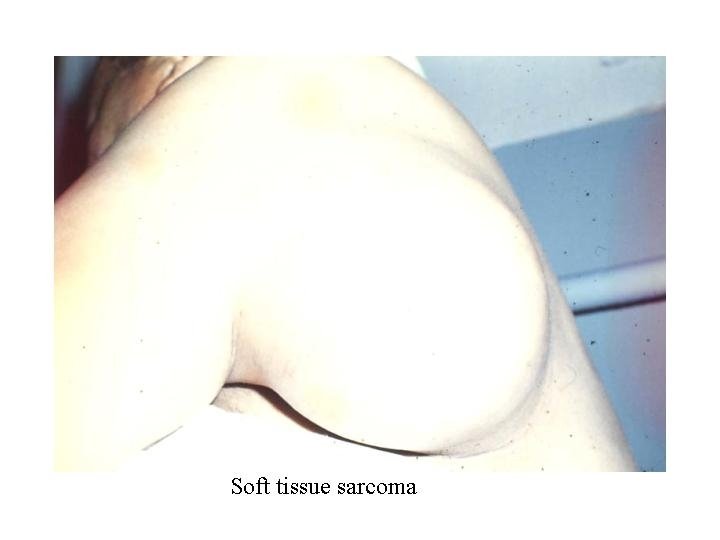
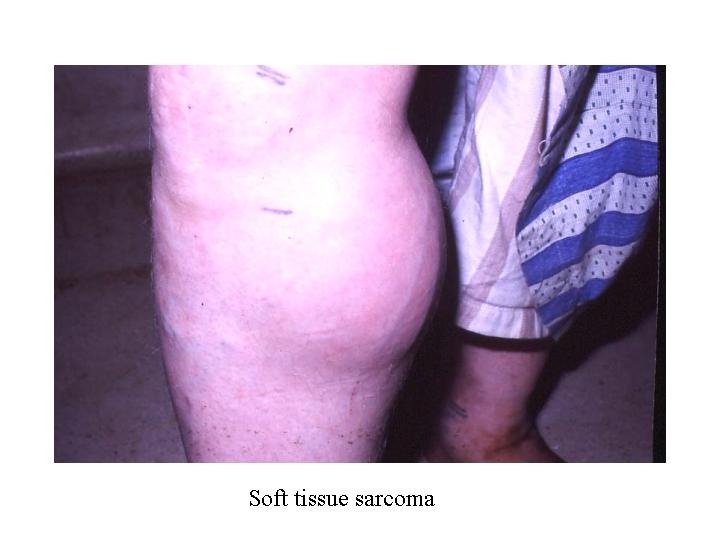
Soft tissue sarcomas of adults Soft Tissue Sarcoma





 Stage G T LN M OAS (5 a) IA")







 • Tumor resection – Radical or compartmental excision –")
 • Should pre operative if – Rapid growth –")
 • Could be used with radio as pre oprative")





 n acute inflammatory response n Prolifaretive")












 Vascular effects Macrovascular")








 n IP = 1 - 3 days n General")
 1. Fulminating 2. Massive ( whole limb) 3. Local")




 1. Meningitis 2. Erysipelas 3. Tetany 4. Rabies 5. Strychnine poisoning 6.")

 n Nursing n Anti tetenic serum n ATS n n n 100.")
 n Stage I n Sedation by luminal or sparine n Stage II")
- Slides: 60
Soft tissue sarcomas of adults
Soft Tissue Sarcoma Epidemiology • Incidence: 2/100. 000 per year • Frequency: 0, 8 -1% of all malignant tumours • Aetiology: widely unknown
Soft Tissue Sarcoma Predisposing Factors • • Ionising radiation Genetic predisposition – Neurofibromatosis – Li-Fraumeni Syndrome – fam. Retinoblastoma – fam. Polyposis coli • Radiation – Increase MFH • Viruses – HIV and kaposi sarcoma • Exposure to chemicals – Phenoxyacetic acid – Chlorophenole – Thorotrast (radioactive) – Vinylchloride – Arsenic • Chron. Lymphatic edema – Stewart-Treves Syndrome
Soft Tissue Sarcoma Histologic Classification
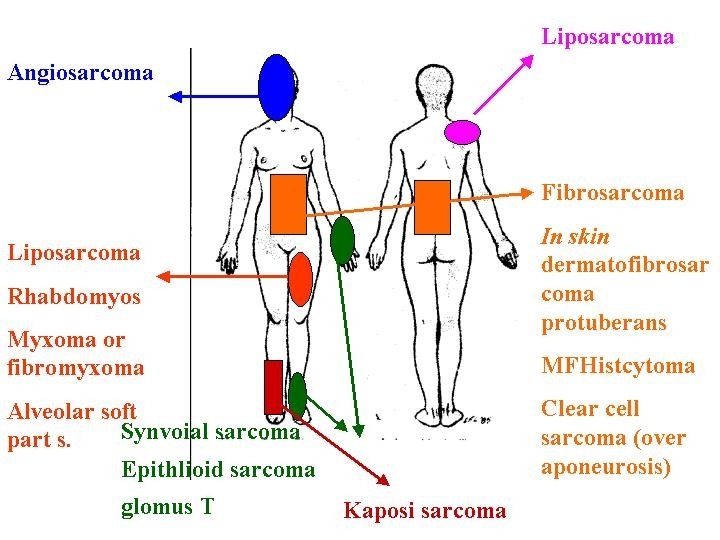
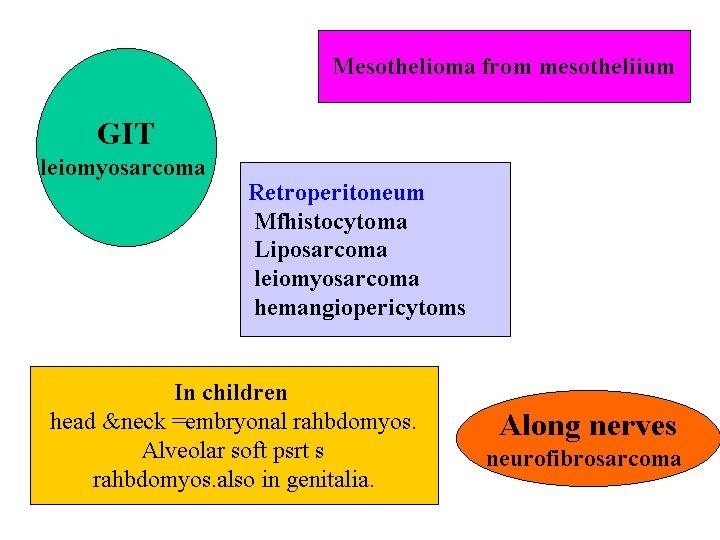
Soft Tissue Sarcoma Localisation
Soft Tissue Sarcoma Stages (UICC) Stage G T LN M OAS (5 a) IA G 1 T 1 N 0 M 0 IB G 1 T 2 N 0 M 0 IIA G 2 T 1 N 0 M 0 IIB G 2 T 2 N 0 M 0 IIIA G 3 -4 T 1 N 0 M 0 IIIB G 3 -4 T 2 N 0 M 0 IVA all G all T N 1 M 0 IVB all G all T all N M 1 79 65 45 10
Clinical presentation • • • Asymptomatic mass Pain and disability Pressure manifestations – – – Arterial Venous Nerves • Metastases – – – Local Blood Lymphatic
Diagnostic work up • Tissue diagnosis – FNABC – True cut needle – Open biopsy • Incisional • Excisional • Imaging – Tumor CT or MRI – Bone plain or MRI – Lung plain or CT
Management of local disease (Surgery) • Tumor resection – Radical or compartmental excision – Wide local excision – Enucleation – Intracapsular • Lymphadenectomy only in epitheliod, angiosarcoma & synovial sarcoma • Amputations • Reconstructions
Management of local disease (Radiotherapy) • Should pre operative if – Rapid growth – High grade – Large size • Should post operative in most tumors except – G 1 – Small G 2
Management of local disease (chemotherapy) • Could be used with radio as pre oprative neoadjuvant • Its use post operative is controversial • Best results with recurrence either loocal or distant
Soft Tissue Sarcoma Therapeutic strategy for adults Local Stage Radical surgery Surgery Metastatic Stage non rad. surgery Surgery +/adj. CT/RT CT +/Salv. Op. neoadj. CT/RT + Surgery Exp. therapy
Soft Tissue Sarcoma CHEMOTHERAPY PROTOCOL IFADIC, q 14 DAYS • DOXORUBICIN 25 mg/m² Day 1, 2 • IFOSFAMIDE 1500 mg/m² Days 1 -4 • DTIC 200 mg/m² Days 1 -4 • G-CSF 5 µg/ kg Days 5 -13
Surgery of the wound and infections
Wound healing process restoration/regeneration n Collagen formation n finroblasts- protocollagen n hydroxylation n Epithelial coverage n Contraction in the tissues n Blood vessels n migration and division n Angiogenesis n Vasculogenesis, in situ.
Wound Healing: Stages n Hemostasis n platelets, endothelial cells, fibrin & fibronectin n Inflammation n neutrophils, macrophages, lymphocytes, growth factors and proteases and cytokines n Proliferation - fibroblasts, epithelial & endothelial n growth factors. n Remodeling - collagenase
Wound healing phases n Lag (24 -48 h) n acute inflammatory response n Prolifaretive (4 -5 weeks) n migration of fibroblasts, capillaries n wound strength: 1 st month 50% 2 nd month 75% 6 th month 95% n Maturation: cross linking, remodelling, contraction
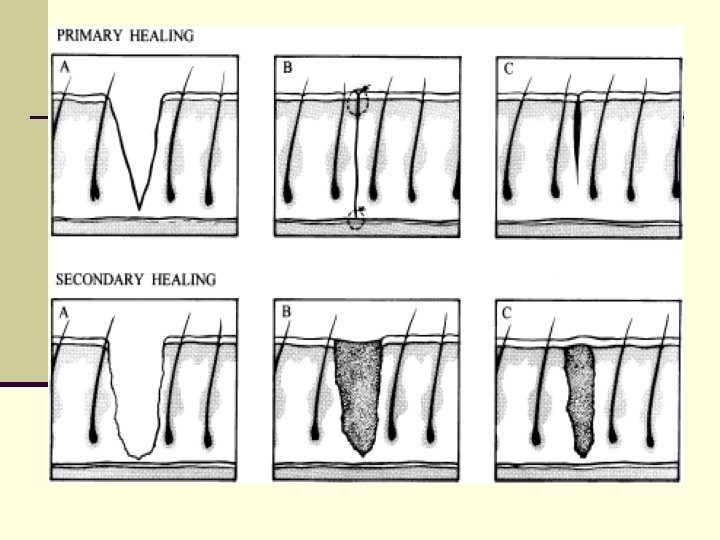
Clinical management n First intention healing n primary closure, epithelisation 48 -72 h n 2 nd intention- contaminated wounds n granulation tissue n 10 000 organism/mm 3 n 3 rd intention- delayed primary closure n 3 -4 days observation, closure
Abnormal wound healing n n n Large, dead space that accumulates fluid, excessive fat that obscures the fascia, BMI>52 poor blood supply, attenuated and weakened fascia, excessive wound tension n chronic lung disease, chronic cough, and vomiting n malnutrition, old age, diabetes (neutrophil dysfunction, and microvascular disease) decreasing phagocytosis, chemotaxis, killing bacteria, adherence, impaired lymphocyte function, glycosylation of C 3, which impairs phagocytosis, and an increased risk of bacterial and fungal infections. n cigarette smoking, chronic steroids, and prior surgery
Special wound healing problems n Gastrointestinal n stricture, anastomotic leak n Keloid, hypertrohpic scar n Marjolin ulcer-sqamous cell carcinoma n chronic wound n pressure ulcer n diabetec ulcer n venous stasis
Keloid and hypertrophic scar
Keloid and hypertrophic scar
Treatment of chronic wounds n Removal of non-viable tissue including: necrotic tissue, slough, foreign debris including residual material from dressings. n Removal of nonviable tissue is referred to as debridement. n Removal of foreign debris is referred to as cleansing. n 4 Types of Debridement Autolytic, Biochemical, Mechanical, Sharp
Wound etiologies n Arterial n Venous n Diabetic n Trauma n Surgical n Auto-immune n Pressure n Mixed
Chronic wound treatment n Debridement n Cleansing n Maintaining a moist environment n Preventing Further Injury
Debridement n Removal of ALL devitalized tissue n Not the Physical Therapy “Pick and Whittle” n Healthy bleeding tissue introduces beneficial platelets and Growth factors n Allows for thorough investigation of the wound n Remove potentially infected tissue n Obtain appropriate deep cultures
Debridement n Mechanical n Surgical – “Audible Bleeding ? ” n Enzymatic n Autolytic = Hydrogels, hydrocolloids, saline
Is there adequate blood flow to the ulcer? Arterial based wounds n Feel the pulse n Segmental pressures n Doppler examination n Waveforms n Can you examine the microvascular circulation?
Is there adequate blood flow from the ulcer? Venous Stasis Ulcers n Skin discoloration n Hemosiderin deposition n Stasis dermatitis n Lipodermatosclerosis n Loss of hair on the legs n Shiny skin on the tibias
Diabetes multifactorial Increased risk of infection Neuropathy (loss of protective sensation) Vascular effects Macrovascular ( trifurcation disease below the knee ) n Microvascular (affects medial layer to prevent vasodilatation) n Humeral (decreased NO) n n
Infections n Invasion by pathogenic microorganism n Nosocomial n Autoinfection n Virulence n Carriers n Opportunistic bacteria
Soft Tissue Infections n n n n cellulitis, intact blood supply Lymphangitis Erysipelas- cellulitis+lymphangitis subcutaneous abscess Impetigo-multiple intraepithelial abscesses Furuncle-sweet glands Carbuncle- subcutaneous tissue n perirectal abscess-fistula at anal crypt n distal phalanx of the finger (felon)
Erysipelas It is acute, non suppurative, spreading inflammation of the skin dt invasion of its lymohatics 1. 2. 3. 4. 5. 6. 7. Rose pink Hot Tense Tender Smooth Blanching on pressure Marked edema dt lymphatic obstruction
Erysipelas n Course n Resolution n Erysipelas migrans n Lymph edema n Gangrene and sloughing n Death n Treatment n Isolation n Rest and elevation n Icthyol or lead subacetate n penicillin
It is a staphylococcal infection originating in a hair follicle but involve the sc tissue and adjacent hair follicle Painful induraed swelling, red, hot & dusky Grow in all directions, central become soft & boggy then break with multiple discharging sinuses
Carbuncle
Gas Gangrene n It is an acute fatal rapidly spreading infection caused by a mixture of gas forming organisms of clostridia group n Predisposing n n n Bad general conditions Local ischemia In-adequte surgical wound care n Clostridial soft tissue include cellulitis and myonecrosis. n n Clostridium perfringens Cl nevyi Cl septicum Cl sordelli
Gas Gangrene Powerful exotoxin n Skin and SC tissue oedematous celluitis with gas that destroy local microcirculation n release RBCs and hemolysis n Early sacchrolytic----- hemolysis--- brick red n Late proteolytic--- H 2 + Fe---- iron sulphide--black color n n Muscles toxins lead to necrosis n Toxins generally
Gas Gangrene ( Clinical picture) n IP = 1 - 3 days n General n Toxemia and prostrtion n Stupor, delirium and death n Local n Brown watery discharge from wound and marked tenderness n Palpable crepitance. n Skin and muscle gangrene early brick red later black n X-rays show GAS
Gas Gangrene ( Clinical Types) 1. Fulminating 2. Massive ( whole limb) 3. Local ( muscle) 4. Gas edema 5. Gas abscess 6. Gas cellulites
Gas Gangrene Prophylaxis n Tetanus immunization n Anti gas gangrene serum 10 cm then 4 cm then 2 cm every 6 hours n Adequate surgical debridement prevents gangrene. n Immediate radical surgical Debridement. n Penicillin in massive doses
Gas Gangrene Active treatment n General Blood transfusion n O 2 therapy n Anti-gas gangrene serum 100 cm daily n Penicillin in massive doses or erythromycin n n Local n Debridement n Amputation
Tetanus n caused by enterotoxin secreted by clostridium tetani n 2 days to several weeks incubation n Complex prodromal symptom n Tonic phase Lockjaw. then Jaw stiffness n muscular contractions, tonic spasms n respiratory arrest n n Clonic phase
Tetanus 1. 2. 3. 4. 5. 6. 7. 8. 9. Acute tentanus Chronic Latent Cephalic Splanchnic Local Cryptogenic Post operative Tetanus neonatorum
Tetanus (DD) 1. Meningitis 2. Erysipelas 3. Tetany 4. Rabies 5. Strychnine poisoning 6. Local cause of trismus
Tetanus immunotherapy n Adults should receive booster toxoid doses at 10 -year intervals n Who do not have three prior toxoid injectionstetanus diphtheria toxoid (Td) n Tetanus immune globulin (TIG) ATS 1500 unit n ATG 250 IU n
Tetanus (treatment) n Nursing n Anti tetenic serum n ATS n n n 100. 000 u ½ IV and ½ IM 50. 000 U after 7 days ATG one dose only n Penicillin & streptomycin n Wound care n Other measure
Tetanus (treatment) n Stage I n Sedation by luminal or sparine n Stage II n Sedation n NG n Tracheotomy n Stage III n Muscle relaxant as curare 20 – 40 mg IV initial then IM n IPPV n NG tube n Continue till spasm disappear