Some Neuro Behavioral Treatments for Insomnia catio pli

Some Neuro. Behavioral Treatments for Insomnia catio pli With Im tays S l a t i p s ing Ho v o r p m I ns for Julie Madsen, Psy. D Robert Grove, Ph. D Clinical Psychologists and Neuroscience Consultants

Is this primary insomnia? Do clocks continue to tick while you sleep?

So, is this secondary insomnia? What is the cure?

Is this iatrogenic insomnia? Are you helping heal?

Goals • • • Why do we need sleep anyway? What are common sources of insomnia? What’s new in the neurobiology of sleep? What’s new in insomnia management? How does that relate to pain management? Can we make the hospital a nice place to sleep? And why that’s so critical to healing.

Why Sleep, Anyway? • The idea that sleep confers the same benefit on all creatures is wrong. – SLEEP TIMES ARE SPECIES-SPECIFIC: – The big brown bat, one of the sleepiest animals known, dozes more than 20 hours a day. Giraffes sleep only about 4 hours. – SLEEP-DEPRIVATION ? *Migrating birds and newborn killer whales appear to forgo sleep for several weeks without having to make up for it later. – REM IS NOT UNIVERSAL: *REM sleep has been found in all – terrestrial mammals but not in dolphins and other cetaceans. – birds but not in reptiles, fish, or amphibians. – GROWTH HORMONE SECRETION VARIES: – Humans secrete more growth hormone during slow-wave sleep. – Rats and dogs secrete growth hormone while they're awake. – REM AND ERECTIONS ARE VARY: – Male humans and rats experience erections during REM sleep. – For male armadillos, erections occur only during non-REM sleep

REMEMBER THE BIG PICTURE

Why Sleep, Anyway? Must serve a repair function of some kind: – #1 is in the gut. MMC resets digestion. – #2 in the brain – SWS rests brain health. – #3 is the musculoskeletal system- resets. .

Politics of Insomnia DIAGNOSTICS - FOR INSURANCE PURPOSES: • Transient Insomnias: – Less than 2 weeks • Intermittent Insomnias: – Repetitive episodes of transient insomnia • Chronic Insomnias: – Continuing difficulty with sleep

Practical Insomnias DESCRIPTIONS FOR UNDERSTANDING CAUSES: • Trauma/Worry-induced Insomnias: – Traumatic thoughts prevent normal sleep. – e g Painful Divorce, IRS, kids, etc – 3 day rule • Metabolic Insomnias: – Tight muscles, cramping at night, pain-immobility – Respiratory Disruptions, asthmas, sleep postures – Heightened cortisol levels at night, ADD brain dysfunction, etc. • IATROGENIC INSOMNIAS: • induced by medical interventions • Sleeping pills – dependence and conditioned sleep • Antidepressants – really neural stimulants

Chronic insomnia • 6 months or longer • Average less than 6. 5 hours sleep per day • Or 3 episodes per week of: – Taking longer than 30 minutes to fall asleep* – Waking up during the night for at least an hour • i. e. Primary Insomnia, chronic-type • Not accounted for by another sleep disorder, mental disorder, medical condition or substance use. SIDEBAR: * Stage 2 Sleep is wakeful, hypnogogic, distorted.

How common is insomnia? • SELF-REPORT: More than half of adults in the U. S. experienced insomnia at least a few nights a week during the past year – Nearly one-third had insomnia nearly every night – Insomnia complants increase with age • The most frequent health complaint after pain • Complaint is twice as common in women as in men

PAIN VS SLEEP: INDEPENDENT COMPLAINTS

You probably know this….

There a Lots of Tests for Sleep Disorders

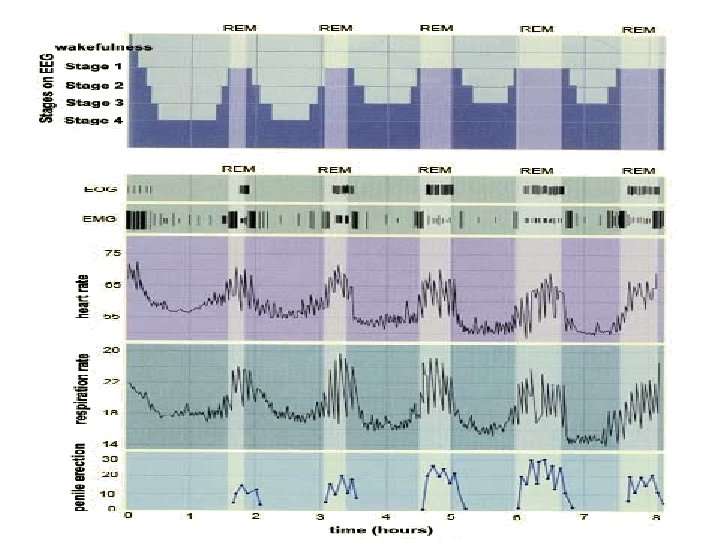
Sleep stages • Five stages, 4 per night – – – Stage 1: Stage 2: Stage 3: Stage 4: Stage 5: Very light sleep Light sleep Deeper sleep Very deep sleep, most restorative REM sleep, when we dream
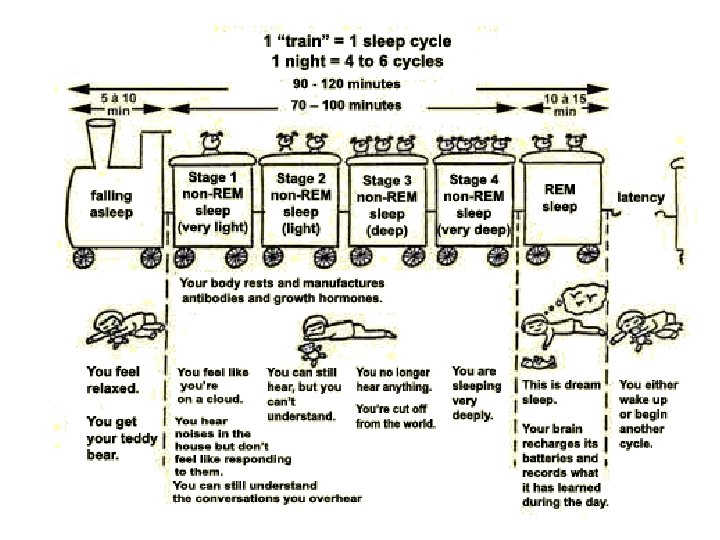

Key Functions of Sleep • Slow. Wave. Sleep- SWS –Growth hormone repairs, heals, energizes cells – basic sleep drive – rest, recovery & homeostasis –Body& blood cell repair, immune system. –Keeps circadian rhythms entrained • Stage 2 Sleep –– Maintains vigilance while sleeping –Hypnogogic, suggestible, distorted time • REM – Memory consolidation –Development of neural connections

REM

Stage 4

HEALTHY NORMAL CONTROL Awake Move REM Stg 1 Stg 2 Stg 3 Stg 4 SLEEP EFFICIENCY: 96. 8% REM LATENCY: 94. 5 min SLEEP LATENCY: 7. 0 min % REM: 13. 3 % STAGE 1: 7. 5 % STAGE 2: 57. 0 % STAGE 3: 16. 9 % STAGE 4: 3. 5

DEPRESSED PATIENT Awake Move REM Stg 1 Stg 2 Stg 3 Stg 4 SLEEP EFFICIENCY: 79. 2% REM LATENCY: 49. 0 min SLEEP LATENCY: 6. 0 min % REM: 16. 9 % STAGE 1: 17. 0 % STAGE 2: 46. 0 % STAGE 3: 0. 0 % STAGE 4: 0. 0

HEALTHY NORMAL CONTROL DEPRESSED PATIENT

How much sleep do you need? • Not everyone needs the same amount of sleep. – Natural short and long sleepers • BUT sleeping less than 6. 5 or more than 9 hours is associated with 1. 7 x greater mortality & risk of disease.

New Data

INSOMNIA AND INFLAMMATION New Data

New Data 1. Sleep Management Health Effects Migrating Myoelectric Complex is disrupted Sleep-deprivation triggers live bacteria in normally sterile tissues. 2. Sepsis occurs without positive blood or tissue tests. Sleep-deprivation produces a progressive, chronic negative energy balance. Sleep-deprivation produces a fatal bloodstream infection without an infectious focus. 3. Non-pathogen bacterial infections increase Sleep-deprivation produces bacterial translocation. http: //ajpregu. physiology. org/cgi/content/abstract/278/4/R 905

Sleep allows Gastro. Intestinal Cleansing Peptides build up
 for")
New Data Sleep-deprivation compromises Gastric Musosa Sprague-Dawley rats were partially sleep deprived (PSD) for 7 or 14 days by housing inside slowly rotating drums. “Sleep deprivation increases • gastric acidity - p. H • noradrenaline • Gastrin • Histamine • decreases gastric mucosal blood flow. ” • It could be one of the risk factors contributing to gastric ulcer formation. Re: bacteri pylori

Slee ws o l l pa

New Data Sleep promotes immunoactivation and healing. “hypnogenic peptides cause fevers and mobilize the body’s immune response. ” Fevers can produce sleep. Infections stimulate cytokines. Cytokines cause an increase in sleep and thus help to increase the body’s immune defenses. ” For example : “Interleukin-1 is an example of these peptides that simultaneously stimulate the immune system and promote sleep. ” So how do you do it in a hospital?

Sleep in middle age • INTERMITENT: Sleep becomes lighter and nighttime awakenings become more frequent and last longer [Western cultures] – Often wake up after 3 hours of sleep – Menopause may lead to hot flashes that interrupt sleep repeatedly • WEIGHT: Breathing problems may begin, especially among overweight people • EXERCISE: Physically active adults sleep more soundly than their sedentary peers. • About 20% of sleep time is spent in dreaming

Sleep is worse in older adults • Dozens of awakenings during the night – Little deep sleep, but dreaming still 20% – ONSET DELAYED: Falling asleep takes longer • Despite the above, over a 24 -hour period older adults accumulate the same amount of total sleep as younger people – Older adults more likely to nap during the day • Older adults do need the same amount of sleep as they did when they were younger

Disorders that can cause insomnia • • Arthritis or any other painful condition Chronic lung or kidney disease Cardiovascular disease (heart failure, CAD) Heartburn (GERD) • Hyperthyroidism • Diabetes • Menopause • Neurological disorders – epilepsy, Alzheimer’s, headaches, stroke, tumors, Parkinson’s Disease SIDEBAR: IATROGENIC INSOMNIA TOO

Bio. Behavioral Causes of Insomnia • Cortisol phase-shifting

Sleep and cortisol I

Sleep and cortisol II
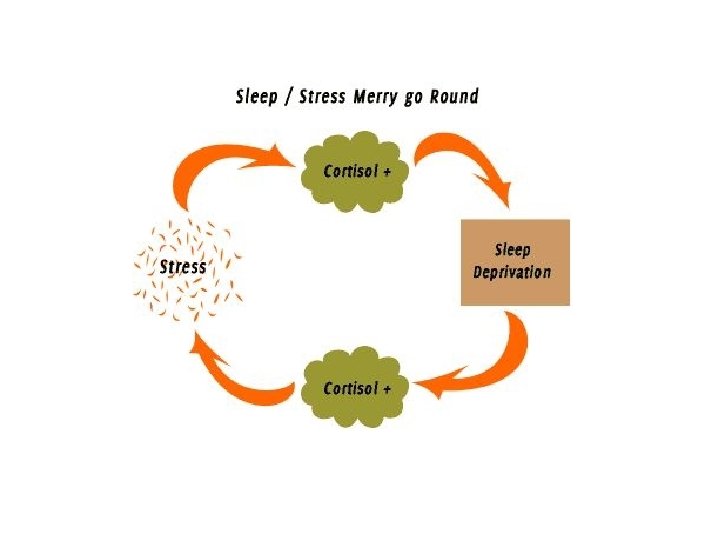

The Cortisol Connection • Moderate Cortisol Levels – – Self-talk includes emotional levels. – Maintains arousal. • Low Cortisol Levels– Self-talk diminishes. – Emotions shut down nautrally* – Reduces arousal

As We Age, Evening Cortisol is Higher. Dreams Deminish, too.

Common Drugs : iatrogenic insomnia • Beta blockers • Calcium channel blockers • Bronchodilators – Humm? • • • Corticosteroids – Humm? Decongestants – Humm? Antidepressants- Humm? Thyroid hormones Anticonvulsants High blood pressure medications * Those in bold print cause Iatrogenic insomnia!

Cultural Causes • Poor sleep habits • Shift work • Shared psychotic disorder- staying up late is fun!

Sleeping Pills and the Magic Bullet • Most common ‘treatment’ approach – Humm? – Drowsiness common the next day – Reassures patient without curing insomnia • NOT meant for chronic insomnia – Effective for insomnia only short-term (a couple weeks) – Tolerance and dependency may develop • SIDEBAR: Conditioning takes place rapidly. – Withdrawal, rebound, relapse may occur
 1 -2 cups")
Good Sleep & Biological Rhythm Hygiene Restrict caffeine (not just coffee) 1 -2 cups before 10 a. m. Warm milk 1/2 hour before bedtime For tryptophan No food or exercise within 2 hrs of bedtime Need clear gut to allow MMC

Non-Drug Treatments Cognitive- Behavior Therapies to manage sleep: – – – Stimulus Control shaping routines Cognitive-distortion correction therapy Sleep Restriction Routines Simple Mental Relaxation Training – not meditation Sleep Hygiene Management Neuro. Behavioral Treatments for sources of insomnia – TM-like Meditation: 10 min twice daily- increases Gamma waves – Biofeedback: 1. SLL, 2. Temperature to 95 degrees- regulate cortisol – Neurofeedback: • 2 protocols – 1. Promote sleep 2. Promote wakefulness – Cardio. Breathing: Heart. Rate. Variability protocols – Capno. Breathing: Correct CO 2 deficiences

Myths about insomnia • Misconceptions about control and predictability of sleep – “I can’t predict when I’ll sleep well or badly. ” • Myths about what behaviors lead to good sleep – “When I have trouble getting to sleep, I should stay in bed and try harder. ”

Sleep Restriction - best if done with a professional • Cut bedtime to the actual amount of time you spend asleep (not in bed), but no less than 4 hours per night • No additional sleep is allowed outside these hours • Record on your daily sleep log the actual amount of sleep obtained

Stimulus Control - You can do this on your own • • Go to bed only when sleepy Use the bed only for sleeping If unable to sleep, move to another room Return to bed only when sleepy Repeat the above as often as necessary Get up at the same time every morning Do not nap

Sleep Hygiene: Environment • Avoid working in bed & set reasonable limit for finishing work prior to bedtime • Avoid serious discussions or arguments prior to bedtime • Avoid working on potentially upsetting things

Sleep Hygiene: Hospital • Avoid working in bed & set reasonable limit for finishing work prior to bedtime • Avoid serious discussions or arguments prior to bedtime • Avoid working on potentially upsetting things

More healthy sleep habits • Adjust the bedroom environment – Sleep is better in a cool room, around 65 F. – Darker is better – If you get up during the night to use the bathroom, use minimum light – Use a white noise machine or a fan to drown out other sounds – Make sure your bed and pillow are comfortable – If you have a partner who snores, kicks, etc. , you may have to move to another bed (try white noise first) Hospital?

‘Mental’ Relaxation training • Engage in any activities that you find relaxing shortly before bed or while in bed – Can include listening to a relaxation tape, soothing music, muscle relaxation exercises, a pleasant image • SIDEBAR: • More effective than no treatment, but not as effective as sleep restriction

TM Meditation and Sleep The trademarked Transcendental Meditation technique can be learned only from a certified teacher. Generic TM-like Meditation is similar. 1. A non-sense phrase is used. 2. Note that thoughts cause the non-sense phrase to go away. 3. It is more acceptable to newcomers to go for 2 ten-minute daily sessions. Hospital?

Computer-Aided Awareness I • Stop Look Listen • Demonstrates how to calm yourself ‘secretly. ’ – Key is how to become aware of arousal within 5 seconds. ’STOP’ – Put aside thought for a moment and LOOK inside. – LISTEN to your arousal. – DECIDE: do you need extra tension now?

Computer-Aided Awareness II • Hand Warming using Tempurature Monitoring. – Stress vasoconstricts, drops finger temp. – Relaxation dilates, increases temperature. – It is impossible to maintain stressful styles while hands warm. – Excellent pre-sleep exercise. – SIDEBAR: May occasionally bring up repressed memories, can’t warm comfortably. Go for detached awareness, not warming per sec.

Hand Warming and Expired CO 2 • Sometimes it is impossible to warm the hands because expired CO 2 levels are too LOW. • SOLUTION: Train to increase CO 2 levels in expired air. • TECHNIQUE: Breathing Training. – Use HR monitoring or – Use Capnometer monitoring

Neurofeedback and Insomnia

Neurofeedback and Insomnia • Usually tired by day, unproductive at night. • Goal is to ‘brighten’ during day with proper brainwaves. • Effect is to become aware of being pseudo -tired during day, and turn on brainwave without needing to be hooked up. • In training, clients find best strategy by trial -and-error.

PRINCIPLES OF CAPNOMETRY

SLEEP AND PAIN • Poor sleep lowers resilience, does not increase pain per sec. • Touch relives suffering, lowers cortisol, good for both. • Medication cocktails often mask suffering, not pain. • Depression here does not mean antidepressants. • If patient is always in bed, he looses stimulus control. • Pain will regress adults to infantile behaviors, revive fears, anger, isolation issues. Accept acting out. • Regegulate cortisol cycle using light-dark cycles, neurobehavioral techniques. • Constant reassurance is necessary- this is neurobiological. Your assurance will elicit better faster recovery.

Neuro. Behavioral Evaluation of Arousal/Recovery : Pain and Sleep Neuro. Behavioral Lab: EEG, EMG, ECG-HRV, Resp, GSR, Temperature. In our Neurobehavioral Lab, we evauate stress/recovery, an indirect estimate ‘cortisol’ shifting important in pain and sleep disorders. • Psychophysiologial Stress Profiling- measures recovery times after stress CRPS- [RSD type] -post 1 yr 10 yo Male Methadone Antidepressants Pain and Sleep

A Caveman’s dream – can you make it out? HINT: The man is on thr right, diagonal to the bison. That’s all, folks!

There May Be Other Ways to Manage Sleep Disorders. Open for Discussion. .
- Slides: 66