Spinal Bifida Dr Gana S I NITMED TUTORIALS

Spinal Bifida Dr Gana S. I ©NITMED TUTORIALS

Introduction Spinal dysraphism – a group of congenital anomalies of the spine in which the midline structures fail to fuse Spinal bifida – confined to the bony posterior arches at one or more levels. Spinal bifida may accompany of several complex anomalies involving the spinal cord, nerve roots, dural and pelvic structures Spinal dysraphism is a major source of disability among children and adults
 - myelomeningocele - meningocele")
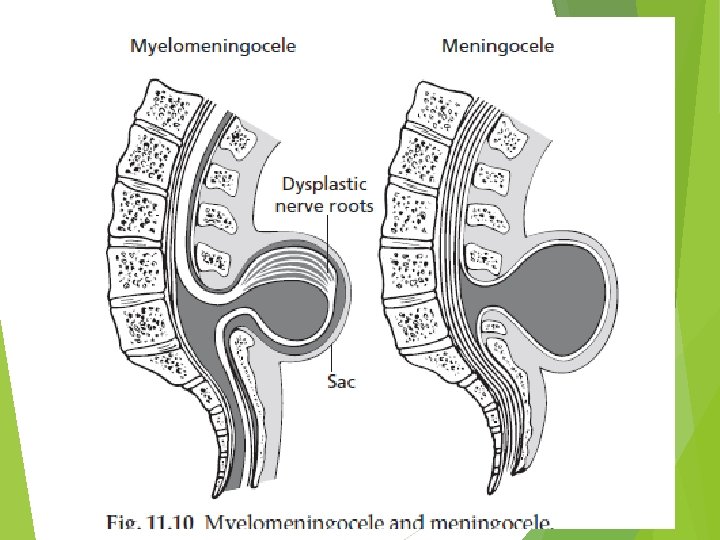
Types of spinal dysraphism Cystic Spinal dysraphism (spinal bifida cystica) - myelomeningocele - meningocele Occult spinal dysraphism (Spinal bifida occulta) - the underlying neural defect is masked by intact overlying skin - Symptoms may not develop until late childhood or even adulthood

Myelomeningocele Most common significant birth defect involving the spine Incidence is decreasing in develop countries (1: 1000 live birth) The aetiology is unknown- environmental and genetic influences - maternal nutritional status (socioeconomic status, folic acid 4 mg daily)

Embryology neurulation; - 3 – 4 weeks of gestation - Complete by 28 days - MM occurs when the posterior neuropore fails to close or it reopens Most common at the lumbosacral region

Diagnosis Prenatal diagnosis - Amniocentesis for alpha feto-protein and acetycholinesterase - Ultrasound - Prenatal MRI Postnatal diagnosis - History and physical examination


Associated anomalies Chiari II malformation Aqueductal stenosis Hydromyelia Cardiac and renal and gastrointestinal defects

Clinical features cont’d Neck Back

Meningoceles

Ruptured myelomeningoceles

Healed myelomeningocele


Upper cervical cystic dysraphism


Hydrocephalus – possible associated anomaly

Management 1. Assessment of the sac and its coverings. 2. Neurological evaluation. 3. Examination for other associated conditions: (a) within the CNS, e. g. hydrocephalus (b) extracranial anomalies, e. g. gastrointestinal, urinary. 4. Counselling and careful discussions with the parents. 5. Surgical procedures.

Neurological evaluation Difficult in neonates Limb paralysis Contracture and foot deformity Patulous anus lacking in sensation Virtually all affected neonates have abnormal bladder function – difficult to assess in newborn

Multidisciplinary care Urologist Orthopaedic surgeons Paediatricians physiotherapy Social workers

Occult spinal dysraphism Diastematomyelia Lipomyelomeningocele Tethered filum terminale Anterior sacral meningocele Myelocystocele Caudal regression syndromes

Cutaneous stigmata of occult dysraphisms Dimple Sinus tract Fatty mass Haemangioma Abnormal tuft of hair

Clinical presentation of occult Neurological symptoms are usually first noted in childhood or adolescence. Slowly progressive neurological dysfunction involving: • bowel and bladder disturbance • progressive weakness of the legs and foot deformities • back pain • sensory disability in the lower limbs • progressive scoliosis.
 MRI. Plain X-rays will")
Radiological asssessment Plain X- ray, CT scan (with intrathecal contrast) MRI. Plain X-rays will show a range of vertebral abnormalities including spina bifida, hemivertebrae, abnormal spinal curves, widened interpedicular distances.

The surgical treatment is aimed at: • removing the underlying pathological cause while preserving neural tissue • untethering the cord.

Prevention Periconceptional Folic acid supplementation Prenatal diagnosis and termination of pregnancy

Outcome Depends on: severity of dysraphism Associated anomalies interventions
- Slides: 27