SMOKING CESSATION Treating Tobacco Use and Dependence Public
 Public Health Department Faculty of Medicine UNPAD")
SMOKING CESSATION (Treating Tobacco Use and Dependence) Public Health Department Faculty of Medicine UNPAD

DR. Ardini Saptaningsih RAKSANAGARA dr. , MPH Date of Birth: 21 Mei 1960 Address : Jalan Pasang 26, Bandung-40114. Education 1986, Dokter : Fakultas Kedokteran, Unpad. 1992, Master of Public Health (MPH): University of Wollongong, Australia. 2004, Doktor : Pascasarjana, Unpad Work Experience 1987 - now : Lecture Public Health Department Faculty of Medicine Unpad 2007 - 2010 : Director Public Health Postgraduate Program Faculty of Medicine Unpad 2010 - 2011 : Head Department of Public Health Faculty of Medicine Unpad Ardini Saptaningsih RAKSANAGARA Jalan Pasang 26. Bandung 40114. Phone : 022 -7276326 Mobile phone : 0811 237 159 Email : araksanagara@yahoo. com

WHY IS TOBACCO A PUBLIC HEALTH PRIORITY ? • Tobacco Public Health Problem ! • Tobacco is the second major cause of death in the world.

• It is currently responsible for the death of one in ten adults worldwide (about 5 million deaths each year) • Tobacco is the fourth most common risk factor for disease worldwide

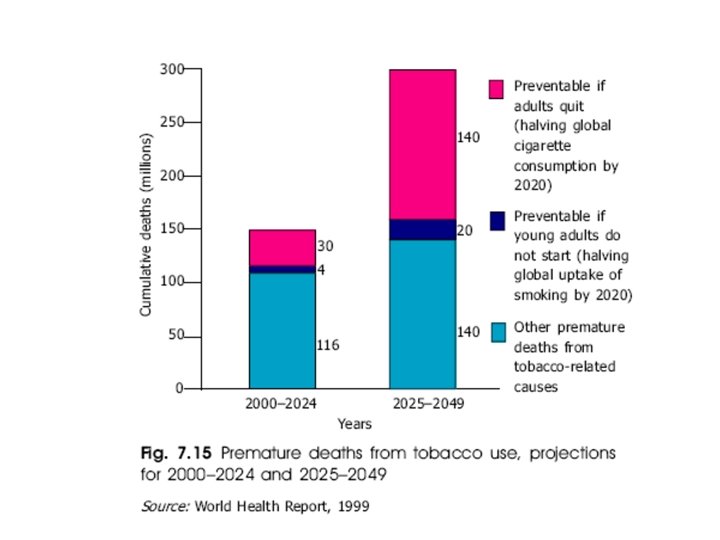
• If current smoking patterns continue, it will cause some 10 million deaths each year by 2025. • Half the people that smoke today – that is about 650 million people – will eventually be killed by tobacco.

WHY IS TOBACCO A PUBLIC HEALTH PRIORITY? • The economic costs of tobacco use are equally devastating. – high public health costs of treating – tobacco-caused diseases, – tobacco kills people at the height of their productivity, depriving families of breadwinners and nations of a healthy workforce. – Tobacco users are also less productive while they are alive due to increased sickness.

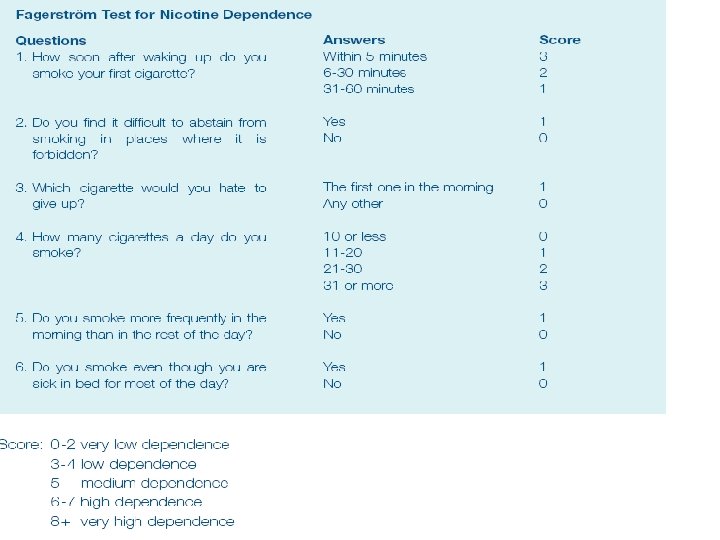
Every day, there will be patients come to your practice to consult about their symptoms/ diseases. Still, even though they will not complain about their smoking habits, you as a good doctor has to screen them for tobacco dependence as a routine procedure
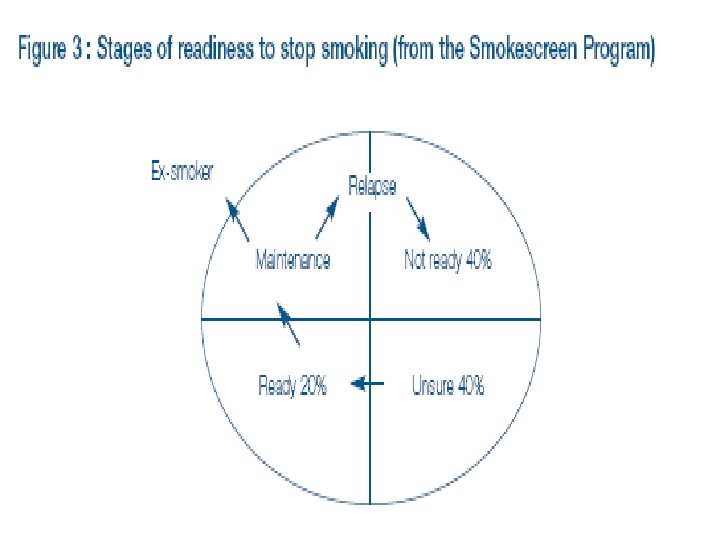

WILLINGNESS TO QUIT

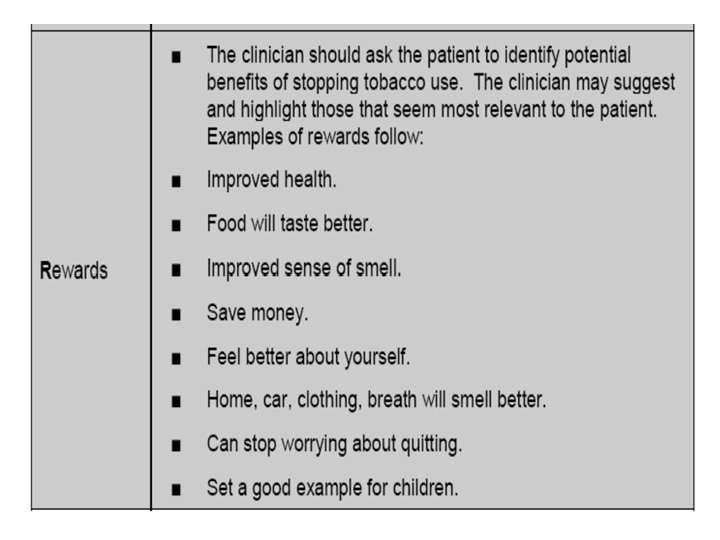
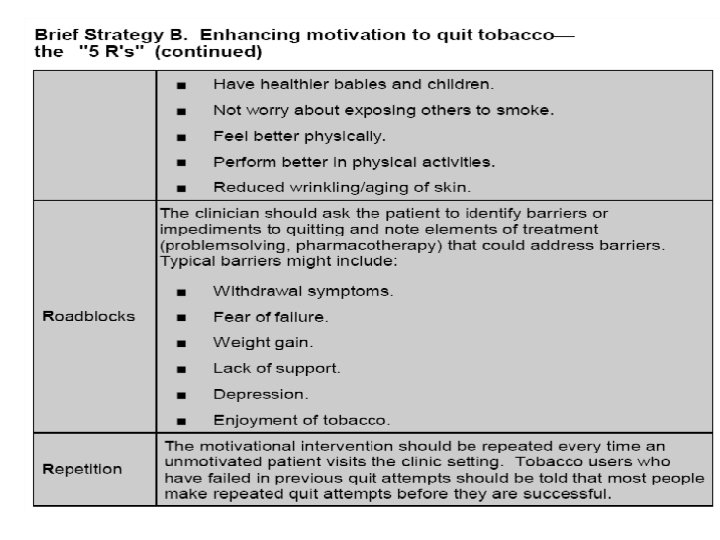
Unwilling to quit • 5 R’S – Relevance – Risks – Rewards – Roadblocks – Repetition

UNWILLING TO QUIT
")
Percentage of smokers (groups of age)

Everyday smokers • Male : 45 % • Female : 3 % • Urban : 21. 2 % • Rural : 25. 3 %

Household expenditure

• Smokers : 29. 2 % – M : 55. 7 % – F : 4. 4 % – Age 10 – 14 : 2. 0 % • No of cigarettes / day: 12 ( 8. 5 – 18. 5) – M : 11. 7 % – F : 15. 7 % – Age 10 – 14 : 10 % • Prevalence smoking in the house with member of family : 85. 4 %

Why tobacco ? • Harmful agent of harm • Cause of death – – – Responsible for 1 in 5 death (USA) Reduce life expectancy : 12 years Major killer of middle age Cause of 80 % cases of CHD Each year : • • Cancer deaths : 155, 000 Cardiovascular deaths : 122, 000 Chronic lung diseases deaths ; 72, 000 Others : 81, 000

Why tobacco control? • Illnesses caused by tobacco are completely preventable

Why progress difficult? • Tobacco industry • Economic self-interest : to get as many people to smoke as many cigarettes as possible

Reducing tobacco use • • • Educational Clinical Regulatory Economic Social or comprehensive

Educational • School based curriculum – Conducted in conjunction with community and media –based activity • Mass media or counter-advertising program • Media campaign change social norms around tobacco used – Decrease adolescent initiation – Increase adults cessation

Clinical • Pharmacologic • Behavioral Regulatory • Product manufacture – Filter, low tar – Promotion, marketing • Sale • Smoking restriction – Public venues – worksites

Economic • Modify taxation • Tariffs • Trade policy Comprehensive approach • Reduce demand supply

Consequences of Tobacco-Use: Preventable Causes of Death Smoking 400, 000 Accidents 94, 000 2 nd Hand Smoke 38, 000 Alcohol 45, 000 HIV/AIDS 32, 600 Suicide 31, 000 Homicide 21, 000 Drugs 14, 200

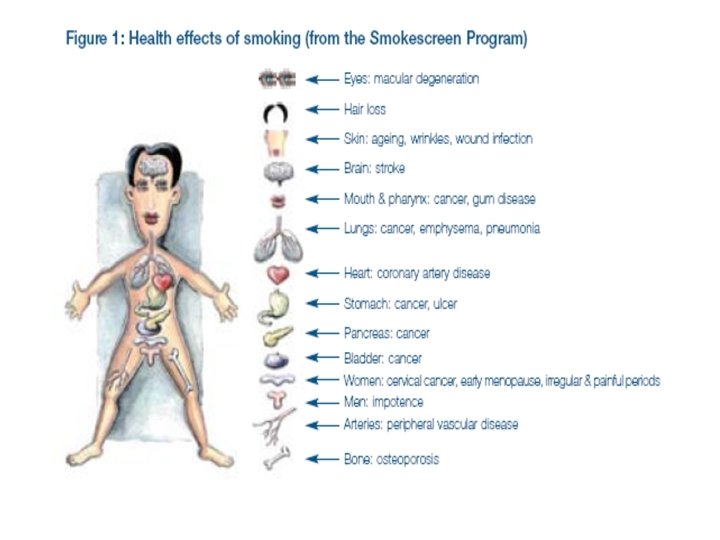
What are the tobacco-related diseases that are contributing to all these deaths?

Tobacco use: The single largest cause of preventable death.

Arteriosclerosis & Atherosclerosis: Healthy artery Damaged artery

Heart Attack: Smokers are twice as likely as Nonsmokers to have a heart attack Torn heart wall: Result of over-worked heart muscle Quitting smoking rapidly reduces the risk of coronary heart disease

Peripheral Vascular Disease

Stroke: This brain shows stroke damage, which can cause death or severe mental or physical disability

Emphysema: Emphysematic lung Healthy lung Symptoms Include «Shortness of breath «Chronic cough «Wheezing «Anxiety «Weight loss «Ankle, feet and leg swelling «fatigue

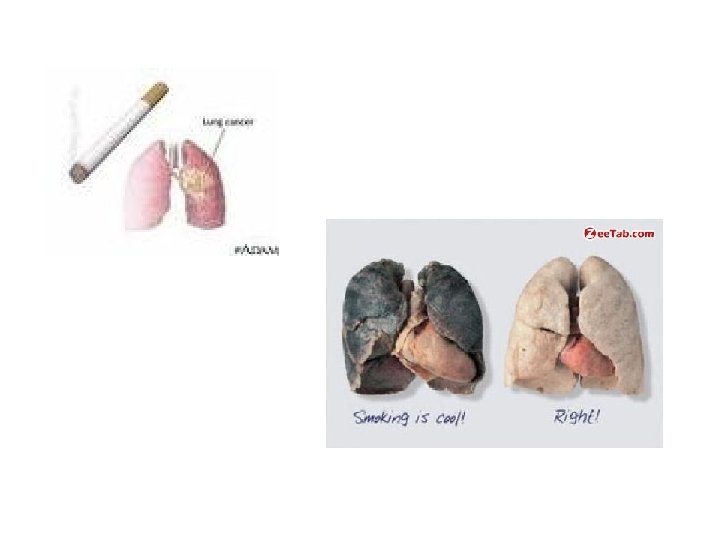
Lung Cancer: The uncontrolled growth of abnormal cells in one or both lungs Lung cancer kills more people than any other type of cancer

Fetal Damage: Fetal Smoking Syndrome: • Birth defects • Premature stillbirth • Low birthweight • Prone to Sudden Infant Death Syndrome • Lowered immune capacity

Laryngeal Cancer Symptoms: • Persistent hoarseness • Chronic sore throat • Painful swallowing • Pain in the ear • Lump in the neck Over 80% of deaths from laryngeal cancer are linked to smoking

Dental Problems: Common Consequences: • Stained teeth • Gum inflammation Above: Cavities • Black hairy tongue Below: Gingivitis • Oral cancer Overall poor oral health • Delayed healing of the gums

Consequences of chewing tobacco: Leukoplakia Oral cancer

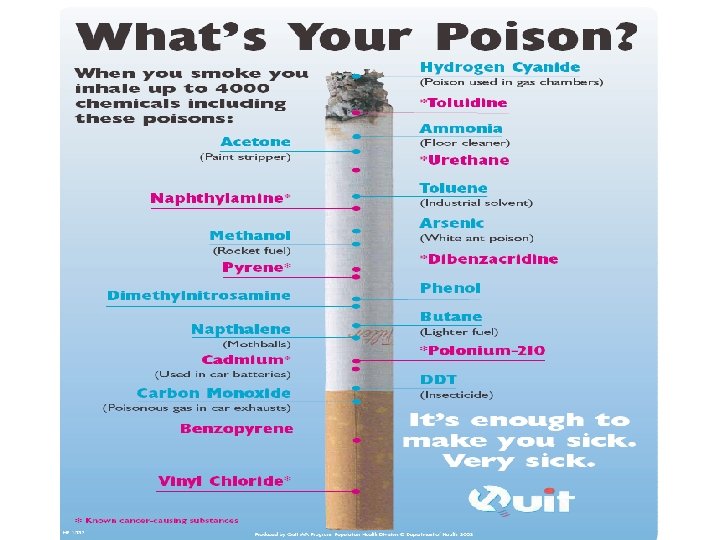
Chemical Box: What’s in Tobacco? « Tar: black sticky substance used to pave roads « Nicotine: Insecticide « Carbon Monoxide: Car exhaust « Acetone: Finger nail polish remover « Ammonia: Toilet Cleaner « Cadmium: used batteries « Ethanol: Alcohol « Arsenic: Rat poison « Butane: Lighter Fluid

If smoking is so bad for us, why do we start?

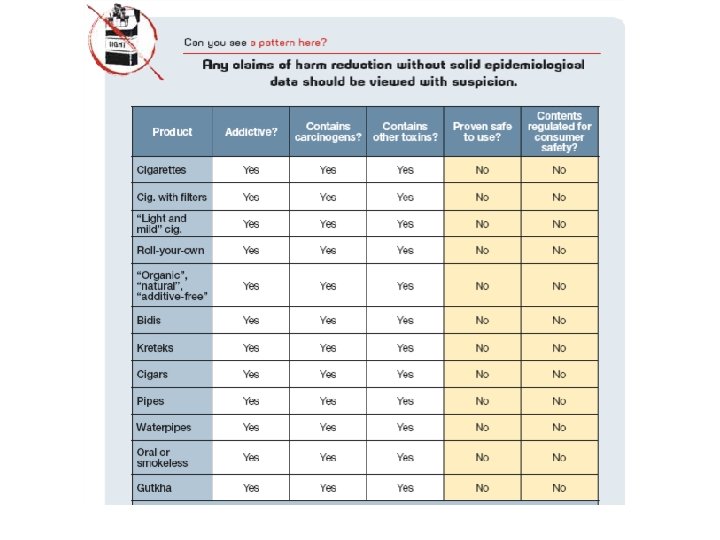
Tobacco Myths • Myth: Clove cigarettes are less harmful than regular cigarettes. • Myth: Cigars are safe • Myth: It’s OK to smoke as long as it’s a “natural” cigarette Conclusion: All tobacco products are addictive (which takes your independence away), cause cancer, and harm non-smokers all around you. The average tobacco user is addicted for seven years before they can finally kick this enslaving habit!

What is a cigar? « A cigar has larger amounts of tobacco than a « A cigar is tobacco rolled up in a tobacco leaf « A cigar does not have a filter cigarette

Cigar Use: Using beauty and fame to promote a dirty, devastating habit

Hookahs: • Not safer than regular tobacco smoke. • Causes the same diseases • Raises the risk of lip cancer, spreading infections like tuberculosis. • Users ingest about 100 times more lead from hookah smoke than from a cigarette.

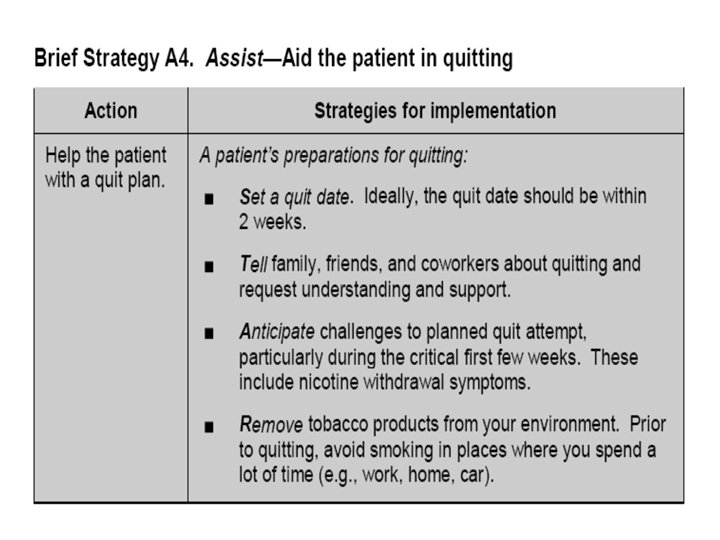
The Quit Plan: • Treat yourself well • Drink lots of water • Change your routines • Reduce stress • Deep breathing • Regular exercise • Do something enjoyable every day • Increase non-smoking social support • Other ideas?

Get Medication and Use It Correctly Talk to your health care provider about which medication will work for you: Available by prescription: • Zyban (Wellbutrin, Bupropion) • Nicotine Inhaler • Nicotine Nasal Spray Available over-the-counter: • Nicotine Patch (Has an increase in efficacy when combined with Zyban) • Nicotine Gum and lozenge

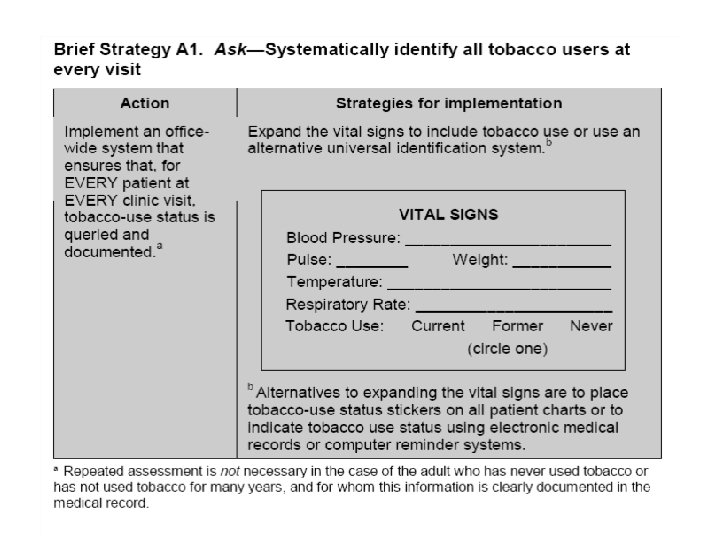
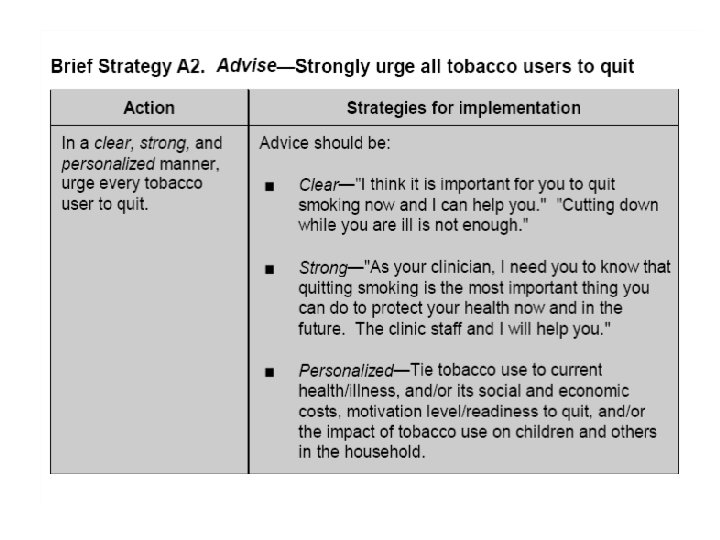
Conclusion • All patients should be asked if they use tobacco and should have their tobacco-use status documented on a regular basis. • Once a tobacco user is identified and advised to quit, the clinician should assess the patient’s willingness to quit at this time. • All physicians should strongly advise every patient who smokes to quit because evidence shows that physician advice to quit smoking increases abstinence rates. • Minimal interventions lasting less than 3 minutes increase overall tobacco abstinence rates.

• Proactive telephone counseling, group counseling, and individual counseling formats are effective and should be used in smoking cessation interventions. • All patients who receive a tobacco dependence intervention should be assessed for abstinence at the completion of treatment and during subsequent clinic contacts.

• Three types of counseling and behavioral therapies result in higher abstinence rates : (1) providing smokers with practical counseling (problem solving skills/skills training); (2) providing social support as part of treatment; and (3) helping smokers obtain social support outside of treatment. These types of counseling and behavioral therapy should be included in smoking cessation interventions.









Thank you
- Slides: 80