Specimen collection transport and handling Talat Mokhtari Azad







 For countries in the Middle East Minimum standard for")





")

- Slides: 22
Specimen collection transport and handling Talat Mokhtari Azad Head of Virology Department Director of National Influenza Centre School of Public Health Tehran University of Medical Sciences 1394
Successful laboratory investigations ü Collection of adequate and appropriate specimens ü Sufficient documentation ü Biosafety and decontamination ü Correct packaging ü Rapid transport ü Choice of a laboratory that can accurately perform the tests ü Timely communication of results
Collection of clinical specimen for virus isolation • • • Enveloped Viruses ( Influenza, Measles, Rubella and Corona viruses are very temperature labile and susceptible to desiccation Throat swabs should be immediately added to viral transport medium (VTM) upon collection Must be kept at 4˚C or -70˚C for longer term storage (>4 -5 days)
Influenza
Who Should be tested • • • A person with fever, cough and pneumonia, who requires admission to hospital. AND any of the following: • CLUSTER: without regard to place of residence or history of travel • HEALTH CARE WORKER: without regard to place of residence or history of travel • Hx of travel to the Middle East within 14 days • UNUSUAL COURSE: without regard to place of residence or history of travel ALSO: ANY respiratory illness if close contact with case w/in last 14 days
Who should be tested (continued) For countries in the Middle East Minimum standard for surveillance should be testing of patients with SARI requiring mechanical ventilation Include investigation of clusters; health care workers unusual presentation or clinical course
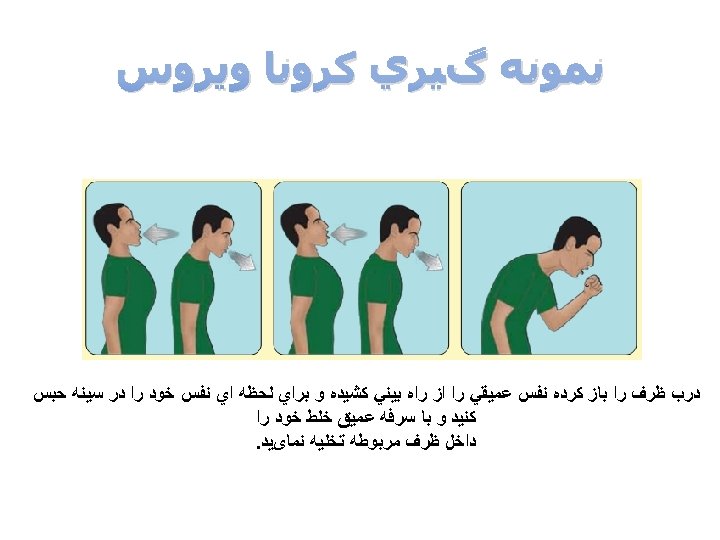
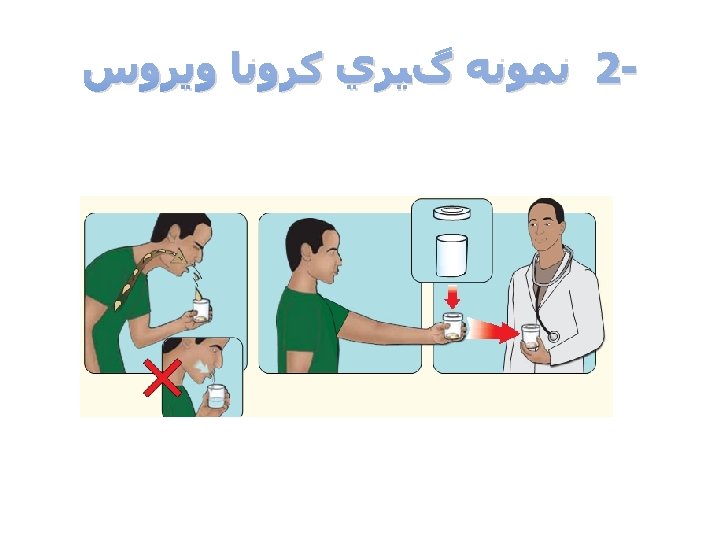
What to collect Strongly ◦ If advise lower respiratory specimens e. g. , sputum, endotracheal aspirate or bronchoalveolar lavage should be used when possible no Sns or Sx of lower respiratory tract infection: Get both NP and OP specimens NP is negative and MERS strongly suspected, retest.
What to collect • Strongly advise lower respiratory specimens • • If no Sns or Sx of lower respiratory tract infection: • • e. g. , sputum, endotracheal aspirate or bronchoalveolar lavage should be used when possible Get both NP and OP specimens If NP is negative and MERS strongly suspected, retest.
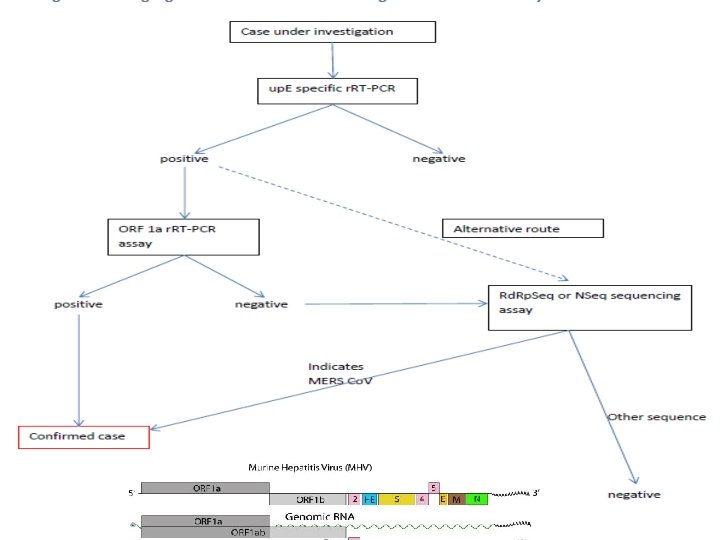
Real time PCR assay overview Confirmation 1 a/1 b Limit: 4. 1 RNA copies/reaction Screening with up. E Limit: 3. 4 RNA copies/reaction
Measles virus Nonsegmented negative-strand RNA genome ~ 16 kb 3’ Le 5’ N P/V/C M H protein F H L Tr
ﺷﻤﺎﺋی ﺍﺯ ﻋﻔﻮﻧﺖ ﺑﺎ ﻭیﺮﻭﺱ ﺳﺮﺧک Patients positive 100% Ig. G: serum 75% Ig. M: in serum 50% 25% Virus for culture from throat or urine -3 -1 1 3 5 7 Fever Rash ﺩﻭﺭﻩ کﻤﻮﻥ ﺭﻭﺯ 17 -8 (-3 to 5 days) 14 21 28 35 Day of illness** (0 to 5 days) **Day 0 = first day of rash ﺗکﻨیک ﺍﻻیﺰﺍ ﺭﻭﺵ ﺍﺳﺘﺎﻧﺪﺍﺭ ﺑﺮﺍی ﺗﺸﺨیﺺ ﺳﺮﺧک ﻭﺳﺮﺧﺠﻪ ﺍﺳﺖ 60 90
Specimens for Measles & Rubella Laboratory Diagnosis ü minimum 1 ml blood sample ü(infants) & others ≥ 5 ml from adults ü 3 fully filled circles of dried blood on a filter-paper üor oral fluid. For oral fluid samples, the spongecollection device should be rubbed for about 1 minute along the gum until the device is thoroughly wet Throat swab and Urine for virus isolation When to collect first patient contact to health facility: adequate collected within 28 days after rash onset Ideally, samples for virus detection should be collected simultaneously with samples
Thank you