South East regional Hospital Orientation South East Regional







 is the heart")










 MONDAY –FRIDAY 1. 2. 3. 4. 5. 6. 7. 8.")









 Any staff member activate duress C-ART response")

















")


- Slides: 52
South East regional Hospital Orientation South East Regional Hospital Orientation D C B A
Objectives SERH Phase 1 Mandatory sessions • Enable participants to gain confidence in knowing what the equipment is , what part of the system it operates and how to operate it EQui. P standard 15. 3 Implementing an organisation-wide systems for work health and safety – Staff education and provision of information 15. 19 ensuring correct organisational response to emergencies and disasters 15. 19. 1 there is evidence of evaluation and improvement of staff training and competencies in emergency procedures including education and orientation
e r Fi & n o i t a u c a Ev
SERH FIRE SYSTEM consists of…. . , • • • Standard sprinkler Heads Recessed sprinkler heads ( isolation rooms and Operating theatre) Anti-ligature Sprinkler Heads Mental Health Smoke detectors Thermal detectors Strobe lights Speakers Mimic Panels WIP Phones EWIS Panel Fire Indicator Panel - operated by the NSW Fire & Rescue or authorised & trained Staff. Fire control Room
Raising The Alarm Break Glass Alarm These are Installed throughout the Hospital corridors and at Mimic Panels – Simple follow the instructions break glass and press here Smoke Detectors The Smoke detectors are installed throughout the hospital ceilings
Fire Detection & EWIS System Mimic Panel The mimic panel will show where a detection /alert has occurred within the hospital. The mimic panel can also display where equipment has been isolated for maintenance and where detections have occurred in the past. The mimic panel should only be used as an indication only and operated by NSW Fire Brigade.
• Warden Intercom Phone. Used by the fire brigade in the event of an emergency to communicate to the main fire indicating panel. All floor WIP phones on each level can only communicate with the main WIP phone located within the Fire Control Room. To operate the WIP phone, the user within the building need only pick up the phone and it will automatically dial to the Fire Control Panel, where it can be answered by a nominated staff member or the Fire Brigade, if they are present within the Fire Control Room. Q. Does the WIP phone connect the outside like a normal telephone ? NO. The WIP phones only connect to the main fire indicating Panel (FIP) within the Fire Control Room only
Fire Detection & EWIS System The Main Fire Indicating Panel (FIP) is the heart of the fire system and the main point of the fire brigade in the event of an emergency. The FIP informs the brigade of all actions happening with the fire systems and location of the issue. EWIS Panel The EWIS panel is located within room SA 011639 – Fire CTRL Centre which is located on Level 01 to the right of the Entry with an external door. This panel operates the Evacuation System of the Hospital. It also acts as the main communication point of the building for the fire brigade
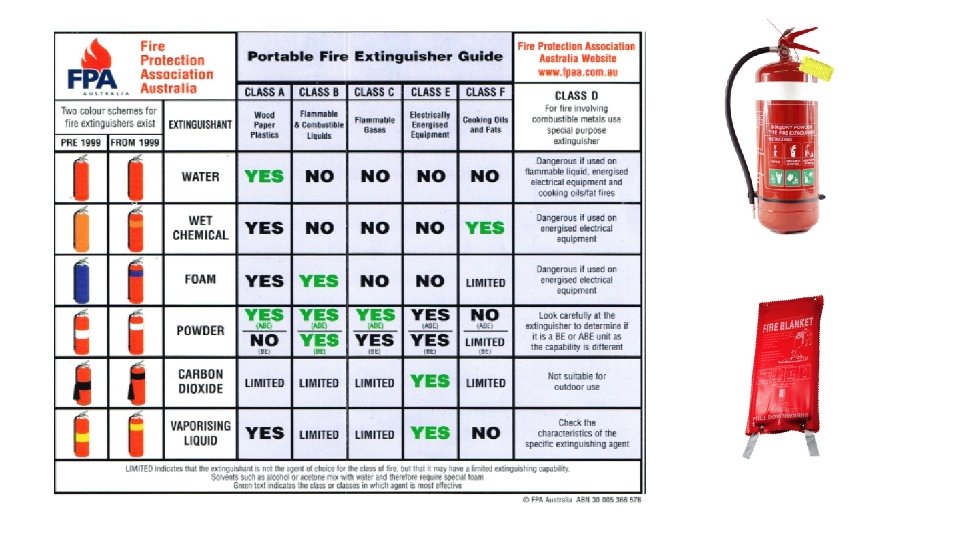
The fire sprinkler, situated in the ceilings is what activates when the heat in the immediate area rises to or above 68 degrees. Unlike the Hollywood movies, only the sprinkler that is most effected by the heat activates, NOT all of them. If the fire is growing and the one sprinkler cannot contain the fire, another one will operate to assist in the containment. WS type wall wetting Fire Sprinkler heads sprinklers Semi-recessed fast These are used to provide response type a higher fire rating to glass sprinkler used windows and doors throughout all general areas and rooms of the hospital. Raven sprinkler. Fully Concealed Clean room Sprinkler These are Institutional type sprinklers used in the Mental Health units of the Hospital. These are used in infection control areas such as Operating Theatres and Isolation Rooms Note: Nothing can be attached to any of the sprinklers such as xmas decoration or signs as this will affect the operation of the sprinkler in the event of a fire
Fire Compartments & Zones Refer to large plans displayed in training room
SERH is divided up into smoke compartments and where a smoke compartment crosses a corridor fire doors are installed. Fire can work its way into or out of a fire compartment if it is intense enough, poorly managed, or not addressed quickly enough. However, fire compartments can still be valuable tools. Anything which slows the speed at which a fire can spread can contribute to fire safety, creating more time for people to evacuate, and potentially reducing fire damage. Strobe Light Installed throughout the Hospital in the ceilings. They indicate that the fire detection system is in alarm, when the area is in evacuation phase. Magnetic door holder device These hold the fire doors open during normal operation and release the doors in the event of a fire alarm. Magnetic door release
STEPS WET SYSTEM DRY SYSTEM – MENTAL HEALTH STEPS 1 Sprinkler activation Single detection activation Double detection activation Single/double detection activation 1 2 Evacuation phase Warning phase within the affected zone Hospital staff investigation period Evacuation phase within affected zone General fire trip (interface with other services) Fire brigade alarm notifications Fire brigade alarm / notification Fire alarm no fire present Fire brigade alarm / notification After 3 minutes (10 mins max. ) Hospital staff isolate warning tones After 3 minutes (10 mins max. ) 3 Evacuation phase cascade to the remaining building – horizontal and vertical 4 3 4 Evacuation phase within the affected Brigade investigate and reset Evacuation phase cascade to zone and warning within the adjoining fire panel and disable the remaining building – zones evacuation phase horizontal and vertical 5 After 3 minutes (10 mins max. ) 5 6 Evacuation phase cascades to the remaining zones on the floor 6 7 After 3 minutes (10 mins max. ) 7 8 Warning/Evacuation to the remaining building- vertical 8
RESPONDING
FIRE WARDEN ROLE In charge Of Shift make sure you’re familiar with all escape routes and exits from your search area, including disabled refuges • • • Remain Calm and reassure others do not leave area, unless in immediate danger note location of the alarm - seen on the mimic panel If fire is in another area alert your staff and standby to receive instruction via the WIP phone If the alarm is in your area, • direct staff to check all rooms including toilets shower cupboards and report back to you • Never place yourself in danger, Initiate R. A. C. E and feedback via the WIP phone (red) • If requested to assist by senior on site coordinator proceed to assist only if it is safe to do so • When instructed evacuate patients /visitors in the following order a) ambulant patients who can help themselves b) Semi Ambulant patients who require assistance c) Non ambulant patients d) Non compliant DO NOT RETURN to the building once the evacuation has been completed without authorisation of the Senior NSW Fire & Rescue Officer.
Nurse Manger/ HASA response to Fire Alarm Activation In Hours After Hours • Administration /HASA proceeds directly to the main entrance to man the entry &prevent people visiting as well as directing the fire brigade to the fire location takes direction Deputy Do. NM (NM) • HASA proceeds directly to the main entrance to man the entry &prevent people visiting as well as directing the fire brigade to the fire location takes direction AHNM • Deputy Do. NM directly to the Fire Control Room • Phones 000 to verify notification • Checks fire indicator panel & EWIS to identify affected area • Communicate to area in alarm mode using the WIP Phone to ascertain situation • Decision point to either turn EWIS into stand by mode OR • Leave alarm to escalate into evacuation mode Operating the Isolating warning tones in the EWIS is only to be done by the Fire Brigade or authorised trained staff. NB Operating the Isolating warning tones in the EWIS is only to be done by the Fire Brigade or authorised trained staff. • AHNM proceeds directly to the Fire Control Room • Phones 000 to verify notification • Checks fire indicator panel & EWIS to identify affected area • Communicate to area in alarm mode using the WIP Phone to ascertain situation • Decision point to either turn EWIS into stand by mode OR • Leave alarm to escalate into evacuation mode Operating the Isolating warning tones in the EWIS is only to be done by the Fire Brigade or authorised trained staff. NB Operating the Isolating warning tones in the EWIS is only to be done by the Fire Brigade or authorised trained staff. When the alarm/fire situation is over ensure all areas are advised of the “ all Clear” via the PA system DO NOT RETURN to the building once the evacuation has been completed without authorisation of the Senior NSW Fire & Rescue Officer.
EVACUATION ASSEMBLY POINTS - Proposed Points to be confirmed Assembly Point 1 Assembly Point 4 Assembly Point 3 Assembly Point 2
Medical Emergency Team
Medical Emergency Team (MET) MONDAY –FRIDAY 1. 2. 3. 4. 5. 6. 7. 8. Medical Registrar Nurse Manager – ( Deputy Do. NM) - Nursing Unit Manager - of that unit - (Control/ crowd) Registered Nurse – Critical care ( Advanced Life support ) Team leader Registered Nurse - Critical care Advanced life support Registered Nurse - Basic Life Support ( RN/EN caring for patient) - Scribe HASA/Wardsperson CNE In a supportive teaching capacity AFTER HOURS 1. 2. 3. 4. Career Medical officer ( Emergency) After Hours Nurse Manager Registered Nurse In-charge of Shift Registered Nurse – Critical care ( Advanced Life support ) Team leader 5. Registered Nurse - Critical care Advanced life support 6. Registered Nurse - Basic Life Support ( RN caring for patient) - Scribe 7. HASA/Wardsperson
MET CRITERIA • All cardiac or respiratory arrest • Airway obstruction or stridor • Unresponsiveness If In doubt press the red EMERGENCY BUZZER Page MET TEAM on 000 to activate a rapid response RAPID RESPONSE CRITERA Any observation in the red zone Deterioration not reversed within one hour of clinical review Increasing oxygen requirement to maintain oxygen saturations greater than 90% Patient deteriorates further before during or after clinical review Arterial blood gas Pa. O 2<60 or Pa. CO 2>60 or p. H , 7. 2 or BE <. 5 Venous Blood gas Pa. CO 2 >65 or p. H <7. 2 Only responds to pain (P) or sudden decrease in level of consciousness on the GCS of 2 or more points Seizures Low urine output<200 ml over 8 hours or , 0. 5 ml/Kg/hr via IDC persisting for 8 hours Blood glucose level less than 4 mmol/l or. 20 mmol/l with a decreased level of consciousness Lactate > or equal to 4 mmol/l Serious concern by any patient or family member Serious concern by any staff member Page MET TEAM on 000 to activate a rapid response
Yellow Zone Clinical review Red Zone Rapid response Medical Emergency Response ESCALATE to NUM I/C Clinical review within 30/60 PAGE 000 Rapid RESPONSE Emergency Buzzer Rapid RESPONSE
Community Primary Care Dental, Oncology, Community Mental Health Drug & Alcohol Renal Discharge lounge EMERGENCY CALL Activated by pressing Remain with person Initiate Basic Life Support Met Team Responds MET TEAM Medical officer decision to transfer to emergency Department EMERGENCY PAGE 000
ACTIVATING A Rapid response • Danger to self • Response • Send for Help • Airway • Breathing • Circulation EMERGENCY Page 000 Caring for rest of the patients Here’s the Resus Trolley Staying with The patient initiate BLS
CO MM UN ICA TIO N • MET TEAM PAGE HANDOVER • • • Medical registrar to CMO @ 1630 hrs Monday to Friday Nurse Manager to After Hours Nurse Manager 1400 hrs Monday –Friday NUM to registered Nurse In charge of Ward 1400 hrs Registered Nurse T/L to Registered Nurse T/L 1400 hrs & 2130 7 days a week Registered Nurse - Registered Nurse 1400 hrs & 2130 7 days a week
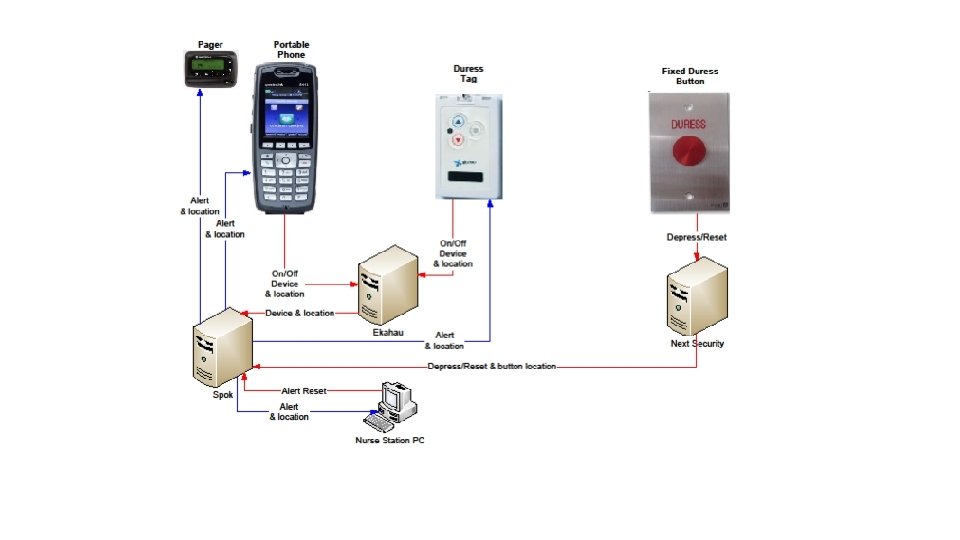
DURESS systems, processes and equipment
• • • Activating the duress system Remain calm do not panic or shout Activate the duress button ( tag, phone, fixed or page) Avoid eye contact do not make any sudden moves Do not take any risks, hand over what is demanded Do not do anything which may antagonise the assailant
Responding to duress Apply your deescalation skills Take direction when the C-ART team arrives Stay calm escalate early Initiate the call for help for self or a colleague
Aggressive incident ( real or imminent ) Any staff member activate duress C-ART response team – responds C-Team HASA, medical officer, Nurse Manager , ALS trained clinician, clinician x 2 ( all having completed the aggressive prevention management training) Nurse Manager/Afterhours Nurse Manager decision point Manages incident Requires external support police activate Report document completed on IIMs Requires Lock down - activate
Clinical Aggression Response Team C-ART Team • In Hours 1. VMO 2. Nurse Manager 3. Registered Nurse – Critical care (ALS) Team leader 4. Registered Nurse - Critical care (BLS/ ALS) 5. HASA/Wardsperson • After hours 1. Career Medical officer (ED) 2. After Hours Nurse Manager 3. Registered Nurse – Critical care (ALS) Team leader 4. Registered Nurse - Critical care (ALS) 5. HASA/Wardsperson NB: all having completed aggressive management prevention training
SECURITY
Security System Overview • Access control system • Intercom system • CCTV System
Access System • Card readers • Wireless readers • Locks • Keypads • Magnetic locks • Exit buttons • Emergency door release • Push buttons • Electric strikes • Duress buttons
CCTV system • Cameras • Except in MH are set to record on motion detection and are recorded by the central server for later review in the event of an incident • 54 cameras cover Carpark, Building entries and intercoms, Hospital street, emergency waiting room, lifts & loading dock • Display monitors • Headend PC and PVR
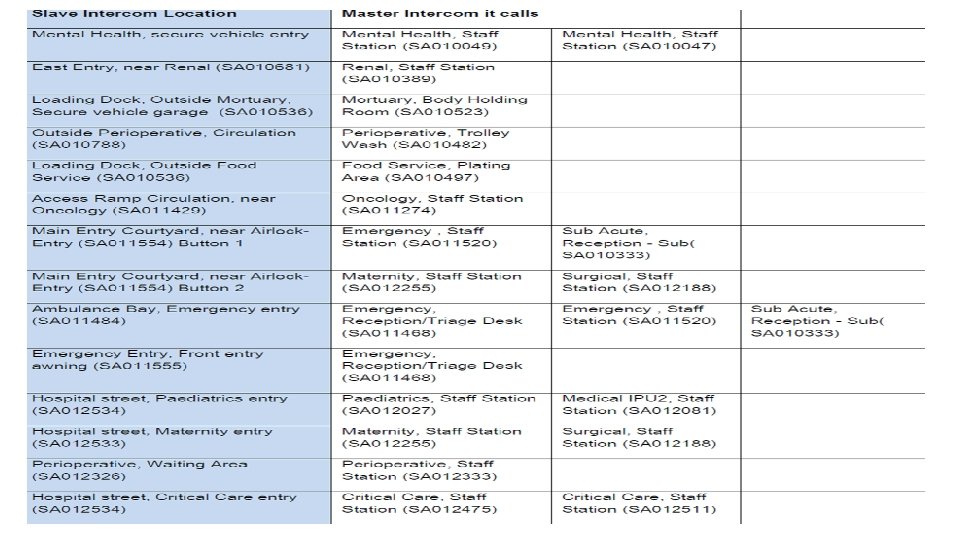
Intercom System • Master and slave intercoms • Slave intercoms are used in areas where people whish to gain access (14 slave Intercom locations) • Master intercoms can be found in nurse stations and security points and are used to give access to people at the slave intercoms ( 22 master slave intercoms)
INTERCOMS • External Intercom stations • Located at key entry points to the hospital • Each external intercom point is provided with CCTV coverage which is displayed on the nurses station screens • A handset is used to answer the call and the door can be remotely unlocked via the handset by pressing 00 (the handsets cannot make external or internal phone calls). • Some intercoms call multiply handsets
PARKING Helipad D Ambulance Site A C B Staff & Visitors Bega Staff On Call Staff Parking CTV coverage Tathra Renal Fleet Loan equipment PTV Oncology , visitors
After Hours Access • The main entry and emergency auto doors will operate on a time schedule providing free entry during working hours and requiring card access, remote door release or intercom access after hours • After hours entry for on call staff will be via emergency • After hours on call staff designated parking - car park A
Staff Lockers • Provided to ensure the security of staff personal belongings • 345 Staff lockers located throughout SERH • All lockers are for the duration of the shift only • Lost keys will incur a replacement fee of $10. 00 Swipe card access • Your swipe card will be programed to reflect your appropriate access level • mandatory training must be completed prior to swipe card being issued • Lost Swipe cards must be reported • Replacement cards incur a fee of $15. 00 • Requests for further access requires your line manager approval
Disaster Emergency Plan Awareness
Disaster • An emergency due to actual or imminent occurrence which: endangers, or threatens to endanger, the safety or health of persons or animals, or destroys/damages, or threatens to destroy/damage any property in NSW, which requires a significant and coordinated response.
Key Concepts • Prevention – Mitigation strategies • Preparation – Disaster planning • Response – Activation • R ecovery – Returning to normality PPRR
Is this a Disaster? • If facilities are faced with a situation that is overwhelming and they are unsure if they have the resources to manage they should call the HSFAC 0477313985 The Local Health District HSFAC is responsible to the NSW State HSFAC.
Communication Cascade for Emergency Management in LHD Local Health District HSFAC LHD Mental Health Service Controller LHD Medical Service Controller LHD Public Health Service Controller Mental health teams Hospital Disaster Controller Public Health Commander Individual Hospital Response Public Health Teams LHD Communication Unit Controller
Emergency Management Who is involved?
Emergency Management Key Stakeholders Emergency Services Emergency Management Committees Functional Areas POLICE State (SEMC) Health FIRE Chair SEOCON Welfare District (DEMC) Energy & Utility Chair DEOCON Engineering Administrative Officer DEMO Transport AMBULANCE SES RFS VRA Local (LEMC) Chair Local Government Administrative Officer LEMO Ag & Animal Public Information
Stages of Activation • Alert – Disaster situation possible: there is an increased level of preparedness. • Stand-By – Disaster situation probable: available for immediate deployment. • Call-Out – Disaster situation exists: there is deployment. • Stand-Down – Disaster situation is contained. NB. THE AREA HSFAC SHOULD BE NOTIFIED BY THE HOSPITAL DISASTER CONTROLLER AT ALL STAGES OF ACTIVATION
Recovery • You will be notified of Stand-Down by the Hospital Disaster Controller • Recovery is the coordinated process of supporting disaster affected communities in the reconstruction of the physical infrastructure and the restoration of emotional, social, economic and physical wellbeing