Specific learning objectives After the End of this

Specific learning objectives • After the End of this chapter students should able to : • List the functions of surfactant. • Explain Compliance and Dead space. • Diffusion capacity of gases. • Ventilation –perfusion ratio

Dead Space • Area where gas exchange cannot occur • Includes most of airway volume • Anatomical dead space (=150 ml) • Physiological dead space = anatomical + non functional alveoli 2

DEAD SPACE Anatomical dead space – the volume of air in the conducting region that does not take part in the gas exchange=150 ml Physiological dead space – total volume of air not equilibrating with blood In Health, ADS = PDS
 VD NO")
Basic Structure of the Lung A tube = Airway (Trachea – Bronchioles) VD NO GAS EXCHANGE DEAD SPACE VA A thin walled Sac = Alveolus GAS EXCHANGE OCCURS HERE Blood Vessels Formula: Total Ventilation = Dead Space + Alveolar Space VT = V D + V A 4
")
Similar Concept: Physiological Dead Space Healthy Lungs: • Anatomical Dead Space = Airways (constant) Diseased lungs: VD VA Physiological = Anatomical Dead Space + Additional Dead Space Blocked Vessel 5

Surface tension: • Intermolecular attraction between the surface molecules and thus it reduces surface area and collapses the lungs. • liquid-air interface Disadvantage • It should be reduced during expiration or else collapse of the lung take place. • opposes the expansion of the lungs during inspiration.

Mechanism of action of Surfactant • Surfactant consist of mainly of–Phospholipids • Phospholipids have hydrophilic (phosphate portion) & hydrophobic (lipid portion) ends • The hydrophilic end dissolves into the alveolar fluid; while the hydrophobic end facing the exterior. • As the hydrophobic portion (lipid) has attraction towards gas, the inward attraction of the molecules of the surface area can be minimized & thereby lowering the surface tension.

• According to the law of Laplace in a spherical structure like alveoli • P=2 T R P=distending pressure T=tension on the wall R=radius. In the lungs ST is reduced by Surfactant.

SURFACE TENSION AIR LIQUID

Surfactant, a phospholipid secreted by type II pneumocytes

Pulmonary surfactant Ø Tendency of the lungs to recoil back from the chest wall is governed by 1. recoil of elastic tissues of lungs 2. Surface tension within the alveoli. Chemistry Ø Protein lipid complex Ø DPPC secreted by type 2 cells pneumocytes. Ø Comes to the surface by exocytosis. Ø Removed by PAMS

Alveolar volume changes without surfactant The surface tension of alveoli would cause small alveoli to empty into larger alveoli if it were not for the effect of surfactant. Clinic relation… Neonatal respiratory distress syndrome, NRDS

Alveolar pressure does not changes with surfactant Law of Laplace: P=2 T/r Small-volume alveoli have a small surface tension while largevolume alveoli have a large surface tension. This enables alveoli of unequal size to exist side-by-side.
; It reduces")
Physiological significance u u It is beneficial to maintain alveolar volume (stability); It reduces interstitial fluid production of lung interstitial tissue and alveolar cavity to prevent pulmonary edema Keeps alveoli dry It decreases inspiratory resistance, reduces inspiratory work and help pulmonary ventilation and lung expansion. 14

• Factors affecting surfactant • Long term inhalation of 100% oxygen • Occlusion of main bronchus Increases Due to 1. Thyroid hormones 2. Glucocorticoids , maturation of surfactant
 It is associated with low-levels of surfactant. Atelectasis")
• Respiratory Distress Syndrome (IRDS) It is associated with low-levels of surfactant. Atelectasis Hyaline membrane disease When a child is born prematurely (28 th – 32 nd week) lungs do not yet have surfactants. Disease can be detected during birth by determining the Sphingomyelin to Lecithin ratio of the amniotic fluid.

Compliance • Compliance is the measure of stretch ability or elasticity or distensibility • Hooke’s law –when a perfect elastic matter is acted upon by a unit force it will stretch by a unit length • Compliance is change in volume by unit change in pressure (∆V/∆P) –ml/cm H 2 O (L/cm H 2 O) • Specific compliance –Compliance/FRC (in L per cm H 2 O per L) • Elastance –Reciprocal of compliance (5 to 8 cm H 2 O / L)

Types of compliances • As both lungs & thoracic cage has elastic nature –in the respiratory system the various compliances are; • Lung compliance (L. C) • Thoracic compliance (Th. C) • Total compliance (T. C) -- (both L. C & Th. C) • Compliance is measured in static condition

Total compliance • Normal value – 0. 11 L / Cm H 2 O • Measurement -- ∆V / ∆P (Airway pressure – Intra pulmonary Pressure)

Lung compliance • Volume of lung expand for each unit increase in intra pleural pressure • Measured by inspiring a series of known volume of air and simultaneously recording the intrapleural pressure of each • Normal value – 0. 22 L / cm H 2 O • (range – 0. 09 to 0. 26 L / cm H 2 O) • In infant – 0. 05 L / cm H 2 O
 2.")
Factors determining lung compliance 1. Elastic nature of pulmonary tissue (contribute 1/3 rd) 2. Surface tension (contribute 2/3 rd)

Elastic nature of pulmonary tissue • Inter woven of elastin & collagen fibers like nylon stocking arrangement. • In emphysema –degradation of elastin & collagen frame work –leads to increase distensiblity. • In old age –change in physico-chemical properties of elastin & collagen –increase distensibility • In pul. fibrosis –increase in interstitial tissue –stiffness – distensibility

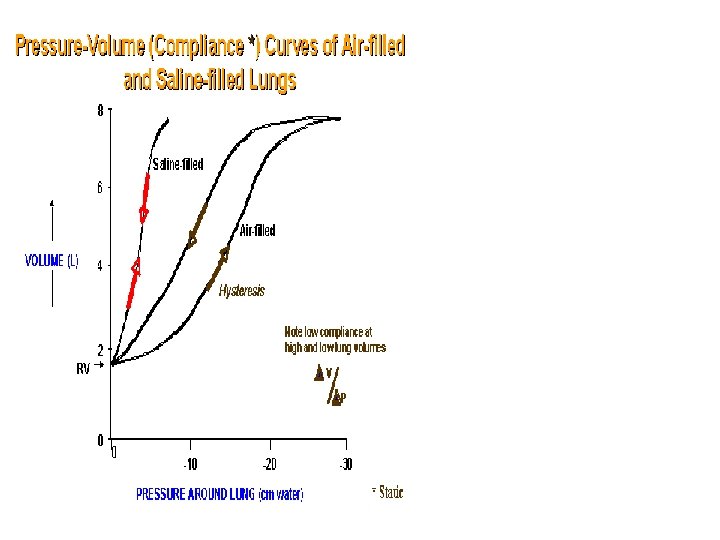
Lung Volumes Changes Related To Transpulmonary Pressure • Inspiration & Expiration compliance is different • Mechanics of inspiration & expiration differ • Curves vary because forces on lung differ during breathing cycle

Hysteresis loop

• Hysteresis loop • In both inspiration and expiration the rate of volume change is equal to the rate of air flow. • Greater the flow rate greater is the vertical deviation from the central line.

• Because of difference in expansiblity of lung and thorax • Viscous resistance depends on rate of lung expansion and contraction. • • • Airway resistance Factors affecting lung compliance Lung volume Phase of respiratory cycle Effect of gravity Surface tension

• • • Work done during breathing Elastic resistance -65% Non elastic resistance Airway resistance 28% Viscous resistance 7%

Work of Inspiration

Diffusing capacity of the respiratory membrane “Volume of a gas that will diffuse through the membrane each minute for a partial pressure difference of 1 mm Hg”

Respiratory membrane Average thickness = 0. 6 µ

Diffusion capacity Amount of gas that crosses the respiratory membrane/min/mmhg Depends on • surface area of alveolar capillary membrane • Thickness of membrane • Solubility of gas • Molecular weight.

• Normal Diffusion capacity for oxygen Do 2=20 -30 ml/min/mm. Hg at rest. Factors Affecting diffusion capacity Dc: • Surface area and thickness of alveolar capillary membrane. Dc= Surface Area of the membrane Thickness of membrane • Solubility and molecular weight Dc= Solubility of the gas √Mw of thegas DCo 2=20. 7*Do 2

• Measurement of Diffusion capacity Do 2= o 2 consumption /min mean ( Palv o 2 - PCap o 2) DCO= Co uptake/min mean ( Palv Co - PCap Co)

Ventilation-Perfusion ratio • Two factors that determine the alveolar PO 2 & PCO 2 are – • Rate of alveolar ventilation (VA) – 4 liters • Rate of alveolar perfusion (Q) –CO=5 liters • The ventilation-perfusion ratio = VA/Q = 4/5 = 0. 8

When VA is normal & Q is also normal =VA/Q is normal When VA is zero & Q is normal =VA/Q is zero When VA is normal & Q is zero =VA/Q is infinity VA/Q is zero –composition of alveolar PO 2 & PCO 2 approaches to that of venous blood • VA/Q is infinity –composition of alveolar PO 2 & PCO 2 approaches to that of atmospheric air • When VA/Q is below normal Physiological shunt is increased • When VA/Q is above normal Physiological dead space is increased • •

• Physiological shunt -Volume of blood does not take part in blood-gas exchange is called (physiological) shunt VA/Q is below normal –Physiological shunt increased • Physiological dead space volume(Dsv) - Volume of gas does not takes part in blood-gas exchange VA/Q is above normal – Dsv increased

Normal variation in VA/Q ratio • Normal individual, in upright posture— • VA/Q ratio variation from Top to Bottom of lungs is –from 3 at top to 0. 6 at bottom • Reasons – • Effect of gravity • Variation in intra-pleural pressure
- Slides: 38