Small Cell Lung Cancer SCLC Diagnosis Treatment and
: Diagnosis, Treatment and Natural History Gary L. Weinstein M.")

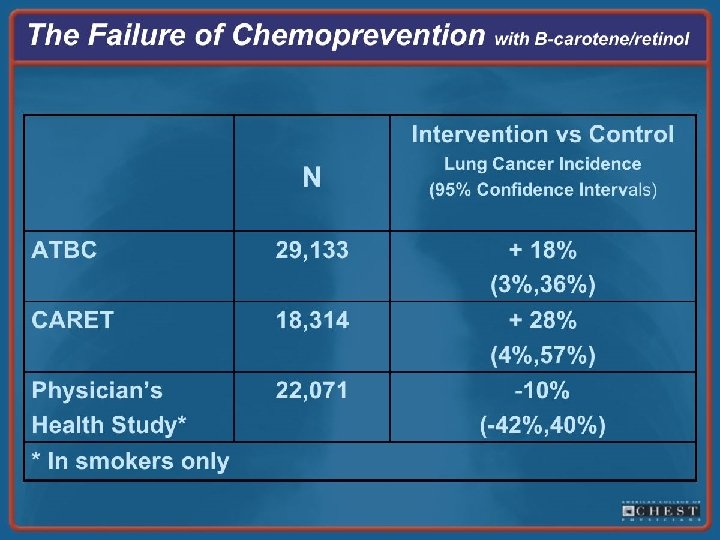

 • Considered highly responsive to “chems and beams” • BUT…usually relapses")
 WHO classification – Classical small cell carcinoma –")










- Slides: 55
Small Cell Lung Cancer (SCLC): Diagnosis, Treatment and Natural History Gary L. Weinstein M. D.
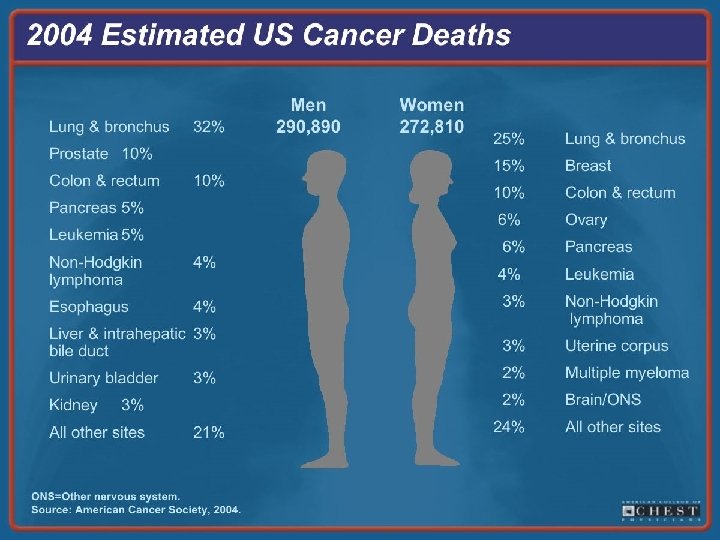
SCLC • Lung cancer epidemiology • SCLC – Pathology – Tumor markers – Genetics – Clinical course – Staging – Treatment
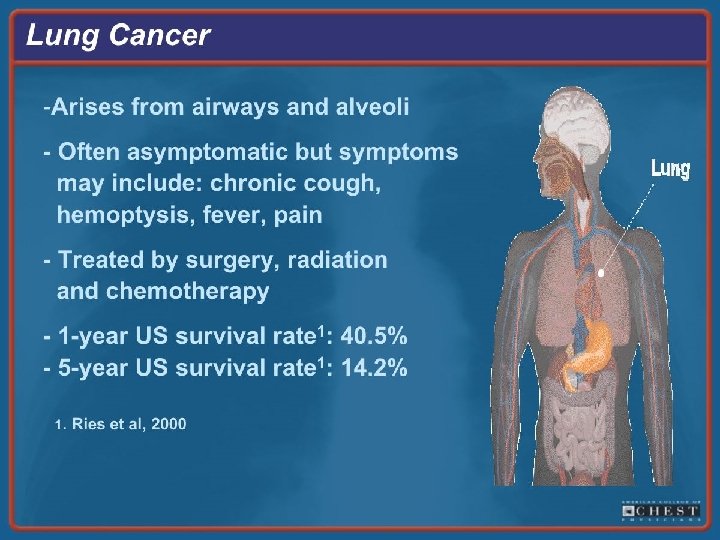
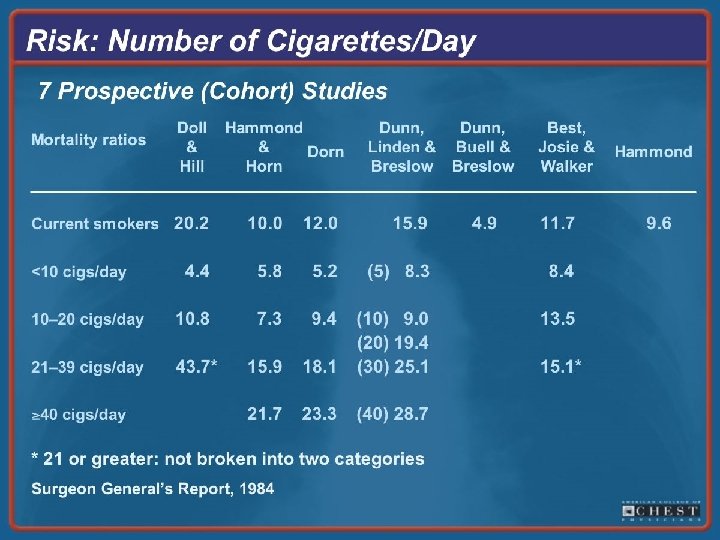
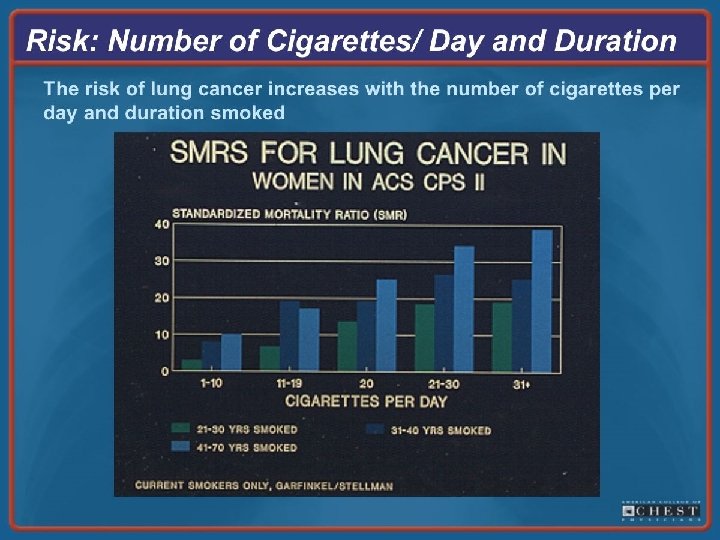
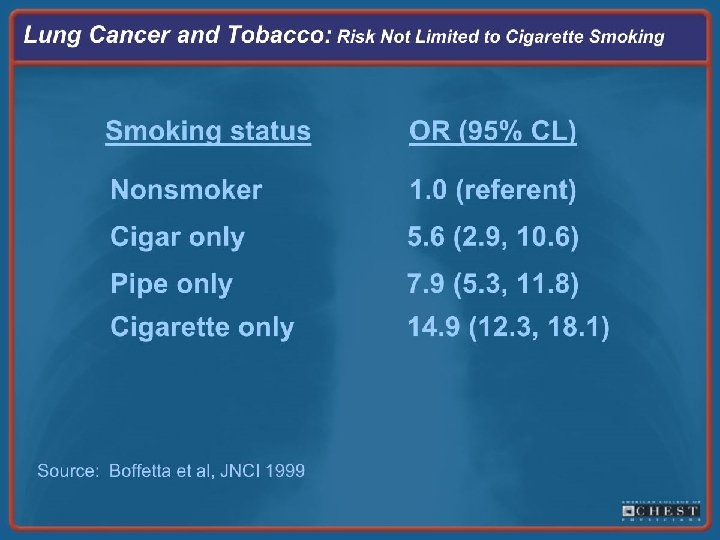
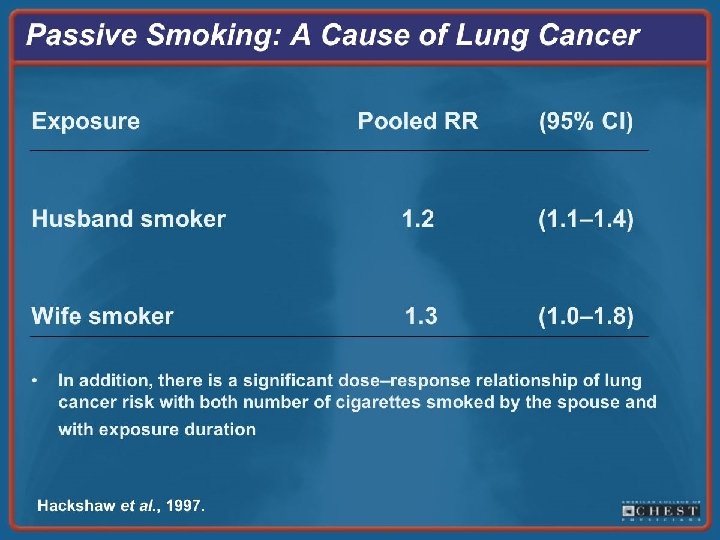
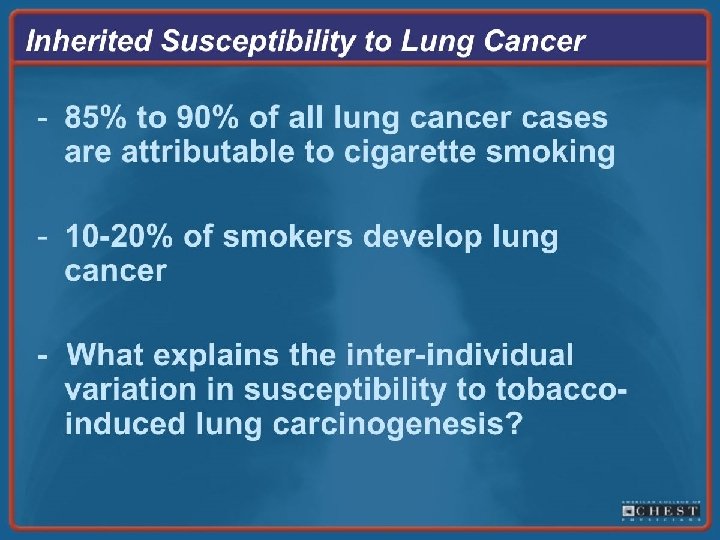
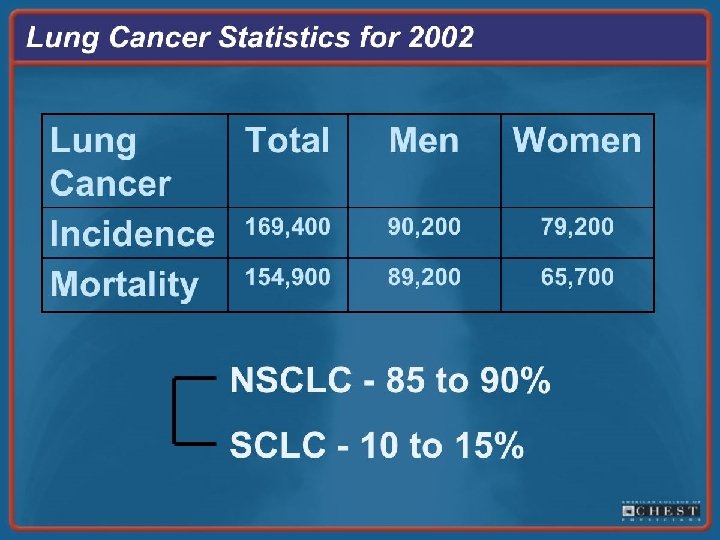
SCLC, factoids • 15 – 25 % of all lung cancers • Almost exclusively in smokers • Distinguished from NSCLC by: – Rapid doubling time – High growth fraction – Early development of wide-spread mets
SCLC, factoids (cont’d) • Considered highly responsive to “chems and beams” • BUT…usually relapses within 2 years despite treatment • Overall, only 3 – 8 % of all patients survive more than 5 years • Most common malignancy associated with Neurologic paraneoplastic syndromes
SCLC, pathology • Most recent (1999) WHO classification – Classical small cell carcinoma – Large cell neuroendocrine cancer – Combined small cell carcinoma with some NSCLC • Cells are approx. 2 X’s the size of normal lymphocytes
SCLC, pathology
SCLC, pathology
SCLC, clinical presentation • Typically arise centrally • Most common presentation is a large hilar mass with bulky mediastinal LAN • Common symptoms cough, SOB, wt loss • Approx. 70 % with overt mets at presentation • Commonly spread to liver, adrenals, bone and brain • Can present with paraneoplastic syndome
SCLC, tumor markers • 3 main groups: Neural, Epithelial, Neuroendocrine • Epithelial: virtually all SCLCs are immunoreactive for Keratin and Epithelial Membrane Antigen • 1 or more markers of Neural/Neuroendocrine differentiation found in approx. 75 % of SCLCs
SCLC, tumor markers – Leads to expression of dopa decarboxylase, calcitonin, neuron-specific enolase, chromogranin A, CD-56 (a neural cell adhesion molecule) gastrin releasing peptide and insulin-like growth hormone – Occasionally patients produce antibodies that crossreact with both the SCLC cells and the CNS cerebellar degeneration syndromes – SCLC cells can produce a number of polypeptide hormones including ACTH and Vasopressin
Neurologic Paraneoplastic Syndromes
Lung cancer, Paraneoplastic Syndromes
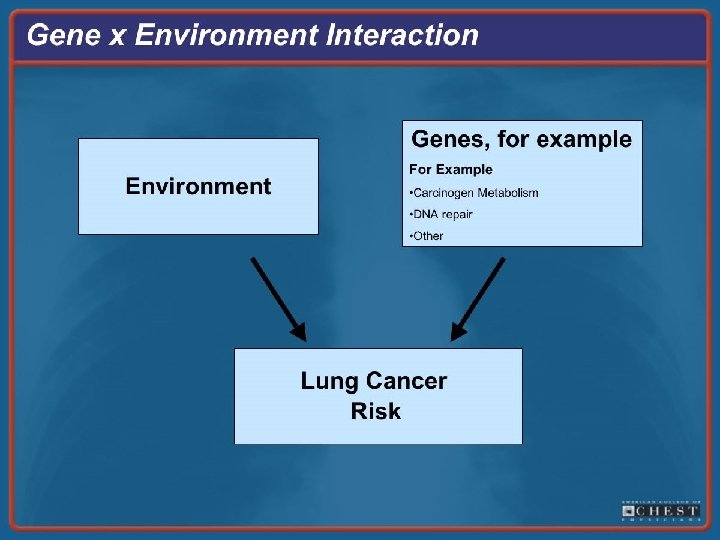
SCLC, genetics • Development of lung cancers occur through stimulation of proliferation and mutagenesis, occurring over YEARS and resulting from exposure to tobacco and other carcinogens
SCLC, genetics • The most common genetics of SCLC are: – P 53 mutation is present in 75 -90 % – Loss of heterozygosity of c-somes 9 p and 10 q in the majority – Deletion of 3 p inactivation of as many as 3 tumor suppressor genes – Loss of the retinoblastoma gene function is nearly ubiquitous – Activation of telomerase in approx. 90 % (allows cells to divide forever)
The End Questions?