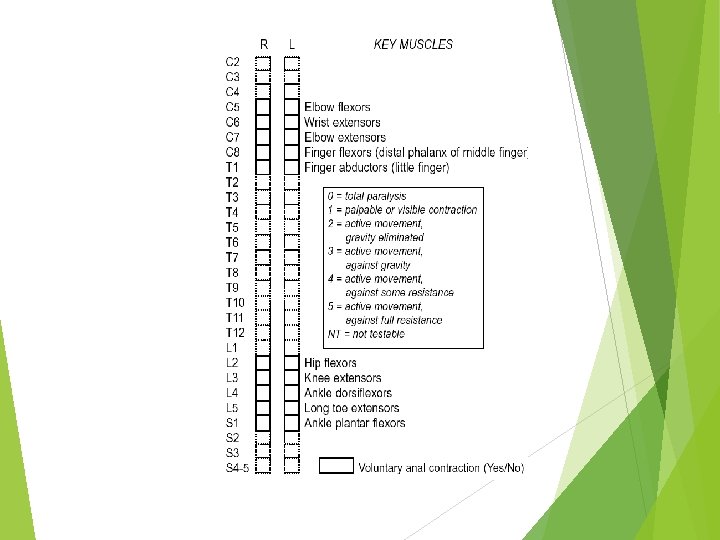
 ASIA: A (complete) ASIA: B (incomplete) ASIA: C ASIA: D")
ความรนแรงของการบาดเจบแบงตาม scale (revised 2000) ASIA: A (complete) ASIA: B (incomplete) ASIA: C ASIA: D ASIA: E ASIA impairment

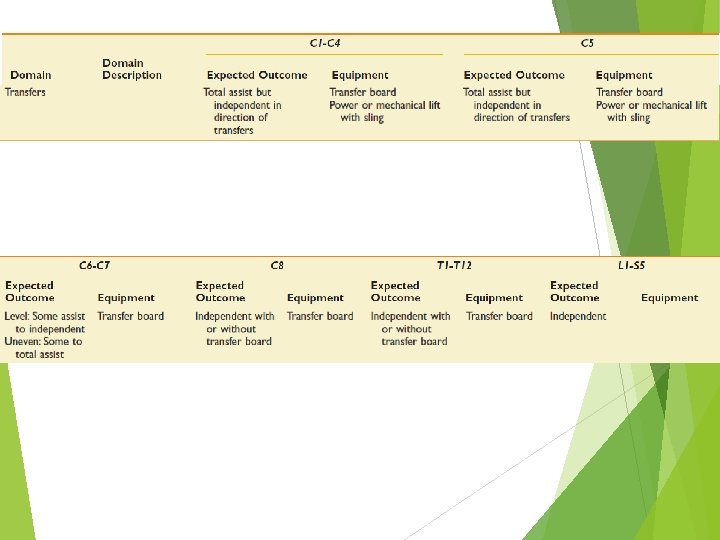
Expected Functional Outcomes by Neurologic Level of Injury

Rehabilitation Phase of Injury Goal : maximizing physical independence becoming independent in direction of care Preventing secondary complications pressure ulcer joint stiffness urinary tract GI tract etc.

Interdisciplinary Team physician Social worker Family members Recreation/v ocational therapist PT Patient OT Psychologist Dieticians Nurses Aids

Interdisciplinary Team physician Social worker Recreation/v ocational therapist Patient Psychologist Dieticians The patient and family Family members need to be educated about. PTthe nature of an SCI and the patient’s prognosis and the OT uncertainty of such Nurses Aids

Interdisciplinary Team Rehabilitation nurses, physician in addition Social to performing worker their standard nursing duties, provide. Recreation/v ocational therapist education on prevention Patient and treatment of secondary Psychologist complications, in addition to training in bowel and bladder Dieticians management. Aids Family members PT OT Nurses

Interdisciplinary Team physician Social worker Family members Physical and occupational therapists in the acute hospital should facilitate prevention of secondary complications such as contractures, pressure ulcers, and disuse atrophy. This is done Recreation/v ocational maintenance of joint ROM, PT through therapist splinting, positioning, and selective muscle. Patient strengthening. - ROM of all joints isperformed and taught by therapists to OT Psychologist people with SCI and their caregivers as soon as it is medically safe to do so. - Performance of an adequate daily stretching program can prevent joint contractures. Dieticians - Splinting of joints, with either Nurses an off-the-shelf or a custom splint fabricated by an occupational therapist, is Aids also often used to provide a prolonged stretch, to facilitate a functional joint
")
Physical Skill Training Mobility self-care skills other activities of daily living (ADL)
 joint ROM and strength Mat activities 1 1 rolling prone on elbows")
Practices (PT) joint ROM and strength Mat activities 1 1 rolling prone on elbows positioning prone on hands positioning supine on elbows positioning, long sitting short sitting quadruped positioning, transfer training

Transfer training stand-pivot and sit-pivot transfers

Transfer training complete paraplegia/lower tetraplegia

Transfer training complete paraplegia/lower tetraplegia 1. Lift feet onto bed and wheel the chair forward against bed. Put on brakes. Then bend forward and lift butt forward on chair. 2. With one hand on the cushion and one on the bed, lift the body sideways onto the bed. 3. Repeated lifts and lifting of legs may be needed.

Transfer training The floor-to chair transfer 1. Sit with legs straight, Pull seat to your side opposite the wheelchair (a person's knee can also be used). 2. With hands on each chair, push up, with your head forward over knees 3. Swing onto the seat. 4. Now, with your head forward over your knees, swing body onto the wheelchair.

Transfer training The floor-to chair transfer

Standing **with caution in individuals with chronic SCI** complete thoracic level injuries KAFO

Wheelchair Skills

Other Spinal Cord Injury Education Home and Environmental Modifications Driver Training Vocational Training

Secondary Conditions

Pulmonary System Pulmonary complications are the leading causes of death for people with SCI
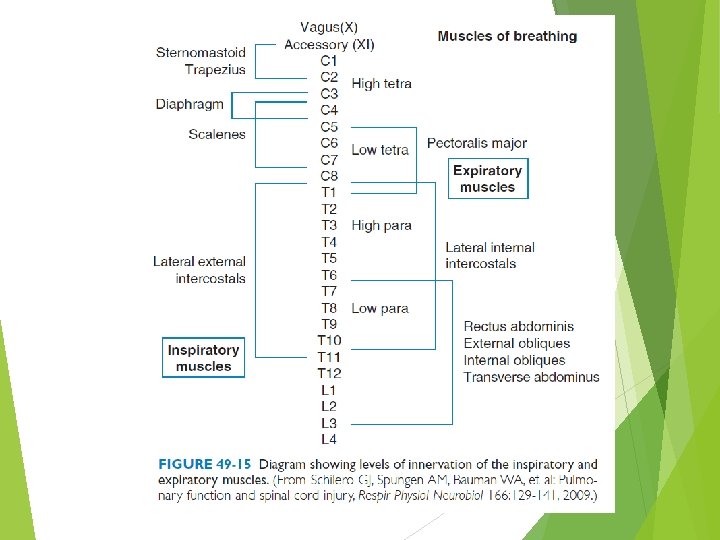

THE POSITION OF THE DIAPHRAGM

Management of Pulmonary Complications Atelectasis pneumonia, pleural effusion, empyema

lung expansion Intermittent positive pressure breathing bilevel positive airway pressure Continuous positive airway pressure (CPAP)

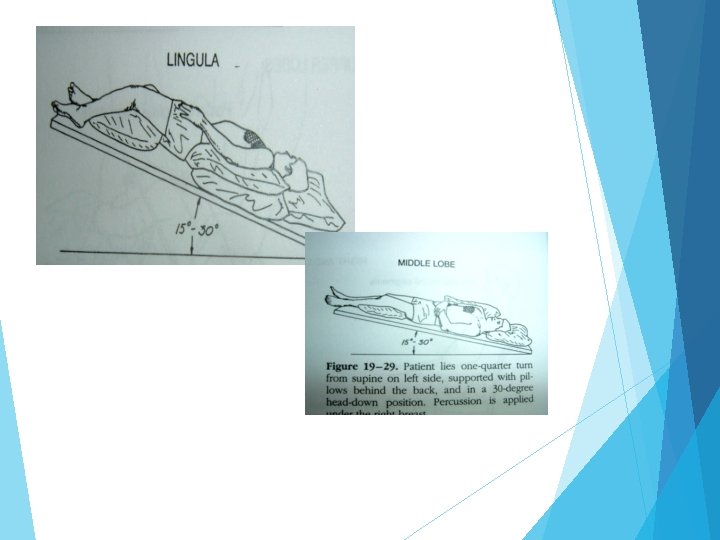
Secretion mobilization techniques Postural drainage Percussion Vibration

Postural drainage

Contraindication Severe hemoptysis Untreated acute condition severe pulmonary edema congestive heart failure large pleural effusion Pulmonary embolism pneumothorax

Contraindication Cardiovascular instability cardiac arrhythmia severe hypertension or hypotension recent myocardial infarction Recent neurosurgery

Precaution Hemoptysis Postoperation Geriatric Malignancy Unilateral lung abscess

Right and Left upper lobe

Right and Left upper lobes

Right and Left lower lobes

Right and Left lower lobes

Percussion Vibration

Chest percussion
 Pulmonary embolism")
Vascular System Deep venous thrombosis (DVT) Pulmonary embolism
 shock")
Orthostatic Hypotension Immediately after SCI a complete loss of sympathetic tone neurogenic (“spinal”) shock with hypotension, bradycardia, and hypothermia the sympathetic reflex activity returns normalization of blood pressure Supraspinal control: absent in those individuals with high-level and neurologically complete SCI orthostatic hypotension

Management elastic stockings abdominal binders hydration gradually progressive daily head-up tilt administration of salt tablets, midodrine, orfludrocortisone.

Autonomic Dysreflexia syndrome and clinical emergency that affects people with SCI usually at the T 6 level or above symptoms pounding headache Systolic and diastolic hypertension profuse sweating cutaneous vasodilatation with flushing of the face, neck, and shoulders nasal congestion pupillary dilatation bradycardia

Autonomic Dysreflexia Triggered by a noxious stimulus below the injury level Distended bladder fecal impaction pathology of the bladder and rectum ingrown toenails labor and delivery surgical procedures, orgasm Etc.

Autonomic Dysreflexia Treatment of acute AD identification of the precipitating stimulus sat up Loosen constrictive clothing and garments blood pressure monitored every 2 to 5 minutes Evacuation of the bladder done Resolved fecal impaction * Local anesthetic agents should be used during any manipulations of the urinary tract or rectum* Administered fast-acting antihypertensive agents

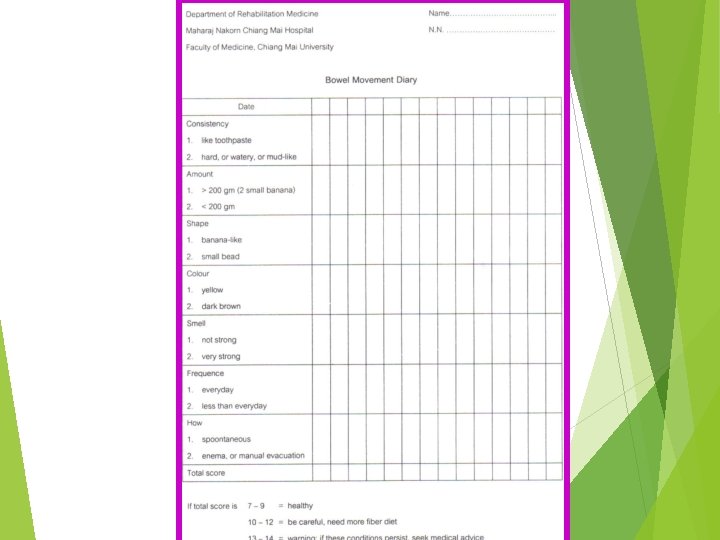
Bowel Management

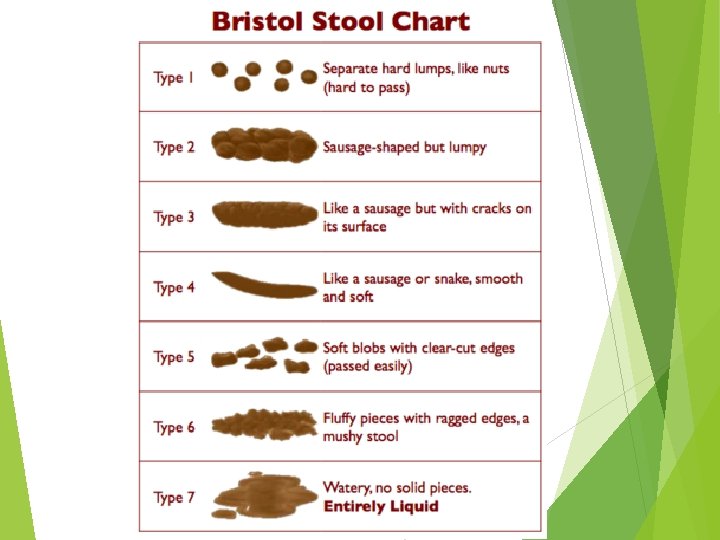
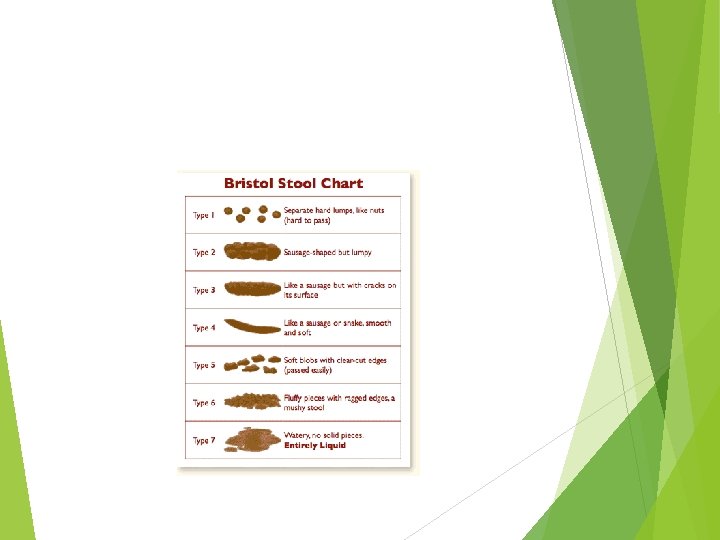
reflexic or UMN bowel areflexic or LMN bowel
 Suprasacral lesion Lower motor")
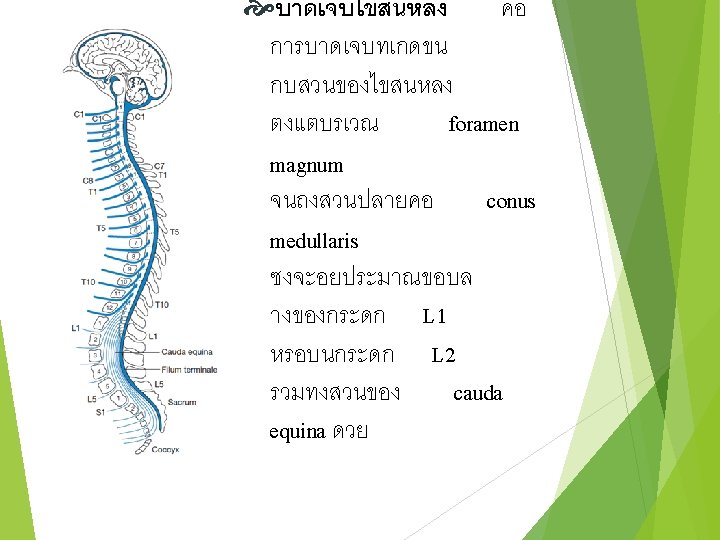
Pathophysiology of neurogenic bowel dysfunction Upper motor neurogenic bowel (UMNB) Suprasacral lesion Lower motor neurogenic bowel (LMNB) Conus medullaris, Cauda equina lesion

Upper motor neurogenic bowel ↓Colonic motility Constipation ↓Ability to sense the urge Loss volitional control incontinence Intact spinal reflex (sacral) Normal or increase anal sphincter tone

Lower motor neurogenic bowel Prolonged transit time constipation ↓ anal tone incontinence Anorectal reflex is absent or decrease Anocutaneous reflex is absent or decrease

Summarize LMNB constipation with a high risk of frequent incontinence through a lax external sphincter mechanism UMNB constipation with fecal retention behind a spastic anal sphincter require a chemical or mechanical trigger for defecation

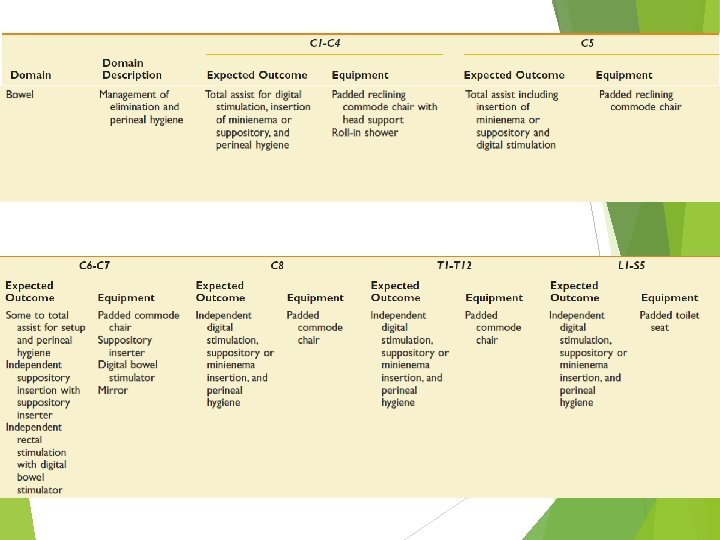
Bowel Level Outcome Expected Outcome Equipment C 1– 4 C 5 • Total assist for digital stimulation, insertion of minienema or suppository, and perineal hygiene • Padded reclining commode chair with head support • C 6–C 7 • Some to total assist for setup and perineal hygiene • Padded commode chair • Suppository inserter • Digital bowel stimulator • Mirror C 8 • Independent digital • Padded commode

Neurogenic bowel management

Management Goal of bowel program 1. effective and efficient colonic evacuation Bowel evacuation at a consistent time of day 2. preventing incontinence 3. preventing constipation. social continence - Predictable - Scheduled - Adequate defecation without incontinence at other time

Bowel program Fluid Diet Timing Frequency Medication Bowel care Procedure to periodically evacuate stool from the colon
![Fluid Must be balanced with bladder management Adequate fluid: [40 x. Bw]+500 cc](http://slidetodoc.com/presentation_image_h2/e889f27feb27f2b8634551f40aca3d72/image-71.jpg "Fluid Must be balanced with bladder management Adequate fluid: [40 x. Bw]+500 cc")
Fluid Must be balanced with bladder management Adequate fluid: [40 x. Bw]+500 cc
 Whole grain")
Diet Adequate fiber intake (No less than 15 grams of fiber daily) Whole grain breads and cereals, esp. bran Wheat Fruits germ and vegetables

Timing+Frequency Aim Timing Frequency • To avoid chronic colorectal overdistention • based on personal lifestyle needs • Schedule at the same time of day • bowel routine after a meal can take advantage of the gastrocolic response • every day in the beginning. • later on at least once every 2 days

Medication 4 general categories Stool softener Bulk former Peristaltic stimulant and prokinetic agent Contact irritant

Scheduled Bowel care Preparation Positioning Checking for stool Rectal stimulation Recognising completion Clean up
")
RECTAL STIMULATION Pelvic nerve mediated recto-colic reflex Caution: Autonomic Dysreflexia* (T 6 and above) Mechanical Chemical Digital Stimulation Suppositories Manual Evacuation Mini-enema

Digital stimulation * typically effective only for people with a UMN bowel Inserting a gloved lubricated finger into the rectum slowly rotating the finger in a circular movement until relaxation of the bowel wall is felt, flatus passes, or stool passes typically occurs within 1 minute repeated every 10 minutes until cessation of stool flow palpable internal sphincter closure absence of stool results from the last two digital stimulations

Digital evacuation * typically performed by a person with an LMN bowel inserting a gloved lubricated finger into the rectum to break up or hook stool pull it out *Abdominal wall massage, starting in the right lower quadrant and progressing along the course of colon

pulsed water irrigation colostomy

Bladder

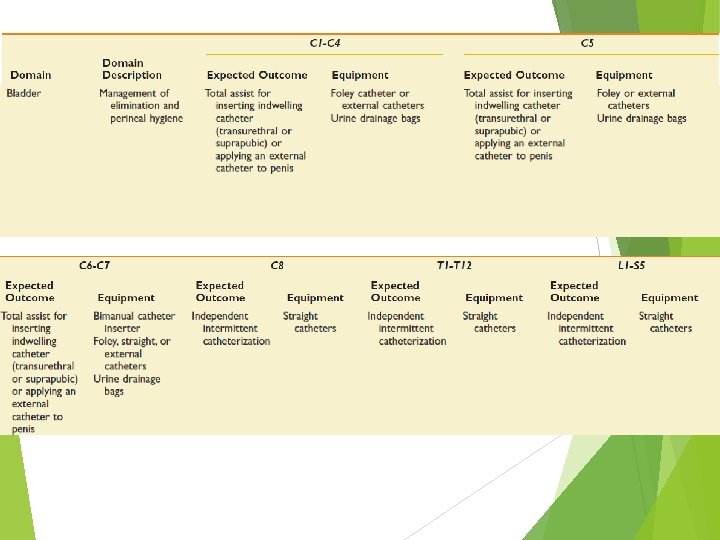
Bladder Level Outcome Expected Outcome Equipment C 1– 4 C 5 • Total assist for inserting • Foley catheter or external indwelling catheters (transurethral or suprapubic) • Urine drainage bags or applying an external catheter to penis C 6–C 7 • Total assist for inserting indwelling catheter • Independent selfcatheterization through a continent urinary diversion • Bimanual catheter inserter • Foley, straight, or external catheters • Urine drainage bags T 1–T 12 L 1–S 5 • Independent intermittent catheterization • Straight catheters

reflexic or UMN bladder Areflexic or LMN bladder

The sympathetic innervation to the bladder and bladder neck or internal urethral sphincter, which modulates relaxation of the body of the bladder and narrowing of the bladder neck to inhibit voiding, is provided by the hypogastric nerves, which exit from the spinal cord at segments T 11 -L 2. The somatic pudendal nerve, also originating from segments S 2 -S 4, innervates the external urinary sphincter

The parasympathetic innervation to the bladder, which contraction of the urinary bladder with opening of the bladder neck to allow modulates voiding, is provided by the pelvic splanchnic nerves, which exit spinal cord at segments S 2 -S 4. from the

Bladder dysfunction In spinal shock, clinical will be similar UMN type Lesion above sacral center Lesion peripheral to sacral center or complete destroys sacral center Detrusor sphincter dyssynergia. Characterized by low urinary volume high bladder pressure uninhibited detrusor contraction Hypotonic of detrusor and/or sphincter 2 possible cilinical senarios Urinary retention: sphincter + / detrusor - May trigger autonomic dysreflexia. (if lesion above the T 6 vertebrae) Continuos incontinence sphincter - / detrusor +/-

Management of Neurogenic Bladder goal of management achieve a socially acceptable method of bladder emptying avoiding complications Infections Hydronephrosis with renal failure urinary tract stones AD
 requires general level care")
CARE IN ACUTE PHASE Immediately after the injury (shock phase) requires general level care Indwelling catheter
 best option for the long-term bladder management physiologic advantage of")
Intermittent bladder catheterization (IC) best option for the long-term bladder management physiologic advantage of allowing for regular bladder filling and emptying the social acceptability of not needing a drainage appliance fewer complications than with other methods.
 total fluid intake of approximately 2000 m. L/day target catheterized")
Intermittent bladder catheterization (IC) total fluid intake of approximately 2000 m. L/day target catheterized volume of 500 m. L UMN bladder: combined with anticholinergic medications http: //www. elearnsci. org/

Reflex voiding option for men with UMN bladder Contractions can be triggered by various stimulation techniques squeezing the penis or scrotum tapping on the suprapubic area A condom catheter is a tube-vented condom that depends on a watertight seal for successful use completeness of voiding can be determined by measurement of a postvoid residual urine volume reflex voiding elevated voiding pressures vesicoureteral reflux, hydronephrosis, and eventual renal failure

indwelling catheter reasonable option for tetraplegia who are unable to perform IC men who are unable to effectively maintain an external catheter on their penis complication with UTI bladder stone formation Epididymitis prostatitis, Hypospadias bladder cancer

suprapubic cystostomy Avoid IC complication Prostatitis Epididymitis hypospadias

Other method Augmentation cystoplasty

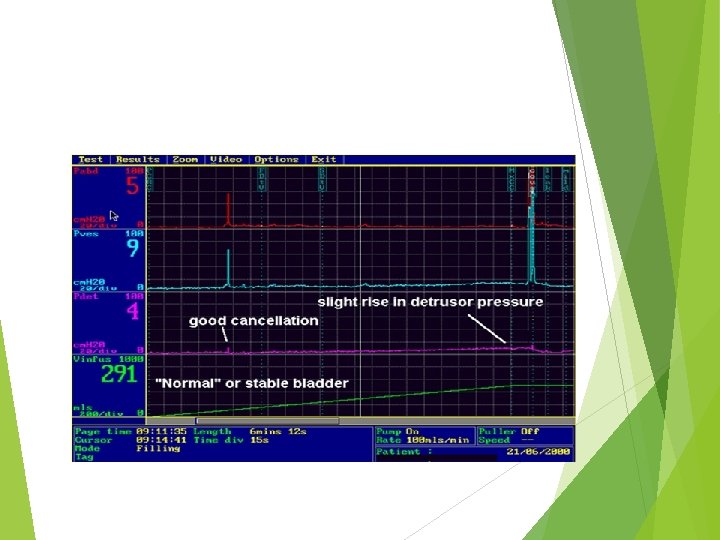
Urodynamic study 107

Spasticity Upper motor neuron Velocity dependent, increase muscle tone and stretch reflex Spinal cord injury spinal shock flaccid flexor spasticity extensor spasticity

Benefit of spasticity Delay muscle atrophy Decrease risk of DVT Decrease osteoporosis Improve standing and walking

Indication for treatment of spasticity Interfere ADL Interfere walking, transfer, wheelchair ambulation Sleep disturbance Pain Joint stiffness

Management of spasticity Identify and get rid of noxious stimuli Physical therapy: prolong stretching, tilt table standing, physical modalities Medications: baclofen, diazepam, Tizanidine hydrochloride Nerve block, motor point block: phenol, alcohol, botulinum toxin Intrathecal baclofen Surgery: rhizotomy, myelotomy

Stretching of spastic muscles Steady static stretching ROM exercises Proper positioning

Steady static stretching

ROM exercises

Proper positioning: supine

Proper positioning: sitting
- Slides: 104