SPINAL ANAESTHESIA Dr Pradnya S Joshi Associate Prof



. Thoracic & sacral concave anteriorly")











 activity •")



, inguinal hernia repair, urogenital, rectal")















- Slides: 39
SPINAL ANAESTHESIA Dr. Pradnya S. Joshi Associate Prof. Dept. Of Anesthesia
LEARNING OBJECTIVES At the end of the lecture, the student shall be able to • Describe anatomy of spinal cord • Enumerate physiological effects of spinal anaesthesia on various systems • Enumerate indications & contraindications of spinal anaesthesia • Enumerate advantages & disadvantages of spinal anaesthesia • Enumerate complications of S. A.
ANATOMY OF SPINE • Spine : composed vertebral bones & fibro cartilaginous discs. There are : 7 cervical : 12 thoracic : 5 lumbar : sacrum which is a fusion of 5 sacral vertebrae : Coccyx 4 -5
VERTEBRAL COLUMN Four curves: Cervcial &lumbar convex anteriorly (lordosis). Thoracic & sacral concave anteriorly (kyphosis) Spinal nerves: 8 cervical 12 thoracic 5 lumbar 5 sacral 1 coccygeal. Total 31
SPINAL CORD • Spinal cord continues cephalad with brain stem through foramen magnum and terminates distally in the conus medullaris at lower border of L 1 in adults and upper border of L 3 in children.
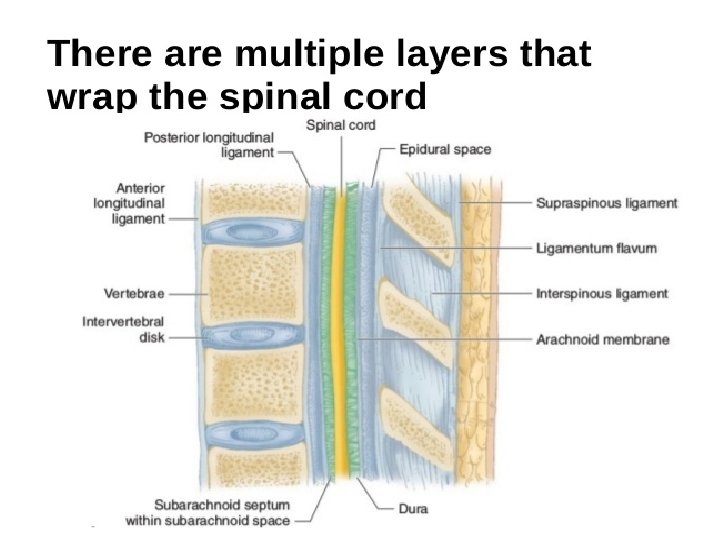
SPINAL CORD Meningeal coverings: From with in to periphery • Pia mater • Arachanoid membrane • Dura mater
SUBARACHANOID SPACE Lies between pia mater and arachnoid mater, ends at S 2 Contents: • CSF • Spinal nerves • Blood vessels supplying spinal cord
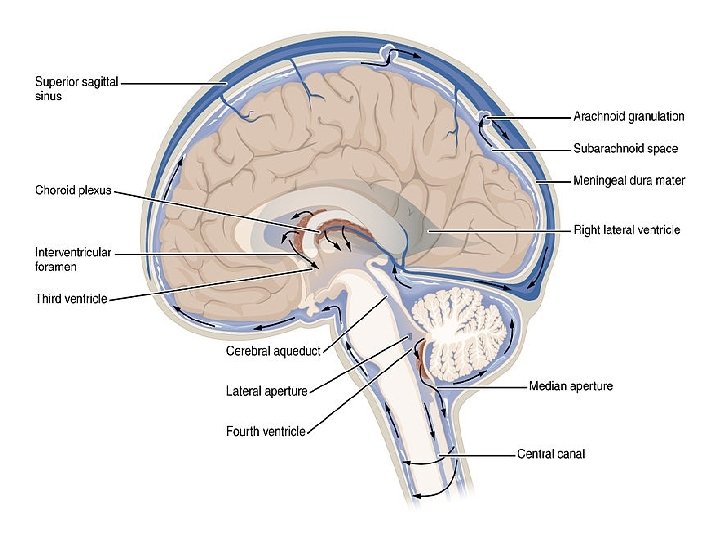
CIRCULATION OF CSF Choroid plexus in lateral ventricles Foramen of Monroe 3 rd ventricle Aqueduct of Sylvius 4 th ventricle Foramen of Luschke and Magendie Subarachanoid space. Re absorption of CSF occurs in arachanoid villi.
August Bier 1885
AUTONOMIC NERVOUS SYSTEM Has 2 components: • Sympathetic fibers Arises from T 1 - L 2 segment. • Parasympathetic fibers From craniosacral segment Cranial nerves giving rise to parasympathetic fibers: 3, 7, 9, 10 Sacral fibers arises from S 2, S 3, S 4 spinal segment.
• S. A. results in predominantly sympathetic blockade , because parasympathetic fibers carried by vagus have higher origin
MECHANISM OF ACTION • Site of action for neuraxial blockade in sub arachnoid space: nerve roots • Blockade of posterior nerve roots interrupts somatic and visceral sensation. • Blockade of anterior nerve root fibers prevents efferent motor and autonomic outflow.
ORDER OF BLOCKING NERVE FIBRES • • • Autonomic fibers Temperature fibers Pain fibers Touch fibers Somatic motor fibers
• • • T 4 ---Nipple T 5 ---Inframammary fold T 6 ---Xiphoid T 10 ---Umbilicus L 1 ---Groin S 2 -4 ---Perineum.
CVS CHANGES HYPOTENSION Occurs because of venous and arterial dilatation BRADYCARDIA Blockade of cardiac sympathetic fibers -> decrease in H. R.
EFFECTS ON GIT • Nausea and vomiting caused by unopposed parasympathetic (vagal) activity • This also results in small contracted gut which provide excellent operative conditions.
URINARY TRACT MANIFESTATIONS • Blockade of both sympathetic and parasympathetic control of bladder function results in urinary retention.
ADVANTAGES • • Low cost Decrease blood loss Less metabolic derangement Better for severe respiratory impairment Allows verbal communication Postoperative Analgesia Avoid complications of G. A.
DISADVANTAGES • • Discomfort in prolonged surgeries Potential of nerve damage Introduction of infection in CSF Post operative leg weakness & urinary retention
INDICATIONS • Primary anesthetic technique in lower abdominal procedures(LSCS), inguinal hernia repair, urogenital, rectal and lower extremity surgeries. • S. A. preferable in geriartic age group for peripheral orthopaedic , vascular and urological procedures. • Obstetric patients with full stomach
ABSOLUTE CONTRAINDICATIONS Patient refusal Infection at injection site Coagulopathy or bleeding diathesis Low fixed cardiac output states: Severe constrictive pericarditis, cardiac tamponade, severe M. S. , severe A. S. • Severe hypovolemia • Raised ICT • •
RELATIVE CONTRAINDICATIONS • Sepsis • Uncooperative patient • Spinal deformity: congenital, traumatic, post laminectomy • Severe anemia
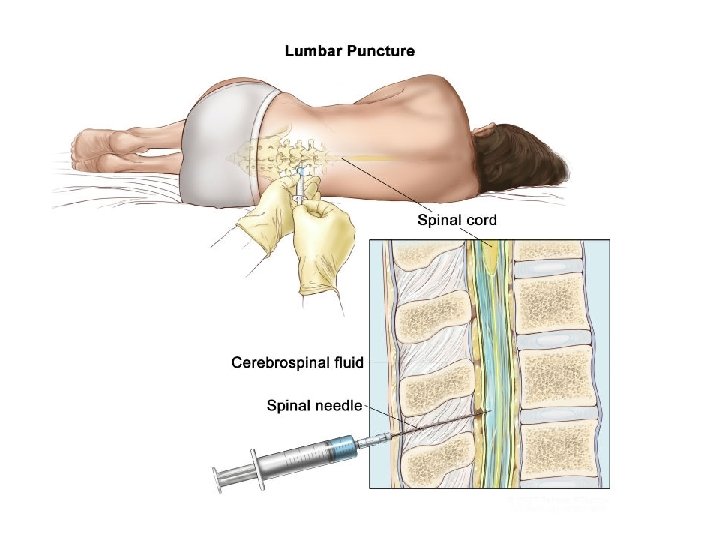
TECHNIQUE OF S. A. Equipment Spinal needle - small needles reduce the incidence of post dural puncture headache. Drugs • Lidocaine(5%) • Bupivacaine(0. 5%) • Ropivacaine(0. 5%) available in isobaric form only
Spinal Needle
Sitting Position
SITING POSITION LATERAL POSITION
Holding for Spinal
INTRAOPERATIVE COMPLICATIONS Due to exaggerated physiological responses Hypotension Management: • Maintain O 2 supply • IV fluids bolus 0. 5 -1 L • RAISE LEGS • Use of vasopressor drugs like Ephedrine or Mephenteramine
Bradycardia • When PR. < 60/Min • P. R. < 50 - Inj. Atropine 0. 6 mg Inj. Epinephrine 50 -100µg
• • • TOTAL SPINAL BLOCK: Level of block extend above T 1 involving cervical segments Nausea, vomiting, difficulty in breathing, hypotension, bradycardia. Management: Maintain adequate airway & ventilation with 100%O 2 supply. Immediately do intubation Maintain circulation with iv fluids. Vasopressor drugs : Inj. Phenylephrine, Dopamine.
• Urinary retention • Nausea &vomiting
POSTOPERATIVE COMPLICATIONS • • Postdural puncture headache occurs 12 -72 hrs post operatively. Cause Loss of CSF through dural puncture -> decreased ICP -> traction on dura & blood vessels Bilateral frontal or retro orbital or occipital headache. Increases in sitting & relieves in lying down
Management Prevention: • use smaller size needle • Prevention of dehydration Treatment: • Recumbent position, analgesics • I. V or oral fluid administration • I. V. caffeine • Epidural blood patch.
Delayed complications • • Transient neurological symptoms Cranial nerve disturbances Visual and auditory disturbances Paralysis of 6 th cranial nerve Backache Spinal haematoma Meningitis or arachnoiditis