SpeechLanguage Therapy Related to Cleft Palate Theresa M

. The Clinician’s Guide to")


 HYPONASALITY- a reduction in normal nasal resonance resulting")





 ARTICULATION DISORDERS RESONANCE DISORDERS (Secondary) LANGUAGE DISORDERS OR")





 Nasal emission- nasal air escape associated with consonants requiring high oral")

 in")

 is a resonance disorder associated with a natural “pressure")

")


 glides")









,")



…")
















- Slides: 59
Speech-Language Therapy Related to Cleft Palate Theresa M. Snelling, MA, CCC-SLP Sarah Sogan, MA, CCC-SLP Pediatric Speech-Language Pathologist Rose Cleft Palate and Craniofacial Center
REFERENCES: Peterson-Falzone SJ, Hardin-Jones MA, Karnell MP, Trost-Cardamone JE. (2006). The Clinician’s Guide to Treating Cleft Palate Speech. St. Louis, MO, Mosby. Kummer AW. (2008) Cleft Palate and Craniofacial Anomalies: Effects on Speech and Resonance (2 nd ed. ). Englewood Cliffs, NJ: Thomson Delmar Learning.
Oral structures for SPEECH AND FEEDING SOFT PALATE and HARD PALATE CREATE CLOSURE BETWEEN ORAL CAVITY AND NASAL CAVITY
WHAT DOES “NASAL” MEAN? HYPERNASAL-excessive nasal resonance during production of vowels. NASAL SUBSTITUTION-incomplete VP closure causes oral consonants in the correct place of articulation to be produced as nasal consonants… m/b, n/d, ng/g NASAL EMISSION- nasal air escape associated with production of consonants requiring high oral pressure. May be audible or not (check with a mirror. )
WHAT DOES NASAL MEAN? (Cont. ) HYPONASALITY- a reduction in normal nasal resonance resulting from a partial or complete blockage of the nasal airway by any number of sources. HYPER-HYPONASALITY (MIXED NASALITY)-the simultaneous occurrence of hypernasality and hyponasality in the same speaker usually as a result of VPI in the presence of high nasal resistance that is not sufficient to block nasal resonance completely.
DIFFERENTIAL DIAGNOSIS OF RESONANCE… “sounds like they have a cold”= hyponasality, not hypernasality. “sounds like they are talking through their nose”= may be hypernasality, but is often confused with hyponasality due to assimilative quality. NEED TO KNOW- is it too much air in nose… or lack of air?
HYPO vs. HYPER…? Hypo. Candy… sounds like “cady” Me, me, … sounds like “be, be. ” Hyper. Vowels resonate in nose… Say “EEEEE” and pinch nose, air stops or sound changes… “baby” may sound more like “Mayme” YOU HAVE TO BE ABLE TO DIFFERENTIATE!
Quick screen… Use a small mirror under nose… Use a straw or listening tube per Anne Kummer’s book (in references). On “mmmm” does air flow equally through both nostrils? On “baby, baby…” there should be no nasal airflow on mirror (unless they stop and breathe… then try with one word. ) !
AVOID THE TERM- “NASAL” …”They sound nasal…” does not differentiate hypo and hypernasality.
CHARACTERISTICS OF CLEFT PALATE SPEECH (Primary) ARTICULATION DISORDERS RESONANCE DISORDERS (Secondary) LANGUAGE DISORDERS OR DELAY VOICE DISORDERS (Laryngeal)
ARTICULATION PLACE, MANNER, AND VOICING… Most errors related to cleft palate have to do with PLACEMENT errors while manner is maintained! ATTEND TO PLACEMENT!!! Usually BACKED!
Glottal stops, nasal snorts PLOSIVES /b, p, t, d, k, g/ AFFRICATES /t. S, d. Z/
Pharyngeal Fricatives, Nasal Fricatives- s, z, sh, v, th, f Affricates- ch/t. S/, j/d. Z/
Most common articulation errors related to palatal clefts- GLOTTAL STOPS PHARYNGEAL FRICATIVES NASAL PHONEME SUBSTITIONS
RESONANCE ERRORS Primary. Hypernasality-Excessive nasal resonance during vowel productions. Less frequent: Hyponasality- a reduction in normal nasal resonance from an obstruction in the nasal airway. Mixed nasality- simultaneous occurrence of hypernasality and hyponasality from a combination of VPI and nasal obstruction at the same time.
NASAL EMISSION (articulation) Nasal emission- nasal air escape associated with consonants requiring high oral pressure. May or may not be audible- often seen in conjunction with hypernasality on vowels.
VOICE DISORDERS Hyperfunctional voice disorders, secondary to compensatory patterns of articulation and resonance. May develop vocal nodules, hoarseness, reduced vocal intensity, and persistent vocal strain. IF YOU SEE THIS, IT IS IMPORTANT TO DETERMINE IF VELOPHARYNGEAL INSUFFICIENCY (VPI) IS CONTRIBUTING- HAVE TO DEAL WITH VPI TO REDUCE VOCAL STRAIN.
LANGUAGE DISORDERS Significant occurrence of OTITIS MEDIA (ear infections and/or middle ear fluid) in individuals with cleft palate due to anatomical differences, may increase time with hearing loss, and contribute to a language disorder or delay. Other developmental issues, reduced vocal output, hospitalizations, parental reaction/attitude, and associated with some syndromes.
COMPENSATORY MISARTICULATIONS Compensatory misarticulations related to cleft palate are usually errors in PLACEMENT OF PRODUCTION. They are learned articulatory postures or placements that typically persist even after successful surgery or appliance management of the pharyngeal port and therefore co-exist with an adequate closure mechanism. They tend to be BACKED ARTICULATIONS relative to the target place of production.
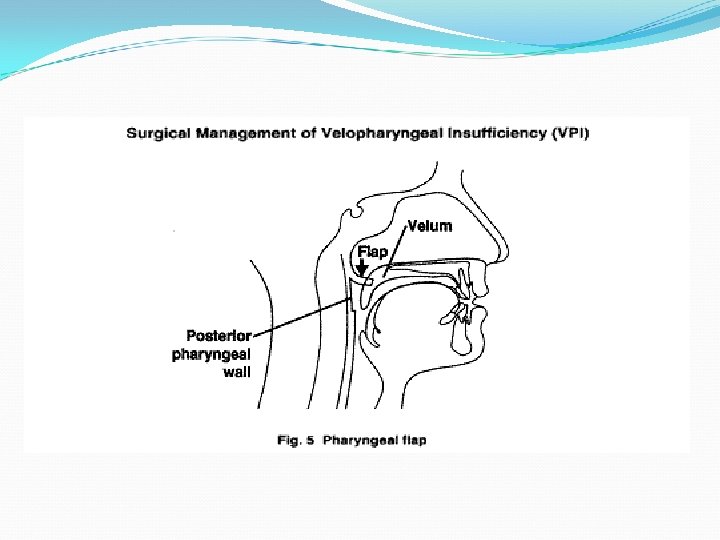
VELOPHARYNGEAL INSUFFICIENCY Velopharyngeal Insufficiency (VPI) is a resonance disorder associated with a natural “pressure valve” in the back of the mouth that does not maintain air pressures that are needed in typical speech production. The disorder may be structural or functional or results in inadequate separation of the oral and nasal cavities.
INSTRUMENTAL ASSESSMENT OF VPI In team/clinic: VIDEOFLOUROSCOPY NASOENDOSCOPY/VIDEOENDOSCOPY NASOMETRY AERODYNAMIC ASSESSMENTS In therapy setting MIRROR TEST** STRAW ASSESSMENT**
THERAPY TECHNIQUES… Goals: TO CORRECT THE PLACEMENT ERRORS (often will improve/correct hypernasal resonance. ) Improve hypernasal resonance (if it’s structural secondary surgical management is needed- but therapy should be tried first especially in the presence of articulation errors. )
Therapy techniques…continued… Target high pressure- oral vs. nasal. LABEL air flow- “windy sound”, “lip popper” for direct feedback… even with little ones (15 -18 months old. ) TARGET strong and varied vowels and glides /w, l, r, j, h/ if not present or weak-Children will often produce glides even in the presence of VPI.
Lip Rounding - W
BACKING reduction… TARGET BACKING- move sounds anterior!!! vowels (anterior round vowels /u/ /oe/) glides /w, r/…not /j/ substitution mid-dorsal IS NOT the goal… but may be the “process” of moving sounds forward (from /k/ placement, to mid-dorsal placement, to tip alveolar…) use ‘lips’ to encourage ANTERIOR airflow- rounded lips help move air forward.
SH- Round lips, anterior
BACKING reduction… TRY OVERPLACEMENT of articulators to decrease backing… ***/t/- produced as a /k/…I often start with tongue between lips rather than on alveolar ridge- then pull it back in mouth once they can produce plosive with tongue tip! (Sarah) Family was given /t/ to work on- Child produced “glottal stop + vowel” and in all word attempts- this was given as homework BEFORE child could produce a /t/! Approach- targeted /p/…moved to overplacement for /t/….
Speech Therapy- what about blowing exercises?
REMEMBER… BLOWING AND SUCKING EXERCISES DO NOT IMPROVE CLOSURE FOR SPEECH (they might improve blowing and sucking…but the goal? ? ? ) No clinical, scientific research to support the benefit of isolated blowing and sucking exercises! SPEECH/SOUND correlation needed for speech improvement…
Blowing, sucking…when to use it… If they have poor lip closure… and you “pop” cotton balls to get lip pressure…QUICKLY work into speech/sound context- “That’s a lip popper!! My lips popped- PAH!” “Pooh”, etc. BLOWING to get oral air because all air is in nose. QUICKLY work to a sound… “WHOA!” (/hw/) or “HAH” /h/ Work towards ‘sh’… BLOW AIR OUT MOUTH, CLOSE TEETH, BLOW AIR AGAIN through teeth and will approximate ‘sh’!
KEY POINTS: Ÿ Determine PLACE of articulation error and target with emphasis on manner, voicing and PLACE classifications. Ÿ Start with PLACEMENT- even pending surgery. IF YOU EMPHASIZE MANNER (plosive, fricative) with VPI- likely to teach/encourage compensatory articulation patterns.
KEY POINTS: Rule out obvious structural issues such as a palatal fistula that does not allow for a build up of oral pressure even in the presence of a functional soft palate; may need obturator to cover fistula in the hard palate.
Fistula
KEY POINTS: Ÿ Encourage strong productions-”Use Your Big Strong Mouth. ” Patients frequently will try to control nasal escape related to VPI by decreasing oral strength, pressure, and volume. This does NOT contribute to optimizing VP closure. Although increasing pressure and volume may increase audible nasal emission, it may be a stepping stone allowing for contrast, and/or improved outcome even following secondary surgery (fistula repair or pharyngeal flap. )
KEY POINTS: Ÿ Chose targets based on stimulability, visual cues (especially with young children), and contribution to keeping sounds ANTERIOR!
KEY POINTS: Ÿ Use visual and tactile feedback… pop cotton, feel airstreams on your hand, see the tongue hump in the back, see air on a mirror or with See. Scape, etc…
KEY POINTS: Ÿ Listen for and eliminate co-articulated errors!! Especially glottal stops paired with stop consonants (/b/ correct in placement with some plosive quality, but combined with a glottal stop. )
KEY POINTS: Use contrast! You will not be teaching the error… Ÿ /t/ vs. /k/ needs contrast with the above strategies; Minimal Pairs contrasts work well for carryover. Ÿ “Push air in Nose…Push/blow air out mouth”… back and forth.
KEY POINTS: With MIXED NASALITY (hypernasality seen in conjunction with denasality and/or nasal obstruction)… IT IS MOST EFFECTIVE TO CONTROL THE HYPONASALITY FIRST WITH MEDICAL SUPPORTto allow for therapy progress related to hypernasality!
CLEFT PALATE SPEECH THERAPY… Birth to 3/Preschoolers… USE INDIRECT LANGUAGE TECHNIQUES BUT… HAVE SPECIFIC SOUND AND RESONANCE GOALS! EATING/CHEWING SOUNDS – to get lip smacks! Stacking blocks- Put block to face- make BIG OPEN VOWEL SOUNDS…you put block on…then give block to child “your turn”…don’t tell them to say it at first…FIRST get the game of turn-taking (motor) then add sound…then modify sound…”POP IT!” “BIG MOUTH!”
BOOKS… Chose target words to facilitate high pressure sound development… “Where’s Spot? ” BOOK = “NO PUPPY!” Child’s response to tell mommy dog…”NO PUPPY!” “DID YOU FEEL THE AIR POP? PUPPY!!” Pop air on their hand- let them pop it on your hand… This is a great combined language and articulation goal 2 word combinations AND high pressure (plosive) sound production!!
STRIDENCY… Dolls: “sh!” for sleeping- targeting fricatives! FOOD/KITCHEN play- “HOT!” Big open air on /h/ to work towards stridency in “sh”… SNAKES- Snake sounds!! “ssss” “Shwoosh”- paired with other sounds. Paper/markers- make long lines or circles to represent continuant feature of /s/, ‘sh’, /f/…pair sound with the motor.
HIGH PRESSURE PHONEMES… Coloring paper/markers- P, B- “lip poppers”- pair sound with any motor activity. “Tap” marker on paper for /p/ or /t/… Train set…”ch, ch… Target “pop” component of the “ch” (the /t/). /k/ = back scraper; /t tongue tapper; /p/ “popper”and “feel” the air on your hand!!
WHAT IF PALATE IS UNREPAIRED OR CHILD HAS VPI? Target BIG OPEN vowels!!! Target anterior lip movement on vowels (“oh”, “oo”, “ow”…) Target Glides- yes even /l/!! Many 2 years olds CAN make an /l/, and if they’re stimulable it will usually not result in a compensatory articulation error. Target Glides- I work on both /w/ and /r/ when they are backed or omitted altogether in words- ROUND ANTERIOR LIPS move the glide forward through the mouth- THIS IS HOW YOU IMPROVE ORAL MOTOR LIP AND TONGUE AND CHEEK STRENGTH!! IN WORDS AND SPEECH!
WHAT IF PALATE IS UNREPAIRED OR CHILD HAS VPI? DON’T teach glottal stops, pharyngeal fricatives or nasal fricatives… on accident! If palate is open or too short, but not yet ready for surgery… be very aware of your targets!! To get good lip use, target /m/ words and tread lightly with a STRONG /b/- will get a paired glottal stop!
WHAT IF PALATE IS UNREPAIRED OR CHILD HAS VPI? TARGET Glides and BIG vowels to increase intelligibility! More accuracy on vowels will improve intelligibility even in the presence of VPI! VOICELESS plosives /p, t, k/are easier to approximate if VPI is present and less likely to be paired with a glottal stop than VOICED cognate /b, d, g/. Target voiceless, with light contact
PRIOR TO PALATE REPAIR: Target IMITATION!! Not necessarily specific sounds, but the GAME OF IMITATION! This goal lays the ground work for speech therapy post palate repair. Target more than just receptive language skillsexpanding play skills and motor imitation. Reciprocal vocalizations- develop between 6 -9 months- play with vowels and inflection and facial expressions.
AFTER palatal repair: Teach the contrast of oral vs. nasal by using terms like “that was in your mouth!” “Uh Oh, that was in your nose!” (my nose too!) Target- big, open vowels…and high pressure consonants (plosives, fricatives and affricates)… IN THE CONTEXT OF PLAY for little ones!!!
GOALS AND OBJECTIVES: HAVE specific targets…related to resonance, articulatory placement, and compensatory articulation patterns: High pressure phonemes (even with 18 month olds). Stridency (sh, s) in sound play or words. Glides (w) using lip rounding. Develop big open vowels to reduce Hypernasality. If connected speech is mumbled with poor intelligibility- target “use your big, strong mouth”.
GOALS AND OBJECTIVES: PROGRESS reports should include information about: Resonance. Articulatory placement patterns. Strategies that worked to address goals. Compensatory articulation errors.
REPORTS! INCLUDE DETAILS RELATED TO CLEFT PALATE IN YOUR REPORTS… IT’S CRITICAL TO THE DECISIONS THE CLEFT PALATE TEAM HAS TO MAKE OVER TIME! TO DETERMINE IF SECONDARY SURGICAL MANAGEMENT IS NECESSARY- IT’S IMPORTANT TO KNOW WHAT HAS BEEN TARGETED IN THERAPY!!
CLEFT LIP/PALATE TIMELINE TEAM CONSULTATIONS- Birth to Adulthood LIP repair- birth to 3 months PALATE repair- 9 -15 months GENETIC counseling – Birth to Adulthood Follow-up varies with diagnosis Pediatrics/Primary Care- Birth to Adult (Establish a Medical Home)
CLEFT LIP/PALATE TIMELINE cont. ENT CARE: Ears/Hearing- Birth to Adulthood Nose/Nasal Airway- Childhood to Adulthood (Rhinoplasty, Septoplasty, Turbinate reductions, Tonsil/Adenoid, etc. ) Final nasal surgery when facial growth is complete (different for males/females) from 16 -21 years. SPEECH/LANGUAGE/RESONANCE- 6 mos. to Adulthood (or until normal speech and resonance established. ) From Birth- for feeding support
CLEFT LIP/PALATE TIMELINE cont. PLASTIC SURGERY- Birth to Adulthood ORTHODONTIA- 7 years to adulthood (often 2 rounds of pre-surgical orthodontia and/or post oromaxillofacial surgery) ORAL Surgery- 6 years to adulthood BIRTH To Adulthood with some craniofacial conditions/syndromes Bone graft (8 -12 years) Orthognathic surgery (13 years to adulthood) Pediatric Dentistry- Birth to Adulthood (establish a dental home)
CLEFT LIP/PALATE TIMELINE cont. Social Work/Psychologist- Birth to Adulthood Developmental Assessment- Birth through School-age (often completed by Pediatrician, Speech Pathologist, Psychologist, or community providers in health care setting or school. ) Occupational Therapy- Feeding Birth through establishment of feeding success.