SON 2111 Abdominal Sonography 1 Lecture 6 The

SON 2111 Abdominal Sonography 1 Lecture 6 The Biliary Tree and Gallbladder Part 1 Holdorf

Outline Part I � Normal anatomy � Diffuse wall thickening � Categories of Jaundice � Sludge � Cholelithiasis � Acute cholecystitis � Chronic cholecystitis � Emphysematous cholecystitis � Gangrenous cholecystitis � Emphysema of the gallbladder � Gallbladder perforation � Acalculous cholecystitis � Milk of calcium bile (Limy bile) � Gallbladder polyps � Porcelain Gallbladder � Hydrops of the gallbladder � Cholesterolosis

OUTLINE PART 2 � Gallbladder carcinoma � Adenomyomatosis � Biliary obstruction � Common duct measurement � Dilated Intrahepatic ducts � Fatty meal � Level of obstruction � Choledocholithiasis � Mirizzi syndrome � Bile duct carcinoma � Cholagnitis � Biliary atresia � Pneumobilia � Choledochal cyst � Caroli’s disease � Pancreatic adenocarcinoma � Laboratory values

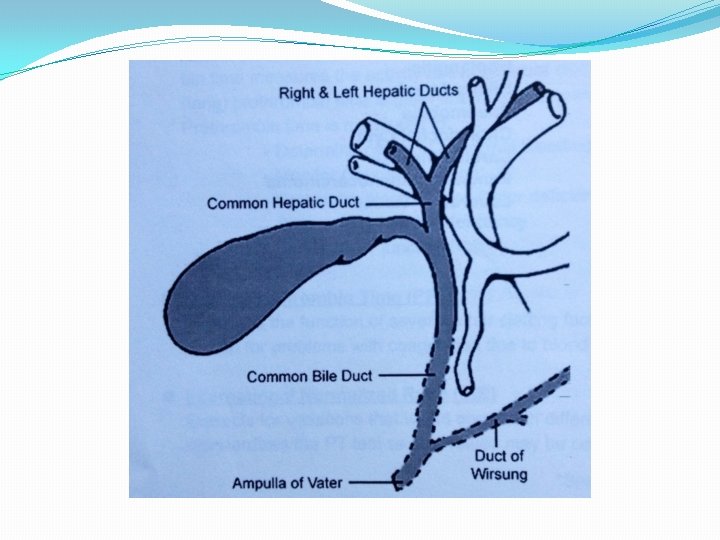
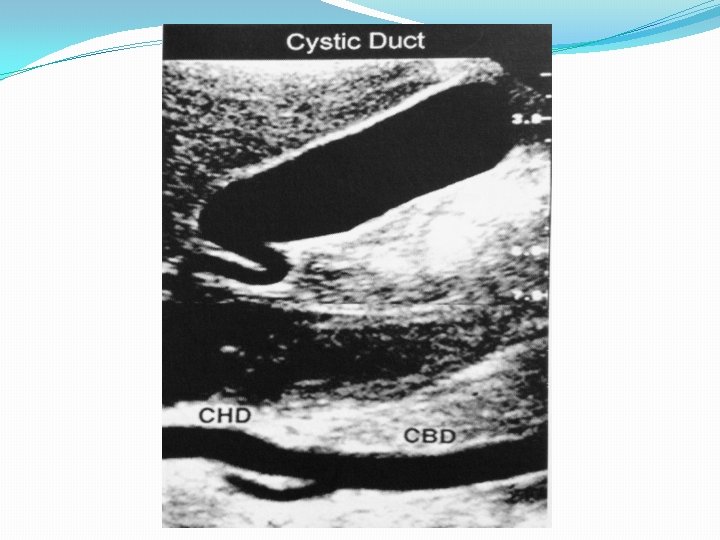
Normal Anatomy �Intrahepatic bile ducts converge to form the right and left hepatic ducts. �The right and left hepatic ducts join to form the common hepatic duct (CHD). �The gallbladder is located at the inferior end of the main lobar fissure. The neck tapers to form the cystic duct which joins with the common hepatic duct (CHD) to form the common bile duct (CBD). �The common bile duct and the main pancreatic duct (Duct of Wirsung) join to form the ampulla of Vater. �It is uncommon to see the cystic duct on ultrasound. Thus, we use the term, “Common Duct” to refer to the extrahepatic ductal system.

Gallbladder � Normal distended Gallbladder is 7 cm to 10 cm long and no more than 3 cm in diameter. � Pear or teardrop shaped sac. L=8 cm or less. Transverse =5 cm, on a fasting patient. � Walls no more than 3 mm. � Bile capacity is 30 -60 ml. � GB is located in the plane of main lobar fissure in the Gallbladder fossa on the visceral surface of the liver lateral to the second part of the duodenum, anterior to the right kidney and transverse colon. � It is predominantly intraperitoneal and is divided into neck, body and fundus. Narrowest portion is neck lying right to the Porta hepatis. Body is the main portion. The position of the fundus can vary considerably. � Normally the Cystic duct should not be imaged with ultrasound. � For the CBD: (1 mm per decade rule) Normally 3 mm.

Gallbladder �Blood supply : cystic artery arising from Right Hepatic vein. Increases in size in acute cholecystitis. �Prep: Minimum of 4 hours NPO. Ideally, 8 hrs NPO. �Causes of non visualization of the GB: - contracted- thick walled, obscures luminal distension - Removed - chronic cholecystitis

�Homework: Show an image of a normal gallbladder in Sagittal and transverse views.

Physiology Biliary system is responsible for transportation, storage and concentration of Bile produced by the hepatic parenchyma. Bile consists of bile acids, cholesterol, lecithin, mucin and Cholecystokinin (CCK) secreted by proximal small intestine. CCK Causes GB to contract and sphincter of Oddi to relax. Bile helps emulsify and absorb fat and facilitate action of the pancreatic enzyme-Lipase. Lab Tests: ALT/SGPT: is more increased in biliary obstruction Alkaline phosphatase markedly increased in obstructive jaundice. LDH moderately increased in obstructive jaundice CCK: Cholecystokinin – a digestive enzyme.

Lactate dehydrogenase �LDH is most often measured to check for tissue damage. �The protein LDH is in many body tissues, especially the heart, liver, kidney, muscles, brain, blood cells, and lungs. �Other conditions for which the test may be done include: Low red blood cell count (anemia)

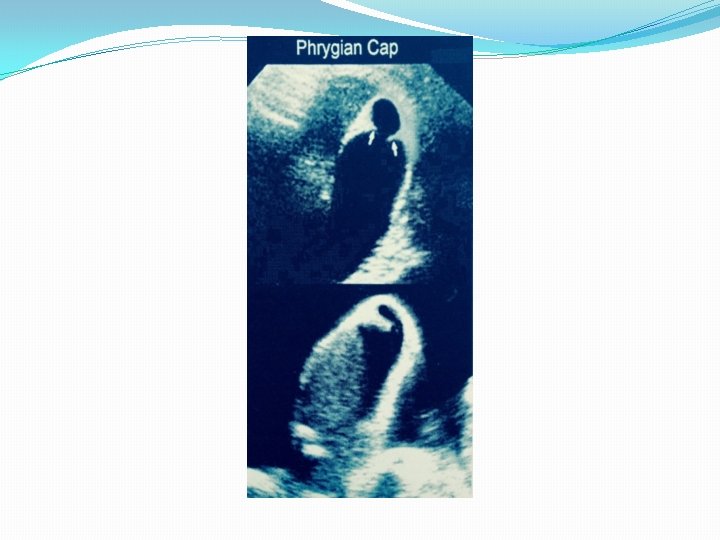
Gallbladder Variants � Hourglass shape � Hartman’s pouch: infundibulum in the neck. � Phrygian cap: kink in the fundus or folds back on the body � Junctional fold or septations in the body of the GB. � Excessively mobile or ectopic: eg. midline, low, left of midline, situs inversus.

Cholescintigraphy Nuclear Medicine Test for GB Function �Is most commonly used to diagnose problems with the gallbladder when other more commonly-performed tests, particularly Ultrasonography, are normal. Cholescintigraphy can be modified with the addition of an intravenous injection of Cholecystokinin, the hormone that is normally released by the body after a meal. � This hormone causes the gallbladder to contract and squeeze out its bile into the intestine. Reduced contraction of the gallbladder following Cholecystokinin (i. e. , reduced emptying of the gallbladder) may mean that there is disease of the gallbladder itself, particularly inflammation or scarring of the wall.

Congenital anomalies �Agenesis �Duplication �Septated

Histologically : � The Gallbladder consists of an inner epithelial mucosa with folds(found only in the neck and cystic duct where its called spiral valves of Heister), then a muscular layer, a subserosal layer and an outer serosal surface(the visceral peritoneum) The Rt and Lt hepatic ducts � hepatic duct immerge from the porta hepatis and unite extrahepatically to form CHD. The rt branch of Hepatic artery at this point crosses under the CHD. The CHD then is joined by the cystic duct forming the CBD. � CBD runs posterior to the 1 st part of the duodenum into a groove near the posteriolateral aspect of the head of the pancreas (HOP) just anterior to the IVC. Thereafter, the CBD enters the posteriomedial aspect of the descending portion of the duodenum (second portion). It is joined by the Main pancreatic duct and together they empty through the papilla of Vater at the sphincter of Oddi. � The intrahepatic and pancreatic ducts should be no more than 2 mm. CHD is normally about 3 mm: CBD is 4 to 5 cm in young adults. Also as one gets older with every decade 1 mm is added, for a normal measure of CBD in a sixty year old is 6 mm to 7 mm.

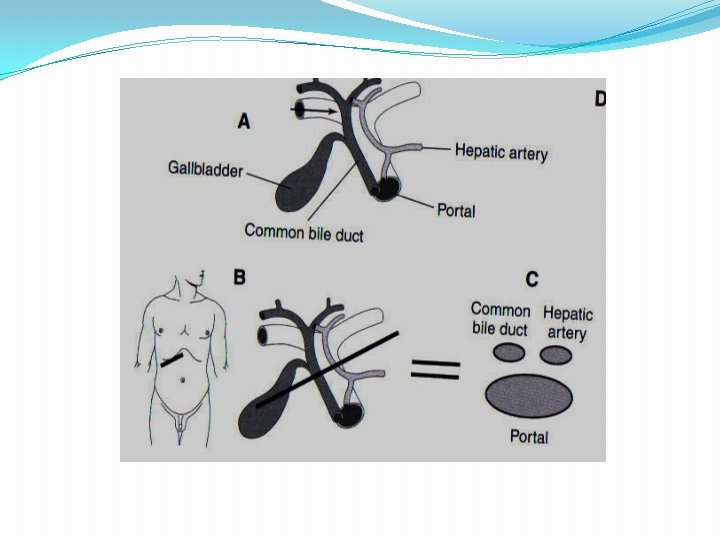
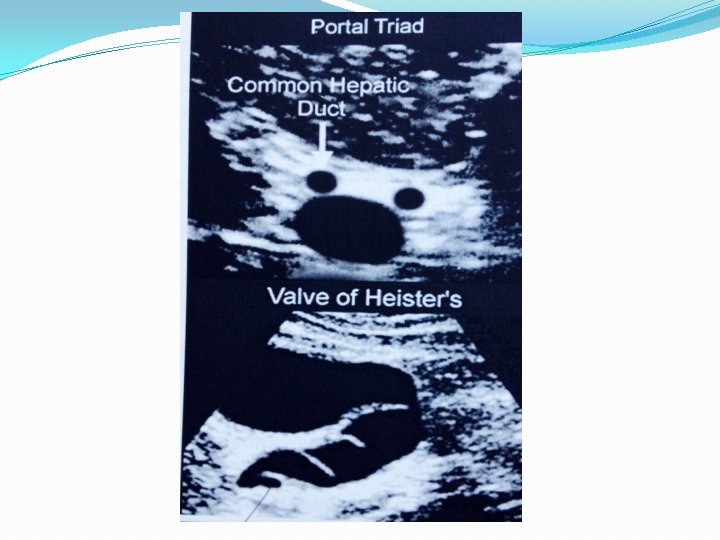
�At the portal hepatis, the portal triad consists of the main portal vein, common hepatic duct, and proper hepatic artery. �Happy sonographers refer to this as the MICKY MOUSE sign. �The gallbladder is divided into the neck, body and fundus. �Valve of Heister is a spiral fold which controls bile flow in the cystic duct. �Hartmann’s pouch is an abnormal sacculation (diverticulum) of the neck of the gallbladder.
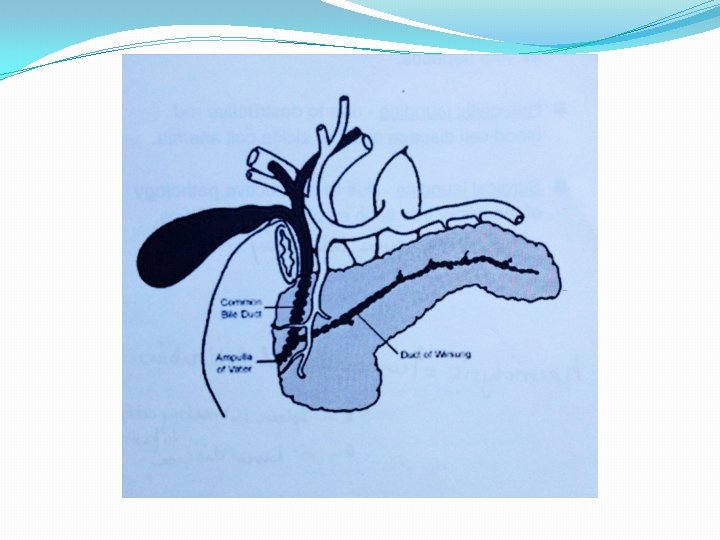

�A Phrygian cap is a fold in the fundus of the gallbladder. �A junctional fold is a fold between the body and the infundibulum of the gallbladder. True gallbladder septations are rare. �The CBD passes posterior to the first part of the duodenum and pancreatic head joining the main pancreatic duct (of Wirsung) at the ampulla of Vater. �The ampulla of Vater empties through the duodenal papilla, controlled by the sphincter of Oddi.

Diffuse Wall Thickening �Gallbladder wall thickness less than 3 mm is considered normal in a properly distended gallbladder. �Most common causes of gallbladder wall thickening is cholecystitis. �Other causes include: �Hypoalbuminemia �Ascites �Hepatitis �Congestive Heart failure �Pancreatitis

Categories of Jaundice �Hepatic jaundice: due to hepatic disease such as viral hepatitis. �Hemolytic jaundice: Due to destructive red blood cell disease such as sickle cell anemia. �Surgical jaundice: Due to obstructive pathology of the biliary tree such as choledocholithiasis.

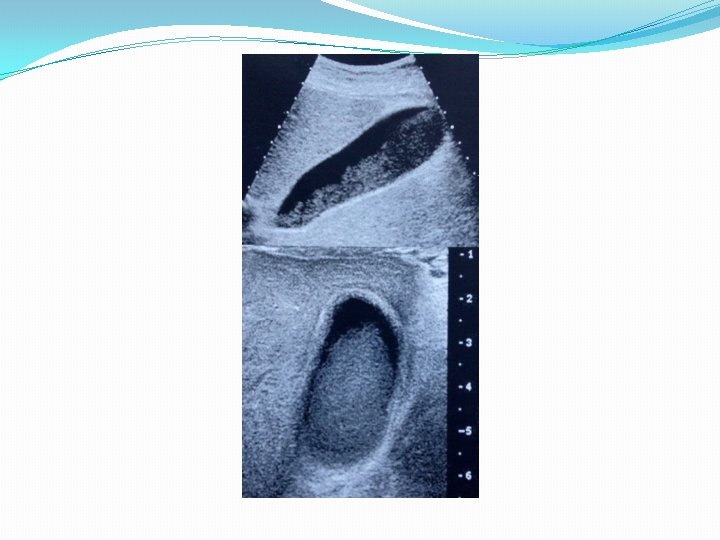
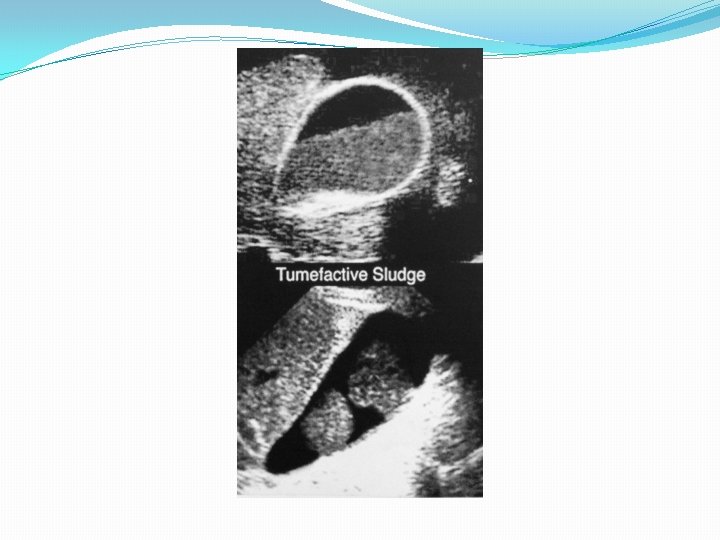
Sludge �Calcium bilirubinate granules and cholesterol crystals make up biliary “Sludge”. �Associated with biliary stasis secondary to prolonged fasting, hyperalimentation (overeating) hemolysis (rupturing of RBCs) cystic duct obstruction, or cholecystitis. �Appears as nonshadowing, echogenic material which layers and shifts with patient position. �Sludge balls (Tumefactive sludge) – organization of sludge.

Cholelithiasis �Sonographic criteria include: �Mobile �Strongly echogenic �Acoustic shadowing Gallstones are composed of Cholesterol Calcium bilirubinate Calcium carbonate

Gallbladder Stone Differentials �Spiral valves of heister �Edge artifact �Junctional fold �Loop duodenum �No movement = possible polyp
 �Gallbladder perforation")
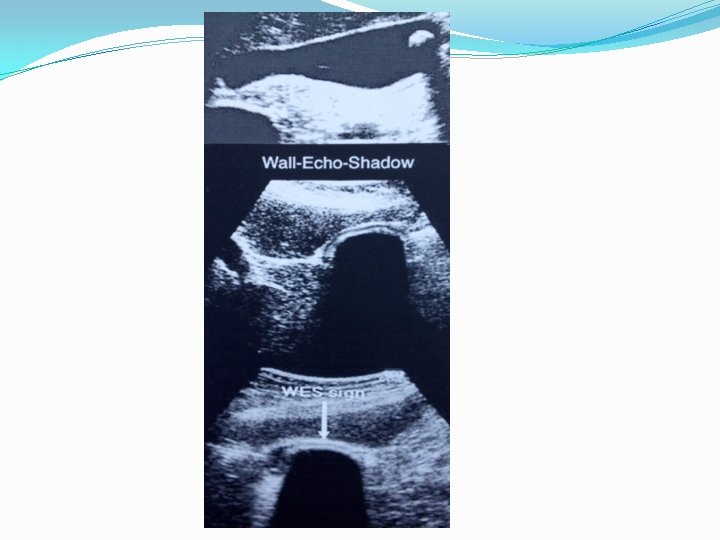
�Cystic duct obstruction may result in: �Acute cholecystitis �Empyema (Accumulation of puss) �Gallbladder perforation �Peri-cholecystic abscess �Bile peritonitis �A gallbladder filled with stones may be seen as a strong shadow in the right upper quadrant. This is called the double arc or WES sing: Wall-Echo-Shadow

Acute Cholecystitis �Gallbladder wall inflammation due to cystic duct obstruction by a gallstone. �Associated with right upper quadrant pain, fever and leukocytosis (WBC count above the normal range). �Features of acute cholecystitis �Gallstones �Murphy’s sign �Diffuse wall thickening �Gallbladder dilatation �Sludge
 �Gangrenous cholecystitis �Gallbladder perforation �Peri-cholecystic abscess Bacterial infection is")
�Complications include: �Empyema (puss accumulation) �Gangrenous cholecystitis �Gallbladder perforation �Peri-cholecystic abscess Bacterial infection is secondary to initial obstruction and ischemia. Associated with Cholelithiasis in approximately 90 -95% of patients Acalculous cholelithiasis in approximately 5 -10% of patients

Chronic Cholecystitis �Defined clinically as chronic gallbladder disease, characterized by recurring symptoms of biliary colic due to multiple previous episodes of acute cholecystitis. �Sonographically, does not appear different from acute cholecystitis. Findings may include a thick-walled, contracted gallbladder. �Sludge and an obstructing cystic duct stone may be present.
 artifacts")
Emphysematous Cholecystitis �Acute cholecystitis due to gallbladder wall ischemia and infection. �Comet-tail (reverberation) artifacts are seen due to the presence of gas within the wall/lumen of the gallbladder due to gas-forming bacteria. �Occurs more commonly in diabetic men.

Gangrenous Cholecystitis �Gangrenous – tissue loss due to decreased blood supply. �There are no specific ultrasound findings to define gangrenous cholecystitis. �Signs suggestive of gangrenous cholecystitis include: �Asymmetric wall thickening �Wall striations �Pericholecystic fluid

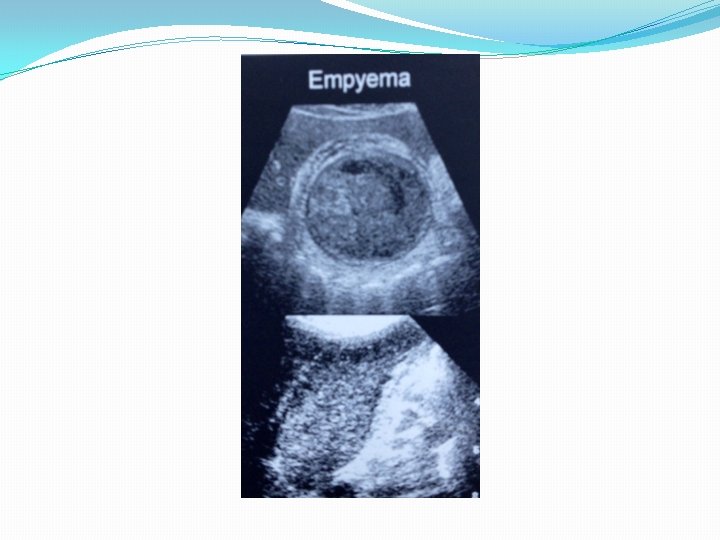
Empyema of the gallbladder �Purulent material within the gallbladder due to bacteria-containing bile associated with acute cholecystitis. �Initiated with obstruction of the cystic duct �Symptoms are the same as with acute cholecystitis with the addition of fever. �Sonographically, it should be suspected in the appropriate clinical setting if atypical bile echoes are seen.

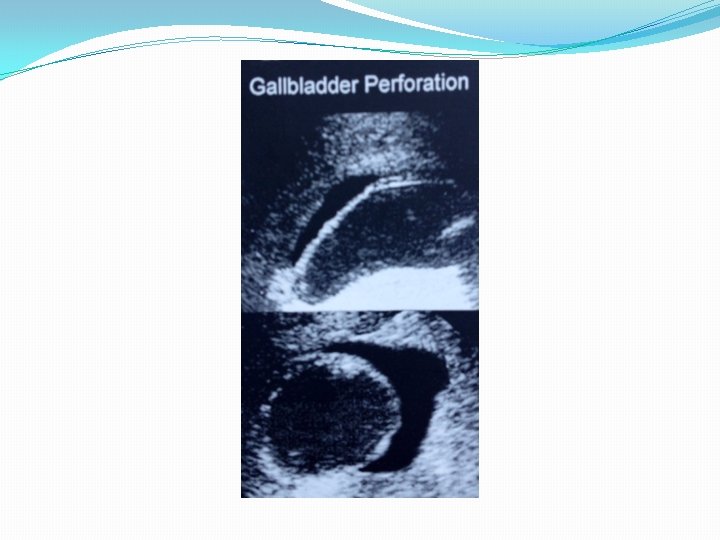
Gallbladder perforation �A complication of acute cholecystitis. �Localized fluid collection in the gallbladder fossa. �Complications include: �Peritonitis �Peri-cholecystic abscess

Acalculous Cholecystitis �Acute cholecystitis without the presence of gallstones. � 5 -10% of cases of acute cholecystitis. �Associated with existing conditions such as �Prolonged total intravenous nutrition. �Abdominal surgery �Severe burns �Sepsis �AIDS
 �Sludge-like material with a high concentration of calcium.")
Milk of Calcium Bile (Limy bile) �Sludge-like material with a high concentration of calcium. �Associated with chronic cholecystitis and gallbladder obstruction of the cystic duct. �May be seen as a fluid-fluid layer that results in distal acoustic shadowing.

Porcelain Gallbladder �Calcification of the gallbladder wall �Associated with chronic cholecystitis

Hydrops of the Gallbladder �Also known as mucocele of the gallbladder �A round, distended, non-inflamed gallbladder due to obstruction of the cystic duct. �Bile is reabsorbed and the gallbladder is filled with an anechoic secretion from the mucosa. �Asymptomatic, presenting as a palpable RUQ mass. �The clinical signs of cholecystitis are absent. �Small stone blocks the bile flow. �Non wall thickening �GB secretes mucus and is over-filled.

�Homework �Show an image of a hydropic gallbladder.
 are deposited in the gallbladder wall. �These deposits, which")
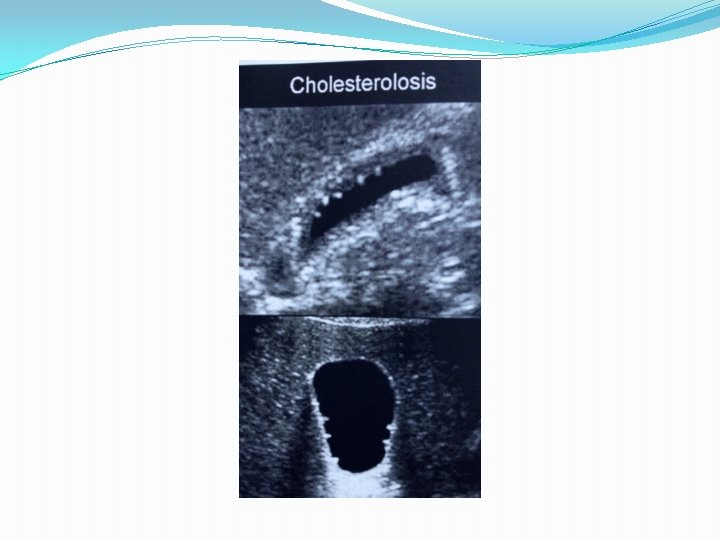
Cholesterolosis �Lipids (triglycerides and cholesterol) are deposited in the gallbladder wall. �These deposits, which appear as polyps, vary in size and can be as large as 1 cm. �This condition is also referred to as “Strawberry gallbladder”, due to the small yellow specks of cholesterol macrophages against the red, bile-stained mucosa. �Looks like light bulbs �Associated with wall thickening

Homework � Define milk of calcium bile. � With what clinical condition is milk of calcium bile associated? � Name three laboratory values that will elevate in association with a biliary obstruction. � What are the two types of gallbladder folding? � What is the purpose of administering a fatty meal to a patient? � What are the two terms that describe a stone-filled contracted gallbladder? � What does a significant elevation of conjugated bilirubin levels indicate? � Gallbladder wall thickening is diagnosed when the wall is greater than ____. � What are the causes for gallbladder wall thickening? � Name the sonographic criteria for gallstones. � Describe the composition of gallstones. � Describe acute cholecystitis � What symptoms accompany acute cholecystitis? � Name the five sonographic criteria that define acute cholecystitis. � What is emphysematous cholecystitis? � Describe the sonographic appearance of emphysematous cholecystitis. � Describe the mechanism of hydrops of the gallbladder.

Rumack Homework Site the page in which you found the answer �What are some normal variants of the gallbladder? �Briefly describe two causes of sonographic nonvisualization of the Gallbladder. �What is biliary sludge? �What is a porcelain gallbladder?

�END PART I
- Slides: 52