SMALL BOWEL NECROSIS AFTER COLONOSCOPY Gastroenterology journal 2019

SMALL BOWEL NECROSIS AFTER COLONOSCOPY Gastroenterology journal 2019; 156: e 12–e 13

A 73 -year-old woman underwent surveillance colonoscopy for a history of colon adenomas. The colonoscopy was uncomplicated and remarkable for 3 small rectosigmoid polyps that were resected with cold biopsy forceps.

The patient was discharged home, and approximately 12 hours later she had the acute onset of lower abdominal pain and obstipation. She presented to the emergency department and on physical examination there was mild abdominal distension with tympany and lower abdominal tenderness to deep palpation.

Later that night, she developed tachycardia and tachypnea. Physical examination showed worsening abdominal distension and tenderness. Blood tests revealed new leukocytosis, lactic acidemia, and hypoalbuminemia.

CT of the abdomen and pelvis showed mildly dilated small bowel loops consistent with ileus. She was admitted to the surgery service and a nasogastric tube was placed to suction with bilious output.

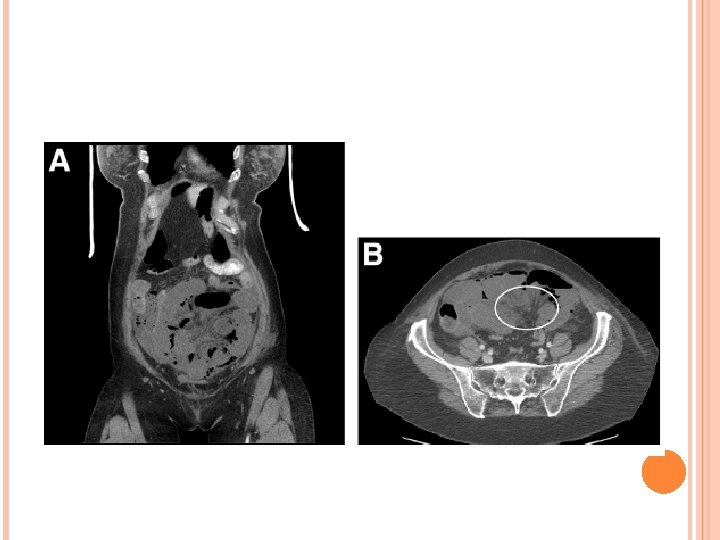
Repeat CT scans of the abdomen and pelvis showed persistently dilated small bowel loops and new pneumatosis intestinalis with pneumoperitoneum (Figure A, B).
.")
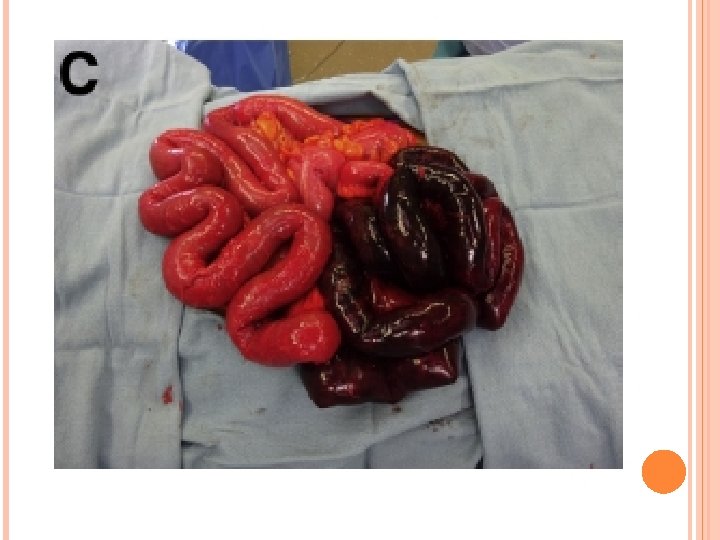
She underwent emergent exploratory laparotomy that revealed small bowel necrosis (Figure C).

Preoperative CT scans demonstrated evidence of small bowel obstruction and twisting of the mesentery in the left lower quadrant (Figure B, circle). Intraoperative findings demonstrated necrotic bowel internally herniated through an adhesion in the right lower quadrant from the epiploica of the sigmoid colon. There was no evidence of perforation.

There was clear demarcation between healthy and necrotic bowel, and 160 cm of necrotic small bowel were resected with primary anastomosis. Her postoperative course was complicated by peritonitis requiring treatment with antimicrobials, and she was discharged 10 days later.

Upon further questioning, she reported a severalmonth history of intermittent abdominal, right flank and right shoulder pain before colonoscopy that resolved after surgery.

We hypothesize that she had a preexisting symptomatic chronic internal hernia; small bowel then became strangulated through an adhesion, which may have been caused by insufflation and manipulation of the colon during colonoscopy. She followed up in surgery clinic 5 days after discharge where she overall felt well and was maintaining adequate oral nutrition.

Small bowel obstruction as a risk of colonoscopy is exceptionally uncommon. Small bowel obstruction after colonoscopy has previously been associated with both internal hernias and adhesions.

There was a single case of mesenteric torsion comparable with our current patient found in the medical literature, in which the patient was managed conservatively without a need for surgical treatment.

However, our case demonstrates that intestinal necrosis requiring intestinal resection may also be encountered. Awareness of this rare but potentially lifethreatening complication is critical in assessing any patient for postcolonoscopy complications.
- Slides: 16