Sonohysterography in abnormal uterine bleeding Dr A Tabatabai

Sonohysterography in abnormal uterine bleeding Dr. A. Tabatabai

using sterile saline solution as a negative contrast medium in conjunction with traditional transvaginal ultrasound. you can image the uterine cavity and evaluate the tubal patency.

it is advantageous over hysteroscopy that it can scan the uterus, ovaries and pelvis at the same time imaging the uterine cavity.

Abdominal or transvaginal sonography can identify myomas and thickened endometrium but is unable to differentiate between the potential etiologies of thickened endometrium, , polyps, submucous myomas, and homogenously thickened endometrium. In combination with endometrial biopsy, it can identify anatomic problems and abnormal pathologic findings.

At transvaginal ultrasonography , the finding of a thickened central endometrial complex, with or without cystic changes, is often nonspecific.

The Thickened endometrium may be a polyp catheter

The Thickened endometrium may be a polyp CYST POLYP With polyps the endometrial-myometrial interface is preserved well-defined, homogeneous, isoechoic to the endometrium

The Thickened endometrium may be a polyp endometrium

The Thickened endometrium may be a Submucosal leiomyomas With myomas the endometrialmyometrial interface is distorted broad-based, hypoechoic,

sonohysterography can accurately depict the percentage of the fibroid that projects into the endometrial cavity

The Thickened endometrium may be an endometrial hyperplasia Endometrium thickness = A-B A B diffuse thickening of the echogenic endometrial stripe without focal abnormality

The Thickened endometrium may be a Secretory endometrium + +

Endometrial cancer is typically a diffuse process, but early cases can appear as a polypoid mass

sonohysterography, allows identification of intracavitary lesions and focal or diffuse endometrial abnormalities and helps determine whether an abnormality is endometrial or subendometrial.

At transvaginal US, when the endometrium cannot be accurately measured or when there is a nonspecific thickened central endometrial complex, sonohysterography can provide additional information and can be used to direct the patient to a visually guided hysteroscopic procedure rather than a potentially unsuccessful blind biopsy procedure.

Transvaginal ultrasound and transvaginal sonohysterogram are both more accurate in diagnosing the location of fibroids than hysteroscopy [A]. New Zealand Guidelines Group

low-tech low-cost Well tolerable no radiation exposure Effective
 33. 3% Laughhead&stones • Pain (menstrual")
Adverse Events • Discomfort • Cramping( minor ) 33. 3% Laughhead&stones • Pain (menstrual like ) (sever pain ) 11. 5% Cecinilli et al • Infection 2. 5% Dubinsky et al

Effectiveness To compare the effectiveness of an Investigatory procedure assessing the endometrium. Hysteroscopy with biopsy is regarded as the "gold standard"

Effectiveness In 10 studies where sonohysterographic findings were compared with surgical findings and histological assessment (hysteroscopy +biopsy OR hysterectomy ) it was found that SIS has high Sensitivity and specificity for evaluation of abnormal uterine bleeding. Sensitivity 94. 9% Specificity 89. 3% (level II evidence)

Author Year n Sensitivity % Bonilla-Musoles 1992 96 Syrop Parsons 1993 14 1993 58 Widrich 1995 130 96 Wolman 1996 47 Keltz 1997 34 Bernard 1997 109 96 100 99 Schwarzler 1998 104 87 Williams 1998 39 Dijkhuizen 2000 50 100 96 100 Specificity % 97 100 94 100 100 76 91 85 85

Effectiveness It benefits clinical decision making, as up to 40% of patients will avoid diagnostic hysteroscopy.

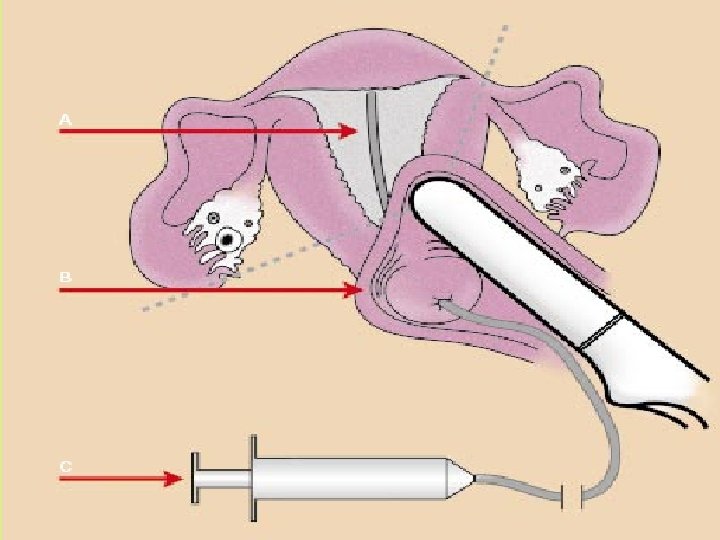
How it works

How it works only preparation necessary was for the patient to empty the bladder.

A speculum, is used to expose the cervix, which was then cleansed with an iodine swab

Various catheter types may be used, including: • 5 -F catheter, with or without an occlusive balloon • pediatric feeding tubes, • insemination catheters, • Goldstein sonohysterography catheter

A catheter, is important to be flushed with sterile saline solution before being inserted to prevent the introduction of echogenic air bubbles.

The catheter can be inserted through the side of a standard speculum, rather than down the channel, for easier removal of the speculum.

Advancement of the catheter was aided by grasping the end of the catheter 2 to 3 cm from the tip with a ring forceps and gently feeding it through the cervical os to position the tip beyond the endocervical canal. The speculum was then carefully removed while the catheter was left in place.

the covered transvaginal probe was inserted into the vagina, and continuous scanning in the Sagittal and coronal or transverse planes was performed during instillation of sterile saline solution. only 2– 5 m. L are actually needed to distend the cavity adequately

Cervical leakage is common, and it is helpful to have two 20 -m. L syringes of saline solution available for the procedure.

The most common indication for SIS is abnormal bleeding in pre- and postmenopausal patients.

SIS delineates masses or defects in the uterine cavity.

SIS distinguishes between focal lesions and global endometrial thickening.

There is no contraindication to SIS in Non-pregnant, noninfected women who are bleeding.

Steps should be taken to avoid uterine lavage propelling cancer cells into the peritoneal cavity. using low pressure infusion by avoiding the use of balloons in women at risk for cancer.

The studies show that the use of SIS will benefit clinical decision making, with up to 40% of patients avoiding diagnostic hysteroscopy. Hysteroscopy is a more invasive procedure, and is associated with significant financial cost, as well as physical discomfort.
 recommended that on the strength of evidence pertaining")
MSAC (The Medicare Services Advisory Committee) recommended that on the strength of evidence pertaining to saline infusion sonohysterography, public funding should be supported for this procedure as a second-line diagnostic procedure for abnormal uterine bleeding, when findings from transvaginal ultrasound are inconclusive.

TVS and SHG offer a cost-effective alternative to diagnostic hysteroscopy in the evaluation of patients aged 40 years or older with abnormal uterine bleeding. The authors concluded that their study suggests that SIS is a more sensitive test than diagnostic hysteroscopy for evaluating abnormal uterine bleeding. Saidi M H, Sadler R K, Theis V D, Akright B D, Farhart S A, Villanueva G R. Comparison of sonography, sonohysterography, and hysteroscopy for evaluation of abnormal uterine bleeding. Journal of Ultrasound in Medicine, 1997; 16(9): 587 -591.

Sonohysterography was in general the most accurate test. Its diagnostic accuracy was markedly superior for polypoid lesions and EH, with total agreement with the gold standard. In diagnosis of intrauterine adhesions, SHG had limited accuracy, similar to that obtained by HSG, with a high false-positive diagnosis rate. Fertil Steril. 2000 Feb

Saline infusion sonohysterography is more accurate in diagnosing submucous fibroids and endometrial polyps in the patients of abnormal uterine bleeding than is TVS should be included in the standard protocol for the management of AUB. Saline infusion sonohysterography should be reserved for those patients who have centrally located fibroids as they may be submucous. Aust N Z J Obstet Gynaecol. 2002 Nov

Conventional transvaginal pelvic sonography does not appear to be a screening procedure of sufficient diagnostic value in the symptomatic patient with abnormal vaginal bleeding. In patients presenting with the chief complaint of abnormal vaginal bleeding, diagnostic evaluation with a saline hysterosonogram may be warranted despite normal findings on a transvaginal pelvic sonogram. AJR Am J Roentgenol. 2002 Jan

Thank you
- Slides: 44