SMALL VESSEL VASCULITIDES Classification ANCAASSOCIATED VASCULITIS Small vessel



: necrotizing granulomatous inflammation, most often affecting")


 is the major target Ag")










 Myeloperoxidase (MPO/p-ANCA) Negative Wegener’s granulomatosis 70% 25%")





 Hypersensitivity vasculitis Cryoglobulinemic Vasculitis (CV) Hypocomplementemic Urticarial")
")

 Arthritis / Arthralgia 75% Abdominal pain")

")
")
 joint pain: NSAID Severe")

 #1 Idiopathic")
 Sparing palmar, plantar, mucosal surface")



- Slides: 40
SMALL- VESSEL VASCULITIDES
Classification
ANCA-ASSOCIATED VASCULITIS
Small vessel pauci-immune vasculitis Granulomatosis with Polyangiitis (Wegener’s): necrotizing granulomatous inflammation, most often affecting respiratory tract Eosinophilic Granulomatosis with Polyangiitis (Churg Strauss): occurs in association with asthma, eosinophilia, and necrotizing granulomatous inflammation Microscopic polyangiitis: occurs in the absence of asthma and eosinophilia with no evidence of granulomatous inflammation
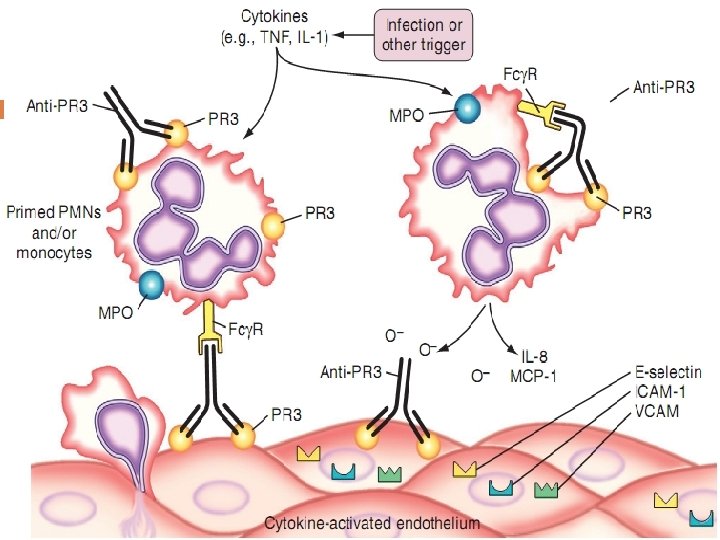
ANCA Anti-Neutrophil Cytoplasmic Antibodies Ab directed against proteins in the cytoplasmic granules of PMN’s and monocytes
c-ANCA Serum from patients bind to cytoplasmic granules and show a granular appearance on immunofluorescence Proteinase-3 (PR-3) is the major antigen Serine protease Present in azurophilic granules
p-ANCA Localized, peri-nuclear staining pattern on PMN’s Myeloperoxidase (MPO) is the major target Ag Elastase Cathepsin G Lactoferrin Lysozyme Permeability-increasing protein Only MPO has been convincingly associated with vasculitis, the others may be seen in other ANCA+ diseases (IBD, drugs, endocarditis)
Epidemiology Begin during the 5 th, 6 th, 7 th decades of life Male predominance Caucasians have greater incidence than African Americans Suspicion that Wegener’s more frequent in colder compared to warmer climates, and that microscopic polyangiitis has opposite trend
Clinical Manifestations
General symptoms Fever Malaise Anorexia Weight loss Myalgias Arthralgias
Upper and lower respiratory tract *Sinusitis, rhinitis, otitis media, ocular inflammation, Subglottic stenosis most common in Wegener’s, *Nodular or cavitary lesions in Wegener’s and Churg-Strauss *Pulmonary hemorrhage
Renal involvement *Less frequent in Churg -Strauss *Hematuria, proteinuria and renal failure *Renal failure usually has characteristics of rapidly progressive glomerulonephritis
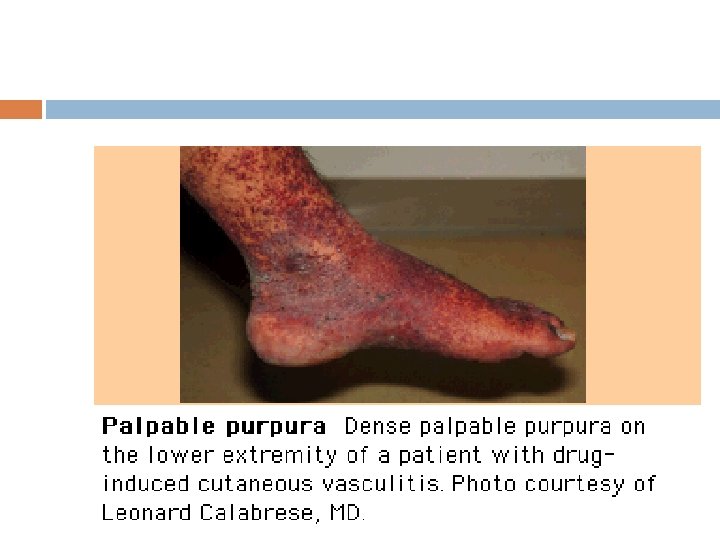
Skin *Purpura most common in lower extremities, occurs as recurrent crops. *Nodular lesions occur more frequently in Churg. Strauss and Wegener’s
Cardiac *Identified in 50% of pts with Churg-Strauss *<20% in Wegener’s and microscopic polyangiitis *Transient heart block, ventricular hypokinesis, infarction, myocarditis, endocarditis, pericarditis
Nerves *Peripheral: mononeuritis multiplex *Central: vasculitis within the meninges
Gastrointestinal *Typically abdominal pain, blood in the stool, mesenteric ischemia and rarely perforation *Can also mimic pancreatitis and hepatitis
Diagnosis
Anti-neutrophil cytoplasmic autoantibodies Proteinase 3 (PR 3/c-ANCA) Myeloperoxidase (MPO/p-ANCA) Negative Wegener’s granulomatosis 70% 25% 5% Microscopic polyangiitis 40% 50% 10% Churg-Strauss syndrome 10% 60% 30%
Pathologic diagnosis Biopsy of involved site Skin Muscle Nerve Gut Kidney
Treatment
Vasculitis: Treatment Remission induction: Cyclophosphamide 2 mg/kg po qd x 3 -6 months Prednisone 1 mg/kg po qd x 1 month, then taper Rituximab Remission maintenance (minimum 2 years) Methotrexate 20 -25 mg po q week + folate Azathioprine 2 mg/kg po qd Mycophenolate mofetil 1. 5 g po BID
Prognosis 5 -year patient survival is 45 -90% 10 -year patient survival is 75 -88% Patients with MPO-ANCA have slightly better renal outcome Patients with PR 3 -ANCA have more extrarenal organ manifestations, higher chance for relapse and higher mortality
IMMUNE COMPLEX SMALL VESSEL VASCULITIS
Immune Complex Vasculitis Ig. A Vasculitis (Henoch-Schönlein) Hypersensitivity vasculitis Cryoglobulinemic Vasculitis (CV) Hypocomplementemic Urticarial Vasculitis
Ig. A Vasculitis (Henoch-Schönlein)
Epidemiology The most common systemic vasculitis of childhood Age: 3 -15 y Incidence in children <17 y: 10 -20/100000 Incidence in adult: 13/ million Male/ Female : 1. 2/1 Black < White or Asian Winter & spring Etiology : Unknown 50% case due to URTI Vaccination Insect bites
Clinical Manifestation Palpable purpura (the most skin manifestation) Arthritis / Arthralgia 75% Abdominal pain 50% Renal disease 21 -54% Scrotum involvement 2 -38% Central & peripheral Nervous system Eye : (Keratitis , Uveitis)
Laboratory findings WBC ↑ ESR ↑ Serum Ig. A ↑ (in 50 to 70%) PLT & PT : normal U/A : RBC & WBC casts, proteinuria
DIAGNOSIS usually based on clinical manifestations Biopsy (skin or kidney)
TREATMENT No treatment is necessary in most patients (Conservative therapy) joint pain: NSAID Severe rash, nephritis, GI manifestation: Glucocorticosteroids
Hypersensitivity vasculitis Cutaneous Leukocytoclastic Angiitis
Epidemiology Incidence: Age: Female/Male : Etiology: 18 -30/million 37 -59 y (usually) #1 Idiopathic Drugs (NSAIDs, Penicillin, thiazides, Sulfonamides, …) Vaccination Infection
Clinical Manifestation skin involvement: palpable purpura (the most common) Sparing palmar, plantar, mucosal surface fever urticaria Arthralgias lymphadenopathy Visceral organ: (Renal, GI)
Laboratory findings ESR ↑ Complement ↓ ANCA –
TREATMENT Any causative medication should be discontinued Treatment should be aimed at the underlying infection Mild & without systemic organ involvement: no specific treatment severe or persistent skin disease not due to infection: corticosteroids colchicine antihistamines dapsone